
Abstract
Background
Migraine-attributed burden, impact, disability and migraine-impacted quality of life are important concepts in clinical management, clinical and epidemiological research, and health policy, requiring clear and agreed definitions. We aimed to formulate concise and precise definitions of these concepts by expert consensus.
Methods
We searched the terms migraine-attributed burden, impact, disability and migraine-impacted quality of life in Embase and Medline from 1974 and 1946 respectively. We followed a Delphi process to reach consensus on definitions.
Results
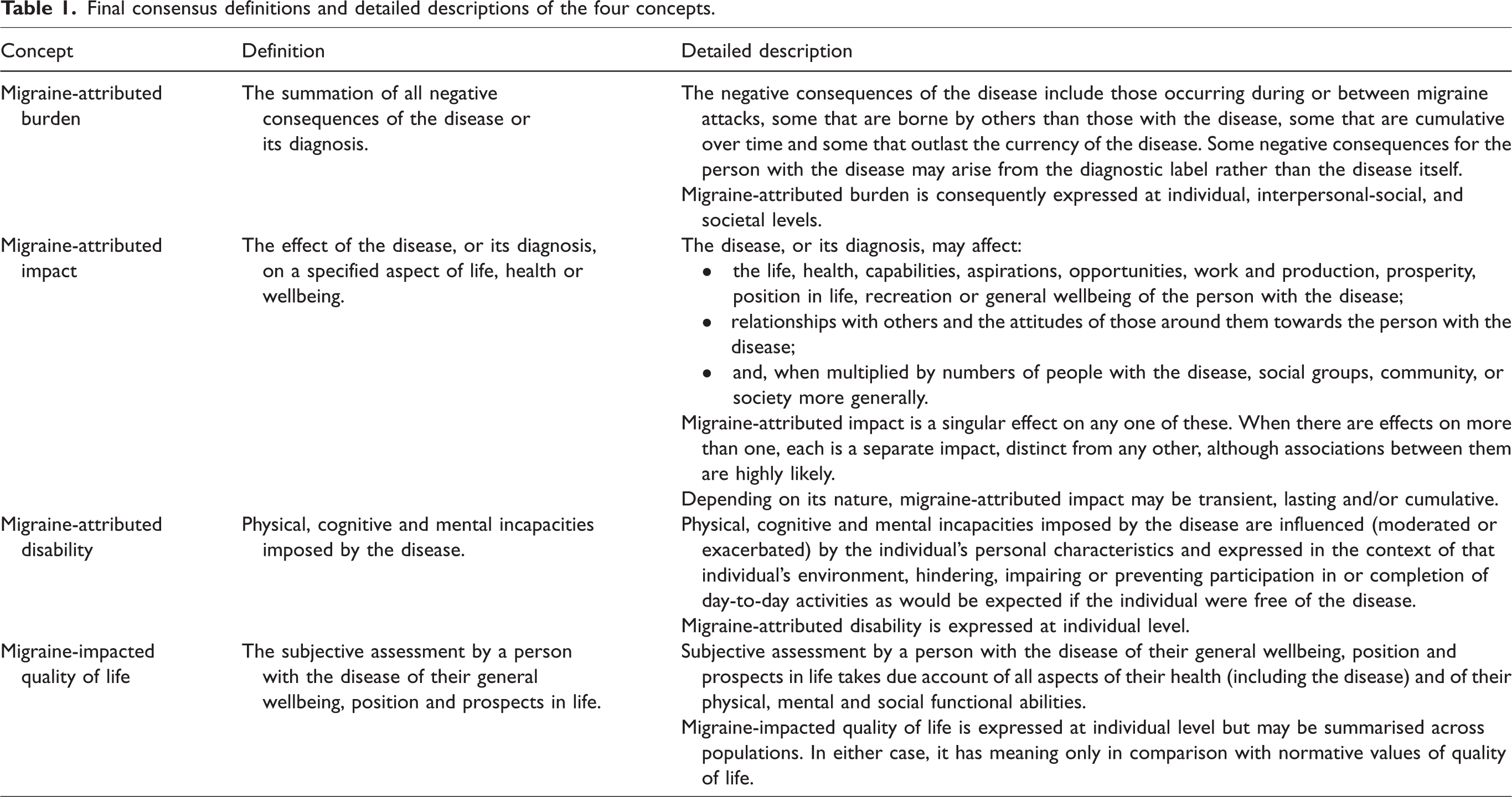
We found widespread conflation of concepts and inconsistent terminology within publications. Following three Delphi rounds, we defined migraine-attributed burden as “the summation of all negative consequences of the disease or its diagnosis”; migraine-attributed impact as “the effect of the disease, or its diagnosis, on a specified aspect of life, health or wellbeing”; migraine-attributed disability as “physical, cognitive and mental incapacities imposed by the disease”; and migraine-impacted quality of life as “the subjective assessment by a person with the disease of their general wellbeing, position and prospects in life”. We complemented each definition with a detailed description.
