
Abstract
Background
Nurses work at headache centres throughout Europe, and their care for migraine patients is acknowledged. However, the specific roles and tasks of nursing vary, and a unified understanding is lacking, posing challenges to knowledge sharing and research.
Objectives
Using an e-Delphi study method, the objective is to obtain healthcare professional headache experts’ opinions on nursing-specific roles and tasks and combine this into consensus statements for nurse recommendations for migraine treatment.
Methods
A three-round questionnaire study was conducted with nurses and neurologists from 18 specialised headache centres in 10 countries. In round 1, statements were compiled from a systematic examination of existing literature and expert opinions. In rounds 2 and 3, the experts rated the importance of statements (from round 1) on a 5-point Likert scale. Statements were analysed using a content analysis method, and the consensus of pre-defined statements was evaluated with gradually increased predetermined criteria using descriptive statistics.
Results
Twenty-one experts, representing all 10 countries, participated. The predetermined consensus of ≥70% agreement was reached for 42 out of the initial 63 statements. These statements formed the final recommendations within two themes: “The nurses’ roles and tasks in the clinical setting” and “The nurses’ roles and tasks in educating patients and colleagues.” The consensus level of statements was strong, with 40% receiving unanimous agreement (100%) and 97% achieving relatively high agreement (>80%).
Conclusion
Nursing plays a vital role with diverse tasks in migraine care. This study offers practical recommendations and a framework for nurses, equipping them with a clinical tool to enhance care and promote a coordinated approach to migraine treatment.
Introduction
Primary headache disorders constitute the most prevalent neurological disorder, and they represent a major public health concern worldwide (1). One of the most frequent primary headache disorders is migraine with a prevalence of around 15% among the adult population in Europe (2,3). For the individual, migraine can adversely affect every aspect of everyday life leading to decreased quality of life, withdrawal from social activities and reduced work- and functional capacity (3–6). Consequently, people with migraine seek general practitioners, neurologists, and specialised headache centres for treatment. Especially, specialised headache centres provide a bio-behavioural approach to meet both pharmacological and non-pharmacological needs (7–9). To provide comprehensive and effective treatment, it is recommended to adopt a multidisciplinary approach that involves various healthcare professionals, such as neurologists and nurses (7,8,10,11). This approach allows for a more comprehensive understanding of the different treatment elements and facilitates the delivery of optimised care to patients. By collaborating and utilising the expertise of multiple disciplines, healthcare professionals can enhance their ability to address the complex needs of patients and improve treatment outcomes.
At many European headache centres, nursing for migraine patients is a recognised and important part of care. Still, a unified understanding of the role of nurses and nursing specific tasks are not defined and unification of nursing across countries is lacking. The existing literature mostly includes studies from individual countries which focus on nursing in primary care settings. They concentrate on aspects such as nurse-led education for empowering patients to manage migraine (12,13), nurse administered screening for diagnosis of migraine (14,15), supervised nurse consultations (16,17), or costs and benefits of migraine nurses (18). The core fundamentals of nursing include: to engage in the promotion of health; to prevent illness; to give care to ill and disabled people; to provide healthcare teaching; to participate in research; and to supervise and train nurses and healthcare professionals (19). Experiences from international meetings in forums for headache nurses show that nursing of migraine patients is derived from the above definition and focuses on patient-centred themes, such as dialogue on living with a disabling disorder and the confronts for patients of coping with, and acceptance of, migraine. Other themes are on guidance and information including technical training on, for example, injections, as well as evaluation of treatment efficacy and the monitoring of side effects thereby strengthening compliance. All the above-mentioned points are important tasks underpinning the need for nurses at headache centres. Nevertheless, the tasks are handled in numerous ways, which can make knowledge sharing and research difficult and prevent development as well. Evidence and consensus on the nurses’ roles and which tasks should be conducted by nurses in headache centres, are still lacking, as well as standardised competencies for nurses. Enabling nurses to consult unified recommendations will strengthen the nurses professionally. Development of recommendations for nursing in migraine treatment will contribute to an improved patient care and standardised level of nursing across European headache centres.
Objectives
The objectives of this e-Delphi study are twofold; 1. To obtain healthcare professional headache experts’ opinions on which roles and tasks are associated with nursing in migraine treatment. 2. Through an iterative multi-staged process, to combine the opinions into consensus statements for the European nurse recommendations for migraine treatment.
