
Abstract
Introduction
Migraine is a common disorder with a high burden. Adequate treatment results in improvement of quality of life. Migraine patients are mainly treated by general practitioners (GPs), but there is still room for improvement. This study investigated whether primary care nurses could improve the treatment of migraine patients compared to usual care as provided by the GPs.
Participants and methods
We conducted a non-randomized controlled prospective trial in 235 patients diagnosed with migraine with or without aura according to ICHD-II criteria, aged between 18 and 65 years. Patients with migraine treated only by their GP were compared to management by a nurse supervised by a GP.
Results
In the intervention group, fewer migraine patients were referred to a neurologist (p < 0.001). The reduction in monthly migraine days compared to baseline was more apparent in the intervention group at six (p = 0.09) and nine months (p = 0.006). There was no significant change in dichotomized HIT score (p = 0.076). Change in satisfaction of patients did not differ significantly (p = 0.070).
Conclusions
The care administered by a headache nurse in the primary care setting supervised by a GP resulted in fewer referrals to the neurologist and more migraine-free days per month, but no change in HIT score. There was no difference in satisfaction scores between both groups.
Introduction
Migraine is a common disorder characterized by debilitating headache attacks, affecting approximately 12% of the population in the Western world (1). The burden of migraine is high, resulting in a loss of quality of life, inability to go to school or work, and a great impact on family and social life (2). Adequate treatment of migraine results in an improvement of quality of life (3). Migraine patients are mainly treated in primary care by the general practitioner (GP). However, migraine consultations are time consuming, which is a problem for GPs with limited time available. Consequently, in the treatment of migraine by the GP there is room for improvement (4).
For other medical conditions, primary health care nurses have already been successfully deployed, e.g. in the treatment of urinary incontinence and diabetes (5,6). Primary health care nurses may also improve the management of migraine patients (7). The role of the nurse in migraine management may include providing patients with information on medication, trigger identification and avoidance, and lifestyle changes. Although many reviews and editorials have been written about a possible positive role of nurses in the treatment of migraine, only two inconclusive pilot studies have been performed (8,9).
This study was conducted to investigate whether the introduction of primary care nurses, who had been trained in aiding in managing migraine under supervision of a GP, compared to usual care as provided by the GP can improve treatment of migraine patients, resulting in fewer migraine-related hospital referrals, a larger reduction in headache days per month, and improvement of patient satisfaction with treatment.
Participants and methods
Design
This study was a non-randomized, controlled prospective trial that was conducted following general medical practices in the eastern part of The Netherlands. In three practices nurses, supervised by the GP, were deployed to provide care to migraine patients. This constituted the intervention group. Migraine patients in eight other practices, who were subjected to usual care as provided by the GP, served as the control group.
The primary outcome constituted the migraine-related GP’s referral rate to the hospital. Referral rate to the neurologist for migraine was chosen as the primary endpoint in order to study primary care-related treatment options to improve the management of this type of patient population. Secondary outcomes in patients were changes in Headache Impact Test (HIT) scores dichotomized at 50 points, changes in mean monthly headache days after three, six and nine months, and differences in patients’ satisfaction with treatment between the control and intervention groups.
The GPs were selected based on their geographical proximity to the Isala Clinic in Zwolle. Every GP who was contacted was willing to participate in this study. The practices in the intervention group were chosen randomly because they already employed primary care nurses for other diseases.
The GPs and nurses in both groups were unaware of the endpoints of the study. The GPs in the control group were not aware that the treatment of the migraine patients was being investigated.
The study inclusion started March 2011, and ended September 2011. A follow-up of nine months was performed by a research nurse until July 2012.
This study was approved by the local medical ethics review board (number 11.0211).
Participants
In the intervention group, patients who consulted the GP for headaches, and who were diagnosed with migraine, were referred to the primary care nurse for management and follow-up. In the control group, the migraine patient was treated only by the GP. In the intervention group the primary care nurse checked whether the patient had a (probable) migraine diagnosis in accordance with the International Classification of Headache Disorders, second edition (ICHD-II) criteria, and in the control group this was performed by the research nurse. Patients with migraine were included if they met the following inclusion criteria: aged between 18 and 65 years, a diagnosis of migraine according the ICHD-II, and provided written informed consent.