Conclusion
These definitions and descriptions should foster consistency and encourage more appropriate use of currently available quantifying instruments and aid the future development of others.
Introduction
Migraine impairs health, disables those affected, and impacts their wellbeing. Evidence of this is supplied by many sources (1 –10). Among these, the Global Burden of Disease (GBD) studies have reiteratively ranked migraine as the second highest single cause of years lived with disability (YLDs) worldwide (8 –10).
The evidence from GBD is particularly compelling, but in the context of our study – concerned with definitions – it calls for considered interpretation. While GBD’s stated purpose is to estimate burden attributed to all diseases, enabling these to be ranked for the purpose of informing health policy (11), the expression of non-fatal burden in YLDs is not conceptually coherent. Firstly, non-fatal burden is not wholly quantifiable by a measure of disability. Secondly, YLDs are not in any case a measure of disability but of disease-attributed health states ranked according to public preferences for one health state over another (12). YLDs better reflect lost health due to disease (12), which may indeed approximate to the concept of burden of disease, but the latter is a much more complex construct than disability, and certainly not synonymous with it.
In the vocabulary of migraine, burden, disability, impact and quality of life are important concepts. They are quantifiers, guiding clinical management of the disorder and informing clinical and epidemiological research into migraine and health policy (13,14). There is a complex relationship between them, which is to some extent hierarchical, with burden correctly regarded as an overarching construct subsuming the others (13).
However, the literature addressing these concepts often distinguishes poorly or not at all between them, sometimes using the terms as though synonymous. Whatever conceptual confusion and disagreements lie behind this, they need to be resolved for the benefit of care, research and health policy. To this end, the terms require clear and credible definitions, whether they are to be applied at individual or population levels. These do not currently exist. Our objective, therefore, was to formulate such definitions by expert consensus.
Methods
Panel of experts
Prior to initiation of this work, Eli Lilly and Company established a ten-member multi-stakeholder working group, including experts in various aspects of headache medicine, representatives of patient advocacy groups and policy makers, to support actions to improve management of migraine in Europe. The group identified barriers to care and proposed remedial initiatives, of which this is one, with members then deciding in which initiatives they wished to participate.
All eight authors constituted the expert panel for this work. TJS, GMT, ZK, PPR, ARG and CT were members of the multi-stakeholder working group and participated as headache specialists with expertise in clinical practice, research, headache terminology and nosography, and/or headache epidemiology. GDA and SLR brought expertise in clinical research and/or headache terminology and nosography, and contributed to the project methodology.
Literature search and screening of records
Two authors (GDA and SLR), along with one other employee of Eli Lilly and Company outside the authoring team (AF – see acknowledgements), searched Embase and Medline for publications addressing any of migraine-attributed burden, impact or disability, and migraine-impacted quality of life, published from 1974 or 1946, respectively, up to May 2021. Details of the search terms and syntax are provided in Supplementary Material 1. Relevant reviews, editorials, concept papers and commentaries were identified from this search through the following procedures. Records were screened by GDA and SLR to remove duplicates and select those including the terms “burden”, “impact”, “disability” and/or “quality of life” in the title and/or abstract. From their full texts, publications were selected that focused on any of these associated with migraine. Primary research publications, and papers focused on financial cost (at individual or societal levels), on comorbidities of migraine as predictors of disability or burden rather than migraine itself, or on validation of scales, were excluded as outside the scope of our study. Uncertainties were resolved by discussion and agreement between these authors.