Methods
Design
This European three- round e-Delphi study was conducted between May 2022 and May 2023 according to published protocol and with inspiration from the Guidance on Conducting and Reporting Delphi Studies (CREDES) and recommended criteria for Delphi studies (20–22). The study was registered at The Region of Southern Denmark (21/52885). According to The Regional Ethical Committee and Danish law, no additional approval was relevant (20212000-145). A written informed consent was obtained from all participants before inclusion in the study. All participants were informed that they can withdraw from the study at any time without giving a reason. The consent form and the questionnaires were completed electronically and stored anonymously in REDCap, a secure web application for building and management of online surveys (23). Elaborative methodological details are available in the protocol (22) and an overview of the study is summarised in Figure 1. Between each questionnaire round the steering committee reviewed and discussed data for feedback and questionnaires were edited accordantly before dissemination. Statements receiving consensus after the third round of questionnaires, were included in the final compilation of recommendations for nurse care in migraine treatment.

Study flow through the e-Delphi questionnaire rounds.
Participants
A purposive sampling technique was used to enrol experts from 18 specialised headache centres in Denmark, Estonia, Finland, Germany, Ireland, Netherlands, Norway, Sweden, Switzerland, and United Kingdom (24). Experts were defined as either nurses or neurologists co-working with nurses in specialised headache centres and had been identified through the fora of European Headache Federation (EHF) or the International Forum for headache Nurses (IFHN). To ensure a predominance of nurses in the expert panel, one neurologist and two nurses from each of the 10 countries were invited.
Eligible nurses had ≥2 years of experience working with migraine patients, worked at a specialised headache centre, were able to read and write English, and were willing to participate. Eligible neurologists have ≥2 years of experience in co-working with nurses at a headache centre, were able to read and write English and were willing to participate.
Round 1
The round 1 questionnaire had three sections: Demographic characteristics, Predefined statements from existing literature, and Expert opinions on nursing.
Demographic characteristics including age, gender, professional background, highest qualifications, nationality, academic/clinical experience, years of experience with migraine treatment and weekly hours working with migraine patients were collected. During the questionnaire development process, two authors (AVR and LSM) conducted a comprehensive examination of existing literature, encompassing both qualitative and quantitative research findings. The aim was to identify studies that had expressions and statements related to the roles and responsibilities of nurses in migraine treatment. These statements were utilised in the elaboration of the questionnaire for round 1. The databases Medline (PubMed), CINAHL, Web of Science, and EMBASE were searched using the search terms (subject heading and keywords) Nursing, Migraine, Nurs*, and Care. These searches were complemented by exploring publications identified through Google Scholar. The amalgamation of findings from various studies contributed to a deeper understanding of the nurses’ roles and tasks. The search was limited to English, adult populations, and peer-reviewed publications up to February 2022. There were 649 publications detected, which were screened by AVR and LSM for duplicates and selected based on the specific terms “nurs*”, “migraine”, and “care” in the title or abstract. Uncertainties were resolved by discussion and agreement between these authors. The 19 selected papers were thoroughly examined (AVR and LSM) for content related to nursing in migraine treatment, roles, and tasks. Drawing inspiration from Green and Thorogood, the authors synthesised prevalent themes emerging from the literature, by conducting a content analysis to identify codes and themes, with the two authors independently creating and synthesising code lists. From the analyses the authors extracted 25 statements grouped into four main domains: screening, communication, medication, and education and information (22,24–26). The expert panel rated each of the statements according to the level of importance using a 5-point Likert-scale (1=Not important at all – 5=Very important). In the third section of the questionnaire, the experts elaborated their opinions on nurses’ roles and tasks. The usage of both pre-defined statements and expert opinions reflected both the known evidence and the clinical practice providing a broad spectrum of ideas (27).
Qualitative data were handled using QSR international’s NVivo V12 and a content analysis was conducted for analysing the written communication in a systematic way (28). Inspired by the analytic steps of Graneheim and Lundman (25), the answers were read several times and, thereafter, analysed through an iterative multi-step process; 1. Detection of content; 2. Division of content into meaning units; 3. Coding units; 4. Interpretation of codes and formulating themes (25,26). This analytic approach enabled identification of content areas and combining or collapsing similar statements for the next questionnaire round (25,27).
Quantitative data were analysed in Stata18 and the extent to which the expert panel members shared the same opinion defined consensus (27). Since the Likert scale was considered an ordinal scale (29), consensus was statistically summarised using median (≥3) and interquartile range (IQR) (≤1.5) and percentage of agreement (≥60%) with responses rated important/very important.
Only statements, which received consensus in all three measures, were included in the next round.
Round 2
The round 2 questionnaire was distributed to all participating experts, regardless of any missing responses from round 1. Demographic information was collected for experts who had not completed the initial round (27). As part of the round 2 questionnaire the expert panel received graphical descriptive statistical feedback including median, interquartile range and percentage agreement on each of the statements reaching consensus in round 1. Using the 5-point Likert scale experts were given the opportunity to reconsider and potentially revise (30,31). Furthermore, statements emerged from round 1 were included for rating and open textboxes were provided for elaborative comments.