Selected papers were reviewed in full by GDA and SLR. Each was screened for descriptions of migraine-attributed burden, impact and disability, and migraine-impacted quality of life. Listings were generated, per paper and per concept, of the topics referenced as part of each concept’s description, and findings were summarised, per concept, as lists and frequencies of across all selected papers.
Formulation of definitions
We used the widely accepted Delphi method (15) to achieve consensus between all eight authors. Since the covid-19 pandemic prevented travel, we met virtually and conducted rounds by email.
For the first round, lists of candidate items identified by GDA and SLR through the literature search and to be considered in the definitions of each concept were pre-circulated (Supplementary Material 2, Table S1). Each member of the expert panel scored each item with regards to correspondence to the concept in question (1: does not correspond; 2: relevant but not critical; 3: directly corresponds and critical) and to clarity (1: unclear; 2: needs revision; 3: clear). There was opportunity in this round to comment. Responses were sent to a facilitator (PF – see acknowledgements) outside the authoring team who anonymised them before sending to SLR for collation. Items were retained when there was >70% agreement on correspondence (including scores of 2 and 3), or otherwise omitted. This agreement level was closely aligned with the median threshold reported across 25 Delphi studies (16) and was used in a previous Delphi study to achieve consensus on another definition (17). Issues around clarity, and comments suggesting items that might be missing, were addressed by rephrasing and revising according to this feedback.
The second Delphi round presented proposed definitions, formulated by GDA and SLR, that best represented all authors’ expressed opinions. Participants responded “yes” or “no”, in agreement or otherwise with each proposed definition (Supplementary Material 2, Table S2). As in Round 1, responses were sent to a facilitator (PF – see acknowledgements) outside the authoring team who anonymised them before sending to SLR for collation. SLR shared the anonymised results with all authors.
In the third round, conducted as a virtual group discussion with follow-up email correspondence, dissenters in the second round (those responding “no”) justified and defended their responses in open forum to resolve disagreements through debate and thereby reach consensus (Supplementary Material 2, Table S3).
Results
Screening of records from the literature search
The initial search yielded 1,584 records. Screening of titles and abstracts reduced these to 280, of which 240 were excluded upon inspection of their full texts (Figure 1). From the texts or reference lists of 39 of the 40 remaining publications (full text was unavailable for one), an additional 7 relevant publications were identified. A total of 46 papers were therefore included in the analyses, published over 28 years (1994–2021) (3,7,8,18–60) (Figure 1).
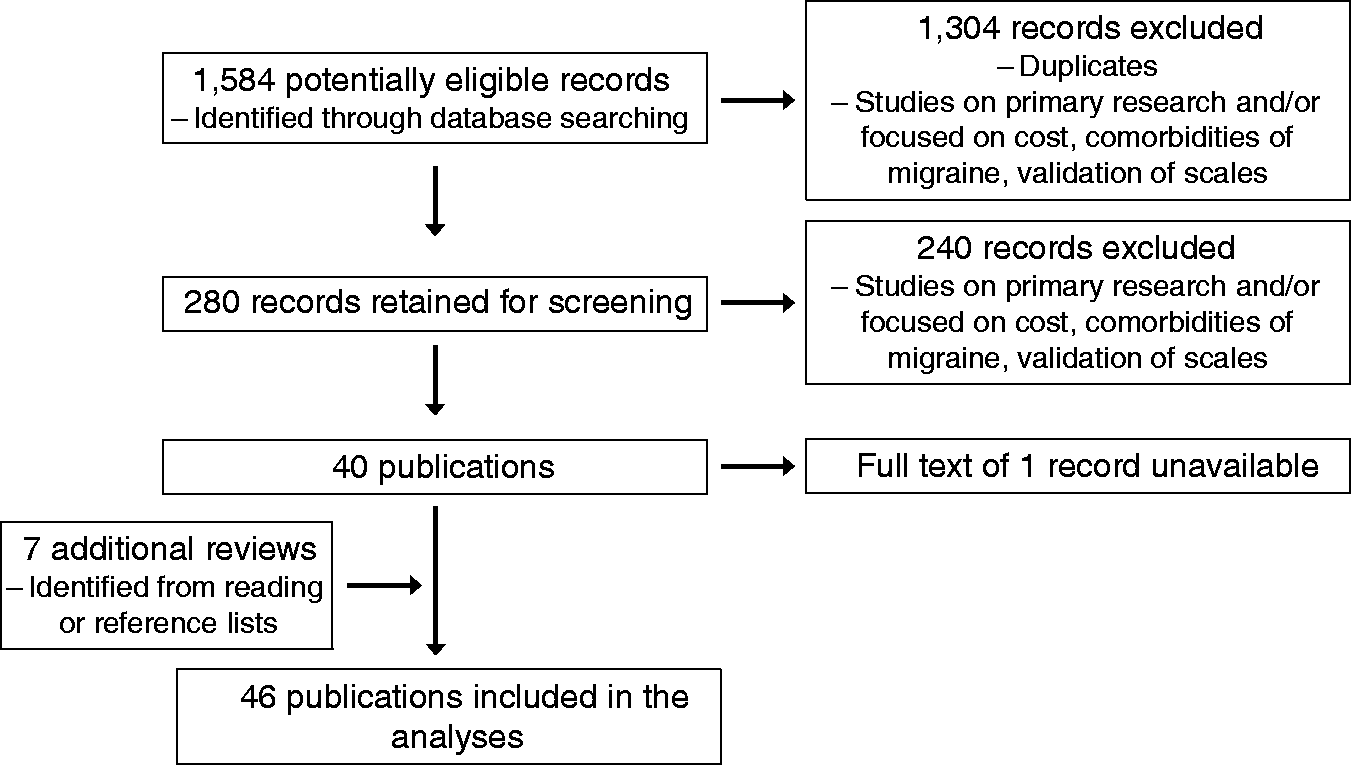
Screening of records from the literature search.
Of these 46, 42 (91%), 36 (78%), 44 (96%) and 28 (61%) respectively offered descriptions of migraine-attributed burden, impact, and disability, and migraine-impacted quality of life. The descriptions were notably characterised by inconsistency and, to some extent, by confusion. Descriptions of migraine-attributed burden included references to impact, disability and quality of life in 45%, 74%, and 38% of cases respectively. This might be expected if burden is considered as an overarching construct, but the descriptions of migraine-attributed impact and disability and of migraine-impacted quality of life commonly included references to each other (Figure 2A), indicating conflation. Ambiguous terminology (for example, GBD’s use of “disability” for lost health, referred to earlier) was a major complicating factor. Overlap between concepts was clearly evident in the specific items ascribed to each concept in the various publications (Figure 2B).
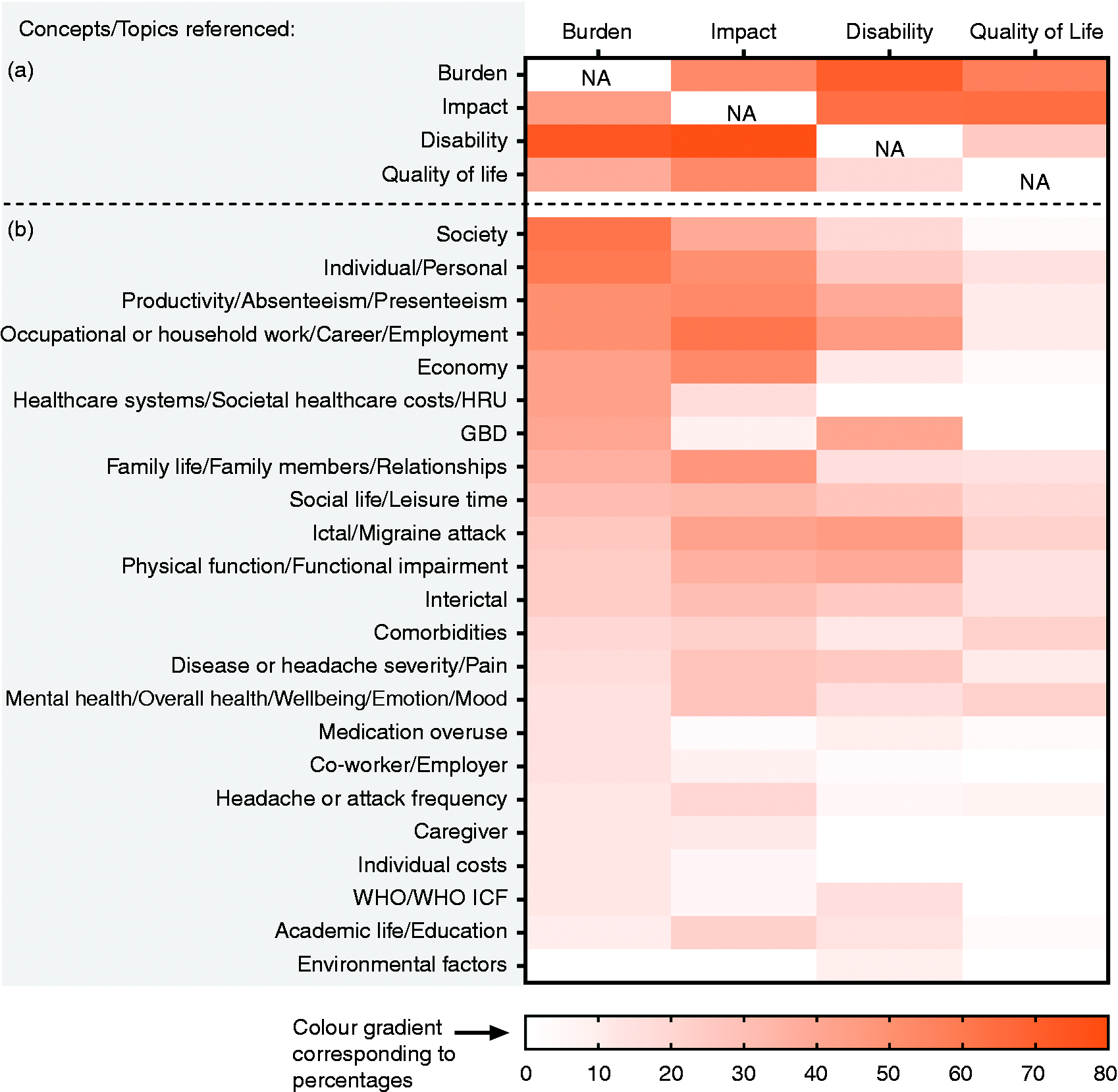