Again, qualitative data were analysed using content analysis to construct new or edit the existing statements (25). Quantitative data were evaluated using progressively increased criteria to strengthen consensus; median ≥3, IQR ≤1.5, and percentage agreement ≥65%.
Round 3
Statements achieving consensus in round 2 constituted the third-round questionnaire. All statements were discussed within the steering committee and analysed to collate similar statements. Furthermore, some of the statements were supplemented by elucidative questions concerning conduction of nursing tasks e.g.: “Nurses conduct independent consultations with patients” with the elaborative question: How should the consultations be held? (1=Face-to-face, 2=Consultation in clinic, 3=Phone call consultation, 4=Virtual consultation, 5=Not relevant, 6=Other).
Graphical descriptive statistical feedback from the previous round was presented and the experts were asked to re-rate the level of importance of statements as per round 2. Open textboxes were provided for explaining answers, but no new statements were obtained in this round. Data were analysed using gradually increased criteria; median ≥3.5, IQR ≤1, and percentage agreement ≥70%.
Results
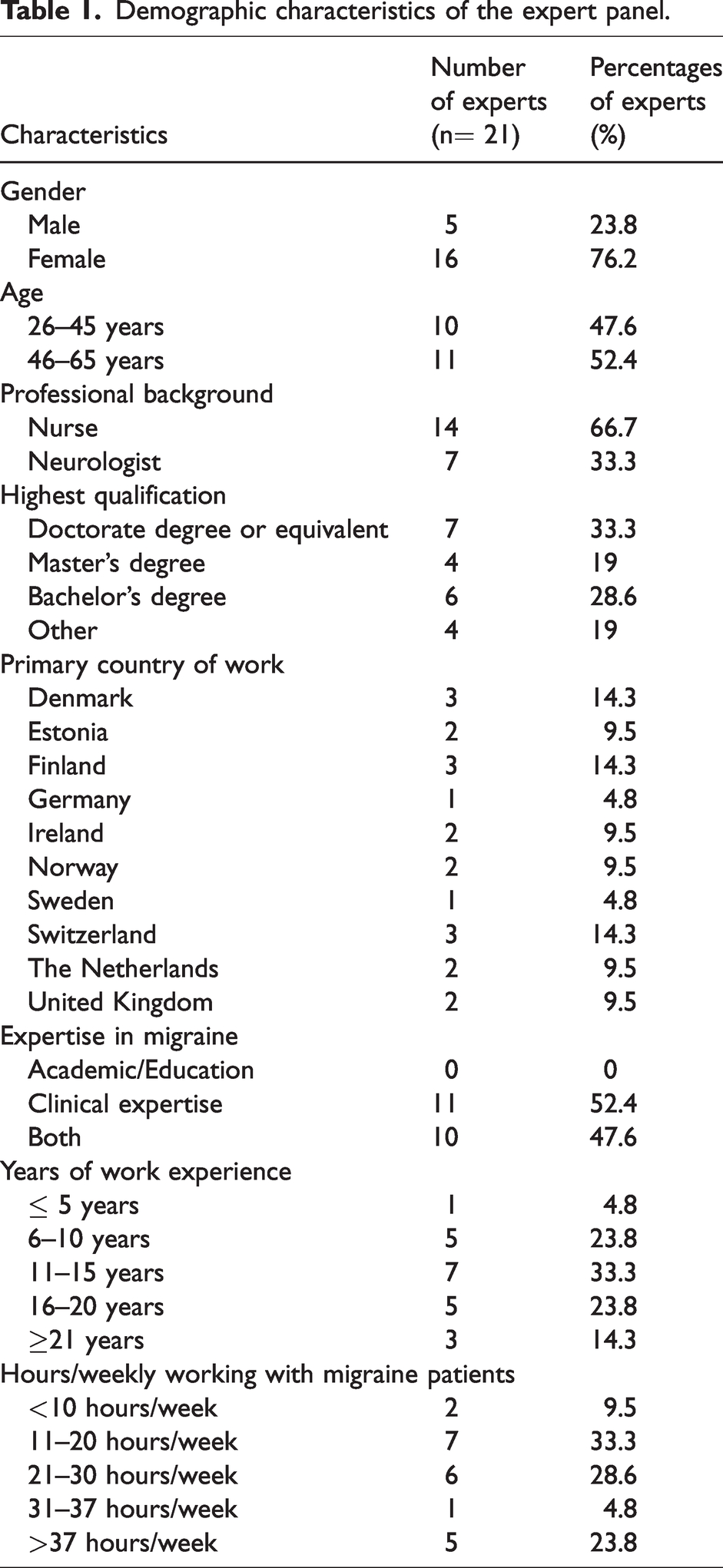
A total of 30 experts, 20 nurses and 10 neurologists, were identified and invited to participate in the study, of theses 21 (seven neurologists and 14 nurses) provided their consent and were consequently included in the study. Detailed demographic characteristics were collected, revealing representation from experts originating from all 10 countries. Predominantly, the participants were females, accounting for 76.2% of the experts, with the majority (66.7%) belonging to the nursing profession. Furthermore, the experts demonstrated a substantial level of experience in working with migraine patients, as more than 95% of them possessed over five years of experience, while 14.3% had more than 21 years of experience as outlined in Table 1.