Concepts and topics (and frequencies thereof) referenced in the literature to describe migraine-attributed burden, impact, and disability, and migraine-impacted quality of life. (a) Publications referencing burden, impact, disability and/or quality of life as parts of each other’s descriptions and (b) Publications referencing specific topics in their descriptions of each concept. NA: Not Applicable; GBD: Global Burden of Disease (study); HRU: health resource utilisation; WHO ICF: World Health Organization International Classification of Functioning, Disability and Health.
Aside from conflation and overlap, publications ranged widely in item inclusion. For example, 62% of reviews that provided descriptions of migraine-attributed burden referred to “society”, whereas 24% referred to “interictal” as part of this concept. Among reviews that provided descriptions of migraine-attributed impact, 61% referred to “occupational or household work/career/employment”, whereas 39% referred to “society” as part of this concept. Among reviews that provided descriptions of migraine-attributed disability, 45% referred to “occupational or household work/career/employment”, whereas 9% referred to “environment” as part of this concept. Regarding migraine-impacted quality of life, 21% of reviews that provided descriptions of this concept referred to “ictal/migraine attack”, whereas 7% referred to “headache or attack frequency” as a part of this concept (Figure 2B).
Proposed definitions and descriptions
The second round of the Delphi process achieved >70% agreement (our predetermined target: see Methods) on all definitions (Supplementary Material 2, Table S2). In the third round, which led to 100% consensus on all, we recognised the need for definitions to be not only precise but also memorable, pursuing the purpose of obviating misunderstandings and future inconsistencies (Supplementary Material 2, Table S3). This led to development of concise definitions, each complemented with a detailed explanatory description (Table 1).
Final consensus definitions and detailed descriptions of the four concepts.