Demographic characteristics of the expert panel.
Round 1
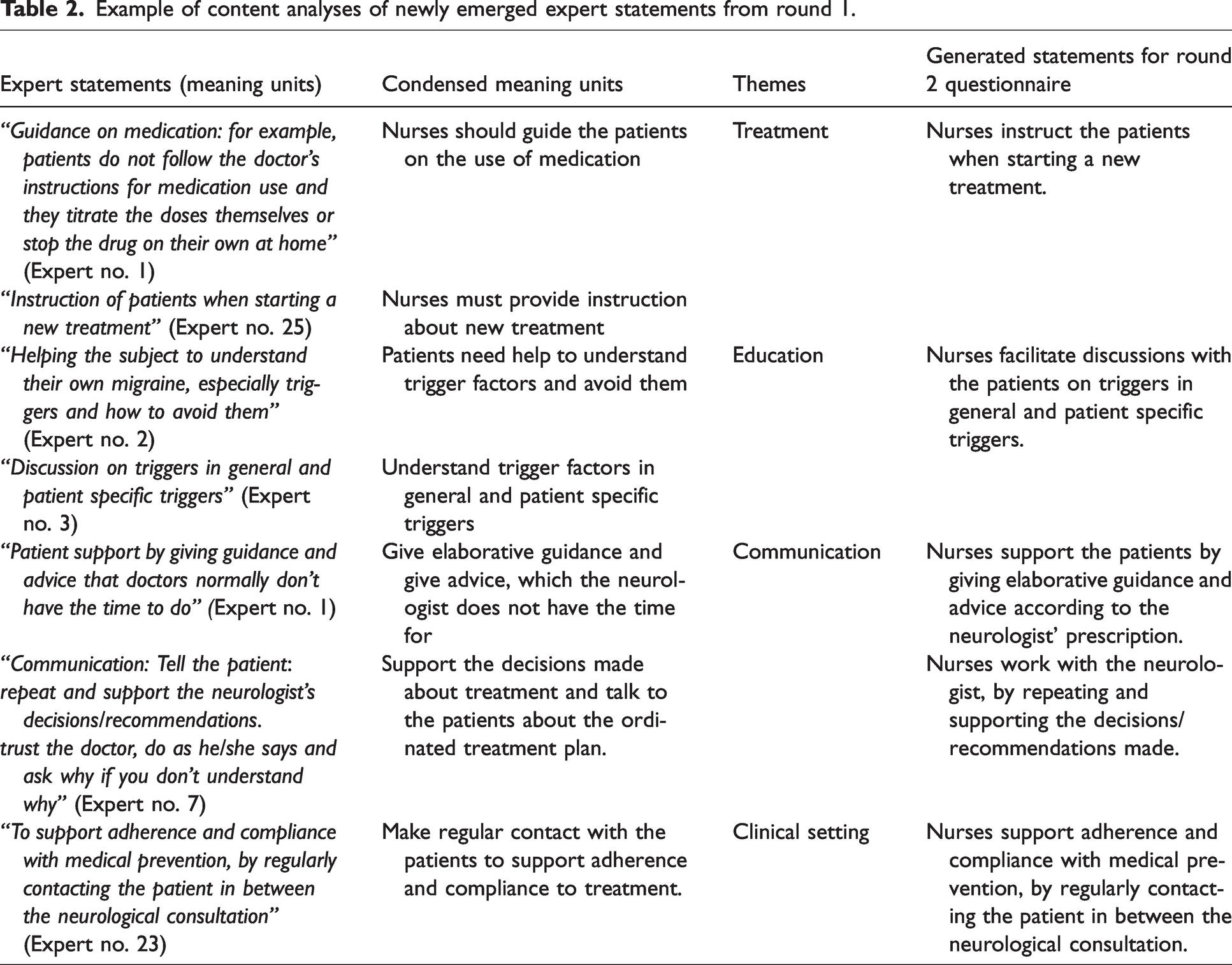
Twenty experts responded to this questionnaire corresponding to a response rate of 66.6%. Twenty-two of the 25 predefined statements from the literature search received consensus after this round and three statements were excluded as they did not reach consensus. Additionally, 38 new statements emerged from the experts’ opinions. A total of 60 statements were proceeded to round 2. (See table 2)
Example of content analyses of newly emerged expert statements from round 1.
Round 2
A total of 21 experts participated in this round, resulting in a response rate of 70%. Prior to the distribution of the third-round questionnaire, all statements with consensus were reorganised and categorised into two final overarching themes: Nurses’ roles and tasks in clinical setting (21 statements), and Nurses’ roles and tasks in education of patients and colleagues (21 statements). Eight statements were collapsed into existing statements due to similar content and wording. A total of 42 statements constituted the three-round questionnaire.
Round 3
Twenty-one experts successfully completed the questionnaire, resulting in a response rate of 70%. Following the completion of round three, consensus was achieved for all 42 statements, which formed the basis for the final recommendations as presented in Table 3. The level of agreement among experts was generally high, with 40% of statements receiving unanimous agreement (100%) and 97% of statements receiving high agreement (>80%). Online Supplemental Table S1 shows a total picture of all statements throughout all three rounds.
Statements receiving consensus after round 3.

IQR: Interquartile range, %: Percentage of experts rating the statements as important or very important.
The main results are divided into two overall themes covering the nurses’ roles and tasks in the clinical setting and in education of colleagues and patients, respectively. The results are illustrated in Figure 2 as a clinical working tool.

Clinical working tool of the recommendations.
The nurses’ roles and tasks in the clinical setting
The initial consultation with a nurse should encompass a thorough assessment of the patient’s headache history, covering details on headache characteristics, accompanying symptoms, frequency, intensity, duration, and medication usage. Furthermore, addressing patient expectations during this first consultation is central to aligning treatment plans with patient goals.
To enhance patient care and adherence, regular nurse-led consultations, scheduled regularly in between neurologists’ consultations are recommended. These consultations provide ongoing support and guidance, enabling nurses to offer explanations, advice, and instructions to promote treatment adherence. Nurse-led consultations are ideally conducted every three months, lasting for 30 minutes, either in person or virtually, with patients also having the option to initiate contact as needed. To ensure an organised approach when patients reach out, nurses are encouraged to implement a triage system involving initial contact, problem assessment, and urgency evaluation. Experts found a need for flexibility in nursing consultation frequency, which can vary based on the patient’s situation. For instance, consultations may be more frequent after initiating new treatment or following hospitalisation for migraine. Furthermore, the study emphasised nurses’ important role in supporting patients with medication overuse headache, suggesting e-consultations for addressing patient inquiries and counselling on withdrawal plans. Post-withdrawal consultations after two weeks are also recommended, the same supportive procedure is also recommended for patients experiencing potential medical side effects. At least once a year it is recommended that the nurses administer The Migraine Disability Assessment Scale (MIDAS) (32,33) and The Headache Impact Test (HIT-6) questionnaire (34,35) to monitor the treatment progress of patients.
Our findings demonstrate that nurses should collaborate with other healthcare professionals like neurologists, psychologists, and physiotherapists, where available, to ensure a holistic treatment approach. In relation to CGRP-Monoclonal Antibodies treatment (CGRP-mAbs), it is recommended that nurses instruct patients in techniques at start up and support with technical issues (autoinjector). More experienced nurses may also provide specialised treatments such as botulinum toxin, greater occipital nerve blocks, and/or the handling of neuromodulation devices.
The nurses’ roles and tasks in education of patients and colleagues
Experts reached a consensus that nurses play a crucial role in educating patients and colleagues about headache disorders, particularly migraine. To equip nurses for this task, they should actively seek knowledge through participation in national networks, teaching courses, online training, conferences, teaching courses, and research projects.
In patient education, a patient-centred approach is essential to enhance patients’ self-efficacy and empower them in managing their lives with migraines. This educational approach should cover various aspects, including general headache and specific migraine information, understanding migraine phases, identifying potential triggers, knowledge of medication usage (both acute and prophylactic), and awareness of over-the-counter medications and associated risks, including medication overuse headache. Explanation of proper headache diary completion is also stressed as a nursing task.
Nurses should also provide education on therapeutic options, such as relaxation techniques and behavioural factors affecting migraines (e.g., sleep patterns, water intake, caffeine consumption, and regular meals). Also, the importance of physical activity and addressing acceptance and denial behaviours should be part of the nurses’ education. Nurses can deliver this education through group sessions, individual consultations, written materials, or online resources.
Lastly, to support patients effectively, nurses should be knowledgeable about local guidelines, relevant literatures, and informative websites and be able to connect patients with patient associations to expand their support network.
Discussion
Experiences from daily clinics and international meetings in forums for headache nurses inspired this study. This three-round e-Delphi process has established a set of expert-based European recommendations for nursing in migraine treatment. The recommendations provide benchmarks as well as a clinical set of working tools to address nurse treatment (Figure 2).