Discussion
In this study we used a Delphi process achieving 100% consensus in formulating new definitions, each with complementary descriptions, of migraine-attributed burden, migraine-attributed impact, migraine-attributed disability and migraine-impacted quality of life. What was the need for these, and what purposes might they serve? We began by searching the literature addressing these constructs and concepts, finding it inconsistent and confused. Concepts were often conflated, and terminology used ambiguously or as though synonymous, while being fundamentally important in understanding how migraine affects people and populations (13). They are crucial in managing the disorder, in describing it, and in needs assessment informing healthcare policy and allocation of healthcare resources. Uncertainties in what they mean, and what they embrace, affect all of these adversely, while misinforming the development of treatments, the construction of patient-reported and other outcome measures, and clinical trial design. The benefits of clear and unambiguous definitions should accrue to all of these.
Migraine-attributed burden
We continued to view migraine-attributed burden as an overarching construct, subsuming migraine-attributed impact(s) and disability, and migraine-impacted quality of life. Several features of our definition, and the accompanying description, call for comment. First, there are negative consequences contributing to burden that arise not from the disease itself but from carrying its diagnosis. The latter are due in part to stigma, but there is burden simply in being a patient, in need of healthcare that must be sought (patienthood) (13). Second, migraine-attributed burden arises both ictally and interictally, in the former case, and to some extent the latter, varying between individuals according to frequency, duration and severity of attacks. Third, there are negative consequences of migraine that are cumulative, and which may outlast the currency of the disease: missed opportunities in education, damaged prospects, lack of fulfilment in career or family (13). Fourth, there are negative consequences of the disease borne by others than those who have it, who are in the social environments (family, friends, colleagues, schools, employers) of those who have it (13). Fifth, some aspects of burden fall on society itself: the opportunity costs of resource expenditure on treating the disease, and the societal losses due to workforce diminution and reduced Gross Domestic Product.
While burden as a construct embraces all negative consequences of the disease, and is defined as the summation of these, there are challenges that are likely to remain insuperable in recognising them all, and in measuring many of those that are recognisable. A single metric wholly quantifying burden is not feasible, either at individual or at population level. While GBD makes a valiant effort at quantifying lost health attributable to migraine (which in future iterations may be expressed as healthy life years [HLYs] lost rather than YLDs), its estimates are based on time in symptomatic state: it does not capture interictal burden, cumulative burden or burden falling on others (61).
Migraine-attributed impact
Our definition and description of migraine-attributed impact similarly acknowledge contributions both from the disease itself and from its diagnosis. Crucially, migraine-attributed impact is a singular effect on a singular aspect of life, health or wellbeing, and the term has no meaning unless the latter is specified. Migraine may and often does have multiple effects on many of these aspects, either simultaneously or in temporal sequence, but it is essential to the concept that each of these is a separate impact, distinct from any other (although associations between them are highly likely). Like burden, some impacts are experienced not so much by the person with migraine but by others, through their relationships with and attitudes towards that person. Like burden, some impacts – on education, employment, or family life, for example – are lasting or cumulative, fully expressed only in future outcomes. At the societal level, there are impacts on healthcare demand and supply, and on workforce productivity and economy.
Because impact is a singular effect, it is, potentially, much more readily measurable – in the units that quantify whatever aspect of life, health or wellbeing is impacted (so long as this is itself measurable). Migraine-attributed impact on productivity, for example, can be and often is quantified as lost productive time, but it could also be measured in units of output.
Migraine-attributed disability
Our definition and description of migraine-attributed disability recognise that physical, cognitive and/or mental incapacities are imposed by the disease. Further, our description acknowledges that these incapacities are influenced by the individual’s personal characteristics, and are expressed in the context of that individual’s environment (62). Incapacities may be imposed during the attack, directly by the symptoms of it (pain, visual disturbances and photophobia in particular), or between attacks, for example by interictal anxiety leading to the disability imposed by avoidance behaviour.
Unlike burden and impact, disability is expressed only at individual level. Because of its multifaceted nature and the influences of personal characteristics and environment, migraine-attributed disability is not readily measured and, like burden, cannot be quantified by a single metric. YLDs, as noted earlier, are a measure of lost health rather than disability. The World Health Organization International Classification of Functioning, Disability and Health (WHO ICF) is a system for describing disease-attributed disability taking account of personal characteristics and environment, but requiring complex question sets (62). No such set exists for migraine, although the methodology for creating one has been described (63).
Disability translates into secondary impacts: undone day-to-day activities; missed work or schooling; undischarged household, community or societal responsibilities; abandoned social activities or recreational endeavours; interrupted care for children and family members. All of these become parts of migraine-attributed burden (13), but they are not, themselves, any part of migraine-attributed disability.