The presented results emphasise the importance of nursing care in migraine treatment, which up to now, as mentioned earlier, has been sparsely described (7,8,11,13,36–39). The recommendations are evolved from the opinions of experts working at specialised headache clinics, however, we believe they are transferable to primary health care settings, as studies already confirm that nurses’ contribution in these clinics has a positive impact on migraine treatment (12,16,17). This study provides comprehensive insights into the multifaceted role of nurses and emphasises the important role of nursing tasks in assessments, patient-centred care and support of adherence and compliance to treatment plans. Furthermore, nursing extends beyond clinical care as it also includes education and support for patients undergoing specialised treatments, contributing to a holistic approach to migraine treatment. According to the recommendations of this study, nurses employed at headache centers are not merely an asset for better care but rather a necessity, given the multitude of important tasks and roles they fulfil in the treatments.
A crucial aspect of the first consultation with a nurse is the discussion of the patient’s expectations of treatment. Actively involving patients by using the shared-decision-making process, nurses enhance patient-centredness and increase treatment compliance (40). The open dialogue between nurse and patient fosters mutual understanding, aligning the treatment plan with the patient’s individual goals, preferences, and expectations. This was also concluded by Mose et al. in the study of medication overuse headache patients, where a close follow up resulted in an increase in compliance (41). Nurses are recommended to adopt flexible approaches in conducting consultations, which can be face-to-face, virtual, or via phone depending on the patient’s needs and preferences. Importantly, patients should have the possibility to initiate consultations when required, ensuring timely access to nursing support. The described variability in consultation set-up and content, driven by patient-specific circumstances such as the initiation of new treatments or hospitalisation due to migraine, stresses the need for adaptable nursing care. Here the set-up of a triage system allows for an organised approach, which could streamline the nursing response, ensuring that patients receive appropriate care in a timely manner. In their study of accessibility of migraine care, Wongsiriroj et al. concluded that having a dedicated nurse in clinic resulted in a positive impact on the use of triage for prioritisation of patients and also increased patient’s compliance to filling in the headache diary (11). Also, Steiner et al. stress the importance of a systematic approach in headache care to secure quality in the treatment of the headache patient (43).
In the present study, consensus was reached that the nurse should contact the patient every third month between consultations with the neurologist. It can be argued that many clinics do not have the resources to see their headache patients that often. The Federation of Neurological Societies (EFNS), now EAN, recommends follow-up of patients every third month (44–48).
Therefore, this would allow scheduling a neurologist consultation every sixth month with follow up by the nurse in between, i.e., after three months or when needed. This systematic set-up could decrease waiting time for patients and increase efficiency. In the study of follow-up telephone consultations for patients after eight and 16 weeks after initial visit, Carlsen et al. found that patients benefit from more efficient treatment and experience increased patient satisfaction (42). That said, it is also worth considering that patients will present with different needs. The study reached consensus that nurses must be available if patients have questions. Here both the patients and the clinic may benefit from open phone hours directly to the nurse or access to the nurse by e-consultation. The number of open hours depends on size of the clinic. Through open access the triage system is also valuable, when the nurse, in dialogue with the patient, assesses the need for follow-up. Not all patients will need a fixed appointment.
For migraine patients undergoing CGRP-mAb, nurses are recommended to provide instruction and support for proper technique, including the use of autoinjectors. Furthermore, experienced nurses can expand their roles to offer specialised treatments such as botulinum toxin, greater occipital nerve blocks, and management of neuromodulation devices, thereby broadening the array of therapeutic options available to patients. This has previously been suggested to accommodate the increasing need for headache specialised treatment (49). It is important to consider that the expansion of nurses’ responsibilities to include the specialised treatments mentioned depends on the local infrastructure in each country or even within each clinic. Further research is warranted in this regard, as the number of nurses in the present study is limited and might not be representative.
With regards to specialised treatments, this study does not mention the role of nurses being part of infusion centers as such centers are very rare in Central and Northern Europe. For example, given the novelty of nurses performing treatment with CGRP-mAbs, we were unable to find any studies related to this in the literature. Possibly, for the same reason, the headache specialists did not add the task as important in round 1.
Nurses should be able to conduct education, both in the context of patient-centred care and by dissemination of knowledge to colleagues. The recommendations highlight that achieving a standardised educational approach is not feasible. To ensure effective patient education, nurses could utilise a diverse range of educational methods. These may include group sessions, individual face-to-face consultations, or the distribution of written or online materials and handouts and depend on educational topic. Patient education is essential in headache management with focus on enhancing patients’ self-efficacy and empowerment, which is also confirmed in other studies (50,51). Patients should feel comfortable expressing their experiences and concerns related to migraines, as this information is invaluable for tailoring treatment plans to their individual needs, which is also a cornerstone in the study of Truglio-Londrigan and Slyer investigating shared-decision-making in nursing practice (40). The education for patients should cover a wide range of topics such as medical treatment, migraine specific characteristics, identification of trigger factors, and influence of behavioural factors on migraine patterns to ensure a well-rounded understanding of migraine management and to support patient adherence and compliance (52). Ford et al. showed that the discontinuation rate for patients treated with preventive medication was high and this was mostly due to side effects and lack of efficacy (53). Also, Hepp et al. confirm that the adherence to preventive medication is low and decreases over a year (54). This supports the findings in the present study which recommends that a supportive follow-up procedure is carried out by the nurse including guidance and advice if medical side effects are suspected. In addition to these topics, there was also consensus regarding the inclusion of information concerning the role of physical activity and relaxation techniques in managing migraines. This consensus is consistent with the conclusions drawn from a recent review conducted by Amin et al., indicating that regular physical activity may have a prophylactic effect on migraine frequency (55). Additionally, relaxation techniques have been identified as beneficial in the treatment of migraine (56,57).
It is important and necessary for nurses to educate their colleagues by sharing their knowledge and insights on headache disorders and treatment. This dissemination of information ensures that the entire healthcare team is well-informed and aligned in their approach to managing patients with migraines, which is also confirmed by Gaul et al. and Zeeberg et al. when they investigated the importance of multidisciplinary treatment (7,8). Also, Bhola and Goadsby acknowledged collaboration among healthcare professionals as it encourages a multidisciplinary approach to care (58). The study reached consensus that headache nurses should seek knowledge at for example national and international networks as well as participating in conferences and by participating and creating research projects. In the realm of headache research, it is a prevalent practice for nurses to partake in data collection. However, studies initiated by nurses themselves are relatively uncommon. It is imperative to emphasise the significance of this aspect for future research, which necessitates a change in the research culture in many countries. Nurse-led studies, however, will increase the awareness on the importance of the nurse as part of the treatment for headache and migraine patients.
Throughout the questionnaire rounds, several statements failed to achieve consensus and were subsequently excluded (see Supplementary Material file 1). Nonetheless, these excluded statements are referenced and deliberated upon below.
Both the initiation of a start-up consultation or a preliminary anamnesis via phone call and the utilisation of a screening questionnaire during the initial nurses’ consultation did not attain consensus among the experts. These statements originated from a systematic literature review conducted prior to round 1 and reflects practices observed within the primary healthcare sector, where the clinical framework differs.
Additionally, experts did not prioritise collective patient education by nurses alongside neurologists, nor did they consider educating families of migraine patients essential. Statements involving nurses administering National Acupuncture Detoxification Association (NADA) or acupuncture, and those related to cognitive therapy or mindfulness techniques, were also excluded. Concerning the clinical framework, statements regarding nurses adjusting medical treatment, conducting independent nurse-led clinics, and referring patients to specialists like psychologists lacked consensus. These statements emerged in round 1, highlighting variations in nursing responsibilities and clinical practices across countries. The lack of consensus often stemmed from a reflection of highly country-specific or clinic contexts.
Strengths and limitations
This study was carried out in accordance with pre-established criteria for consensus (22).
Statements were formulated based on existing literature and expert opinions, encompassing both empirical evidence and already established clinical practices. The predetermined statements in the initial round might introduce a potential for bias, however, it can be argued that these statements function as sources of inspiration and stimulate additional considerations from a clinical standpoint. Considering that the panel of experts represented healthcare institutions from 10 different countries, each characterised by unique clinical structures, the study encountered challenges. The expert-generated statements revealed variations in the perception of the nursing role across nations, which - we hypothesise - is mostly related to different clinical settings. However, as 42 statements received consensus among the experts, we conclude that patients’ needs are very similar across North and Central European countries, which is also confirmed by Bhola and Goadsby when they compared organisation of care at multiple headache centres worldwide (58).
Research and clinical implications
The development of standardised recommendations for nursing care in migraine treatment serves several purposes. First, it provides a framework for nurses to deliver high-quality care to migraine patients. Second, it enhances the consistency and continuity of care across different healthcare settings and countries. Third, it recognises the invaluable contributions of nurses to the multidisciplinary approach required for effective migraine management.
This study represents a crucial step by outlining expert-based recommendations for nursing care in migraine treatment, but also opens for several paths for future research and practice development. These include:
Implementation of Recommendations
Future studies should focus on the practical implementation of the developed recommendations within clinical settings. Assessing the feasibility and effectiveness of integrating these recommendations into nursing practice is essential.
Evaluation of Applicability
This study was carried out in Northern and Central Europe and does not include Southern European countries. It is necessary to evaluate the applicability of the recommendations in different clinical contexts and countries. Including Southern European countries in such evaluation studies will help identifying potential adaptations or modifications needed to accommodate specific clinical needs. This will secure that the results here represent a larger part of Europe, where other collaborations within the headache field already exist. The current formulation of certain recommended tasks, such as patient education, communication approach and content in consultations lacks specificity. Therefore, it would be beneficial for future studies to conduct a comprehensive investigation into the efficient execution of these tasks. Additionally, exploring the feasibility of aligning and standardising the description of these tasks across different countries would provide valuable insights.