Migraine-impacted quality of life
There is a certain tautology about migraine-impacted quality of life, since, as the term implies, it is the consequence of an impact. Conceptually, however, it has unique importance among the many components of migraine-attributed burden, deserving of recognition per se. Our definition and description recognise three distinctions from the concepts of impact and disability. First, it is wholly subjective, and therefore not externally verifiable. Second, it is an evaluation not of the impact itself but of the remnant after it (what is left, not what is taken away). Third, it is an assessment of what is, taking account of the disease as only one among all factors of influence, not of what might be were it not for the disease: at individual level, it makes, or should make, no direct attribution to migraine (no sound basis exists for doing this). For this last reason, it has meaning only in comparison with normative values. It may be summarised across populations, and in large groups the difference between means of normative and migraine-impacted values can be fairly attributed to the disease.
Strengths and limitations
One limitation of this work was the small number of experts contributing to these definitions and descriptions. Another was that people with migraine were not involved or consulted. The major strength is that the definitions and descriptions were formulated to be relevant to care, research and health policy.
Next steps
We recognise that these definitions are a starting point. The next steps require broader input to assess their comprehensibility, acceptability and comprehensiveness. Using different methodologies, these steps must involve experts from other parts of the world – in headache medicine and in public health – and be informed by the views of people who bear the burden of migraine. Alignment across these various constituencies, once achieved, will provide a far better basis than we have now for scrutinising the available instruments, and establishing just how well they measure what they claim to on the one hand and what matters on the other.
Conclusions
The literature in the field of migraine shows inconsistencies, conflation, overlap and confusion in the terminology used to describe migraine-attributed burden and components of it expressed as migraine-attributed impact, migraine-attributed disability and migraine-impacted quality of life. Our definitions and complementary descriptions, arrived at by expert consensus, are a starting point in fostering consistency in the future. Ultimately, the benefits should be expressed in more appropriate use of currently available quantifying instruments and the future development of others, with better care and monitoring of patients, less ambiguity in clinical and epidemiological research, and more reliably informed health policy.
Public health relevance
The literature describing migraine-attributed burden is inconsistent in its use of “burden”, “disability”, “impact” and “quality of life”, often conflating their underlying concepts. These inconsistencies have intruded into quantifying instruments, so that needs assessment, and health policy are unreliably informed. Consensus definitions and detailed descriptions of these terms, formulated through a Delphi process, are offered as a future remedy.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024221110102 - Supplemental material for Migraine-attributed burden, impact and disability, and migraine-impacted quality of life: Expert consensus on definitions from a Delphi process
Supplemental material, sj-pdf-1-cep-10.1177_03331024221110102 for Migraine-attributed burden, impact and disability, and migraine-impacted quality of life: Expert consensus on definitions from a Delphi process by Timothy J Steiner, Gisela M Terwindt, Zaza Katsarava, Patricia Pozo-Rosich, Andreas R Gantenbein, Sarah L Roche, Grazia Dell’Agnello and Cristina Tassorelli in Cephalalgia
Supplemental Material
sj-pdf-2-cep-10.1177_03331024221110102 - Supplemental material for Migraine-attributed burden, impact and disability, and migraine-impacted quality of life: Expert consensus on definitions from a Delphi process
Supplemental material, sj-pdf-2-cep-10.1177_03331024221110102 for Migraine-attributed burden, impact and disability, and migraine-impacted quality of life: Expert consensus on definitions from a Delphi process by Timothy J Steiner, Gisela M Terwindt, Zaza Katsarava, Patricia Pozo-Rosich, Andreas R Gantenbein, Sarah L Roche, Grazia Dell’Agnello and Cristina Tassorelli in Cephalalgia
Footnotes
Acknowledgements
The authors thank Angeles Flores, an employee of Eli Lilly and Company, and Daniela Gödderz, an employee of Executive Insight, for their support with the literature search. We also thank Janet Ford, an employee of Eli Lilly and Company, for support with development of an earlier version of this article and with formulating the input to Delphi Rounds 1 and 2. We are grateful for contributions from David Ayer and Philana Fernandes, employees of Eli Lilly and Company, in, respectively, providing support with formulating the input to Delphi Rounds 1 and 2 and anonymising responses.
Availability of data and materials
Details of the literature search strategies can be found in Supplementary Material 1.
Authors' contributions
All authors contributed to the conception or design of the work. TJS, GMT, PPR, ARG, SLR, GDA and CT contributed to the acquisition, analysis or interpretation of data for the work. All authors contributed to drafting of the work or revising it critically for important intellectual content. All authors approved the final version to be published and agreed to be accountable for all aspects of the work.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TJS reports personal fees from Eli Lilly. GMT reports consultant fees from Amgen, Eli Lilly, Lundbeck, Novartis and Teva, and has received grant support from the Dutch Research Council, Dutch-Brain Foundation, the Dutch Heart Foundation, IRRF, and Dioraphte. ZK has been a speaker and/or consultant, and/or received research support from Allergan, Amgen/Novartis, Eli Lilly, Merck and Teva. PPR has received honoraria as a consultant and speaker for Allergan/AbbVie, Almirall, Biohaven, Chiesi, Eli Lilly, Lundbeck, Medlink, Medscape, Novartis and Teva. Her research group has received research grants from Allergan/AbbVie, AGAUR, la Caixa foundation, EraNET Neuron, FEDER RIS3CAT, Migraine Research Foundation, Instituto Investigación Carlos III, MICINN, Novartis, Teva, and PERIS, and has received funding for clinical trials from Alder, Amgen, Electrocore, Eli Lilly, Lundbeck, Novartis and Teva. She is the founder of ![]() , the Honorary Secretary of the International Headache Society. She is on the editorial board of Revista de Neurologia, an associate editor for Cephalalgia, Headache, Neurologia, Frontiers of Neurology and advisor for The Journal of Headache and Pain. She is also a member of the Clinical Trials Guidelines Committee and Scientific Committee of the International Headache Society and has edited the Guidelines for the Diagnosis and Treatment of Headache of the Spanish Neurological Society. ARG reports financial support for speaking, consultancies, education, research, or travel from Allergan, Almirall, Amgen, Biogen, Biomed, Curatis, Eli Lilly, Grünenthal, Lundbeck, Novartis, Teva Pharma. SLR is a full-time employee of Eli Lilly and Company. GDA is a full-time employee and minor stockholder of Eli Lilly and Company. CT received honoraria for the participation in advisory boards or for lecturing from: Allergan/Abbvie, Eli Lilly, Lundbeck, Novartis, Teva and Medscape. Her Institution has received payments for clinical trials for Allergan/Abbvie, Eli Lilly, Lundbeck, Novartis and Teva. CT has no ownership interest and does not own stocks of any pharmaceutical company. CT is on the editorial board of The Journal of Headache and Pain and Cephalalgia. TJS, GMT, ZK, PPR, ARG and CT did not receive fees from Eli Lilly for the activity related to this manuscript.
, the Honorary Secretary of the International Headache Society. She is on the editorial board of Revista de Neurologia, an associate editor for Cephalalgia, Headache, Neurologia, Frontiers of Neurology and advisor for The Journal of Headache and Pain. She is also a member of the Clinical Trials Guidelines Committee and Scientific Committee of the International Headache Society and has edited the Guidelines for the Diagnosis and Treatment of Headache of the Spanish Neurological Society. ARG reports financial support for speaking, consultancies, education, research, or travel from Allergan, Almirall, Amgen, Biogen, Biomed, Curatis, Eli Lilly, Grünenthal, Lundbeck, Novartis, Teva Pharma. SLR is a full-time employee of Eli Lilly and Company. GDA is a full-time employee and minor stockholder of Eli Lilly and Company. CT received honoraria for the participation in advisory boards or for lecturing from: Allergan/Abbvie, Eli Lilly, Lundbeck, Novartis, Teva and Medscape. Her Institution has received payments for clinical trials for Allergan/Abbvie, Eli Lilly, Lundbeck, Novartis and Teva. CT has no ownership interest and does not own stocks of any pharmaceutical company. CT is on the editorial board of The Journal of Headache and Pain and Cephalalgia. TJS, GMT, ZK, PPR, ARG and CT did not receive fees from Eli Lilly for the activity related to this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Eli Lilly and Company.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.