Patient Outcomes
Research efforts should also concentrate on evaluating the impact on patients of nursing care, guided by these recommendations.
Interprofessional Collaboration
Further exploration of the collaborative dynamics between nurses and other healthcare professionals, such as neurologists, physiotherapists, and psychologists, in migraine care is needed.
Conclusion
In conclusion, this study establishes expert-based recommendations for nursing care in migraine treatment, encapsulating the core tasks and performance expectations for nurses in this specialised field. The recommendations highlight the decisive role of nurses in clinical management and education, emphasising their significance in headache centres. The recommendations define the role of the headache nurse and help define the headache nurses themselves, however, as mentioned, set-ups differ from country to country and even from clinic to clinic. Therefore, a structured education for and a formal definition of headache nurses are needed and would be valuable. Future research focusing on implementation of these recommendations in clinical settings and assessing their practical applicability can result in an important base for at structured headache nurse education and thereby nourish the continuous development of nursing care for migraine patients.
Article highlights
This study establishes expert-based recommendations for nursing care in migraine treatment, encapsulating the core tasks and performance expectations for nurses in this specialised field. This study provides a framework for nurses to deliver high-quality care to migraine patients. This study is the first to enhances consistency and continuity of nursing care across different healthcare settings and countries.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024241252161 - Supplemental material for Consensus recommendations on the role of nurses in headache care: A European e-Delphi study
Supplemental material, sj-pdf-1-cep-10.1177_03331024241252161 for Consensus recommendations on the role of nurses in headache care: A European e-Delphi study by Annette Vangaa Rasmussen, Rigmor Hoejland Jensen, Andres Gantenbein, Marja-Liisa Sumelahti, Mark Braschinsky, Susie Lagrata, Kristi Tamela, Jennifer Trouerbach-Kraan, Manjit S. Matharu, Veronica Dalevi, Hanneke Smits-Kimman, Signe Bruun Munksgaard, Johannes Tröndle, Maren Østergaard Eriksen, Gøril Bruvik Gravdahl, Camilla Nellemann Larsen, Esther Tomkins, Marja Hassinen, Lise Rystad Øie, Leena Eklund Karlsson and Louise Schlosser Mose in Cephalalgia
Footnotes
Acknowledgements
The authors especially would like to thank H. Lundbeck A/S for the research grant. The authors also want to thank OPEN, Open Patient data Explorative Network, Odense University Hospital, Region of Southern Denmark for assistance. Finally, the authors would like to thank all experts for their valuable knowledge sharing and goodwill in participating.
Authors’ contributions
A.V.R and L.S.M designed the study. All authors contributed to the writing and revising of the manuscript and approved the final manuscript.
Availability of data and materials
The datasets generated during and/or analysed during the current study will be made available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.V.R. has received honoraria from Lundbeck and Eli Lilly for Advisory Boards and written compendium; R.H.J. has received honoraria for lectures and patient leaflets from MSD, Berlin-Chemie Menarini, ATI, and Pfizer and participated in medical advisory boards for ATI and Electrocore and conducted clinical trials for Eli-Lilly and ATI; A.G. has received honoraria for lectures or consulting from AbbVie, Almirall, Biogen, BioMed, Curatis, EliLilly, Lundbeck, Neurolite, Novartis, TEVA/Mepha; S.L. received fees for attending advisory meetings, presentations and preparing presentation materials from AbbVie, TEVA, Eli Lilly, Tillots Pharma, Salvia and Novartis; M.S.M. is chair of the medical advisory board of the CSF Leak Association, serves on the advisory board for Abbott, AbbVie, Eli Lilly, Salvia, Lundbeck, Pfizer and TEVA, has received payment for the development of educational presentations from AbbVie, Eli Lilly, Lundbeck, TEVA and Pfizer; S.B.M. has received travel grants from Lundbeck, TEVA, AbbVie and for Advisory board for AbbVie, Lundbeck, Novartis, TEVA; M.H. received funding for travel and/or speaker honoraria from TEVA, Lundbeck and compensation for advisory service or producing educational material from TEVA, Lundbeck and Novartis; All other authors have declared no conflict of interests.
Ethics approval and consent to participate
The study is registered at The Region of Southern Denmark (21/52885). According to The Regional Ethical Committee and Danish law, no additional ethical approval was relevant (20212000-145). A written informed consent was obtained from all participants before inclusion in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: H. Lundbeck A/S funded this study with a research grant. H. Lundbeck A/S has not been involved in the design, conduction or writing this nor any related manuscripts.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.