Intervention
The migraine patients in the intervention group were managed by a nurse who was supervised by the GP. The nurses followed a four-day course on migraine in which they were trained in diagnosing migraine, according to the ICHD-II criteria, the prescription options of acute and prophylactic migraine medication, and non-pharmacological treatment aimed at identifying and avoiding migraine triggers, and lifestyle changes. During this four-day course the migraine nurse obtained clinical experience regarding diagnosing and treating migraine patients under the supervision of a neurologist at a headache outpatient department.
The responsibilities of the nurse were to administer non-pharmacological treatment, provide information about medication for acute or prophylactic treatment, and initiate GP-prescribed pharmacological treatment when necessary. Non-pharmacological management involved providing education about migraine and helping patients to identify situations that could reduce migraine attacks. Regularly the nurse reported back to the GP the results of the treatment. If necessary the nurses suggested to the GP adjustments of medication.
During a baseline period of four weeks, the patients completed a headache questionnaire that included questions about headache characteristics and demographic characteristics. They also kept a diary in which they recorded the presence, duration in hours, and severity of the headache using the visual analog scale (VAS) score, the use of acute and prophylactic medication and number of headache days per month (10). At baseline, three, six and nine months, patients completed the HIT (11). Satisfaction of patients with the total treatment was assessed using a five-point scale, with 1 being totally satisfied and 5 totally unsatisfied.
Data collection
The data of the patients in the intervention and control groups were collected by research nurses who were unaware of the endpoints.
Data were collected after three, six and nine months by a research nurse. In the control group, the research nurse was instructed to avoid interference with the migraine treatment of the patient initiated by the GP.
Statistical analysis
The characteristics of patients within a given general practice typically tend to be more alike than those of patients across different practices. Ignoring this clustering of information usually results in an underestimation of the magnitude of the standard error, and hence affecting the probability to reach significance. The analysis of such data requires a multilevel approach that accounts for this practice dependent clustering of information.
Because in this study patients were nested within GP practices, we conducted a multi-level analysis using MLwiN 2.25. Multilevel models are hierarchical systems that estimate regression coefficients and their variance components while at the same time correct for the dependency of information. The first level was defined as patient, the second level as GP’s practice. A correction for confounding was applied in the event the regression coefficient of the group variable was subject to ≥10% change as a result of fitting the model with a confounder (12). Duration of migraine attacks and menstruation-induced migraine attacks were considered potential confounders in the relationship between the proportion of referred patients and intervention group allocation in this study.
For the secondary outcomes of patient satisfaction and number of monthly headache days, linear multilevel regression models were developed The assumptions of normality and homogeneity of the variance were assessed by inspecting normal probability plots and plots of standardized residual vs. predicted values. Because the original as well as log-transformed HIT score variable did not comply with the assumptions, this variable was dichotomized (cut-off at 50 points).
To address the primary outcome, all available patients were included in the analysis. The analyses of the secondary outcomes were conducted on two populations: 1) non-referred patients and 2) referred and non-referred patients. Once patients were referred to the neurologist they were excluded from the analyses of the secondary endpoints. This may have generated a less severe and not fully representative migraine population of non-referred GP patients. Therefore, we conducted an additional analysis to determine whether this patient selection may have affected the secondary outcomes. This latter analysis was performed on the referred and non-referred patient population. For all tests, a two-tailed significance level of p < 0.05 was used.
Results
Baseline characteristics
After the baseline period, three patients in the control group and four patients in the intervention group were excluded because they were diagnosed with medication-overuse headache.
A total of 235 patients diagnosed with migraine were enrolled in this study between March 2011 and September 2011: 94 patients in the control group and 141 in the intervention group.
Baseline characteristics.

According to visual analog scale (VAS) score (0–10). bSome patients had migraine of multiple duration. HIT: Headache Impact Test.
Follow-up
Outcome measurements.
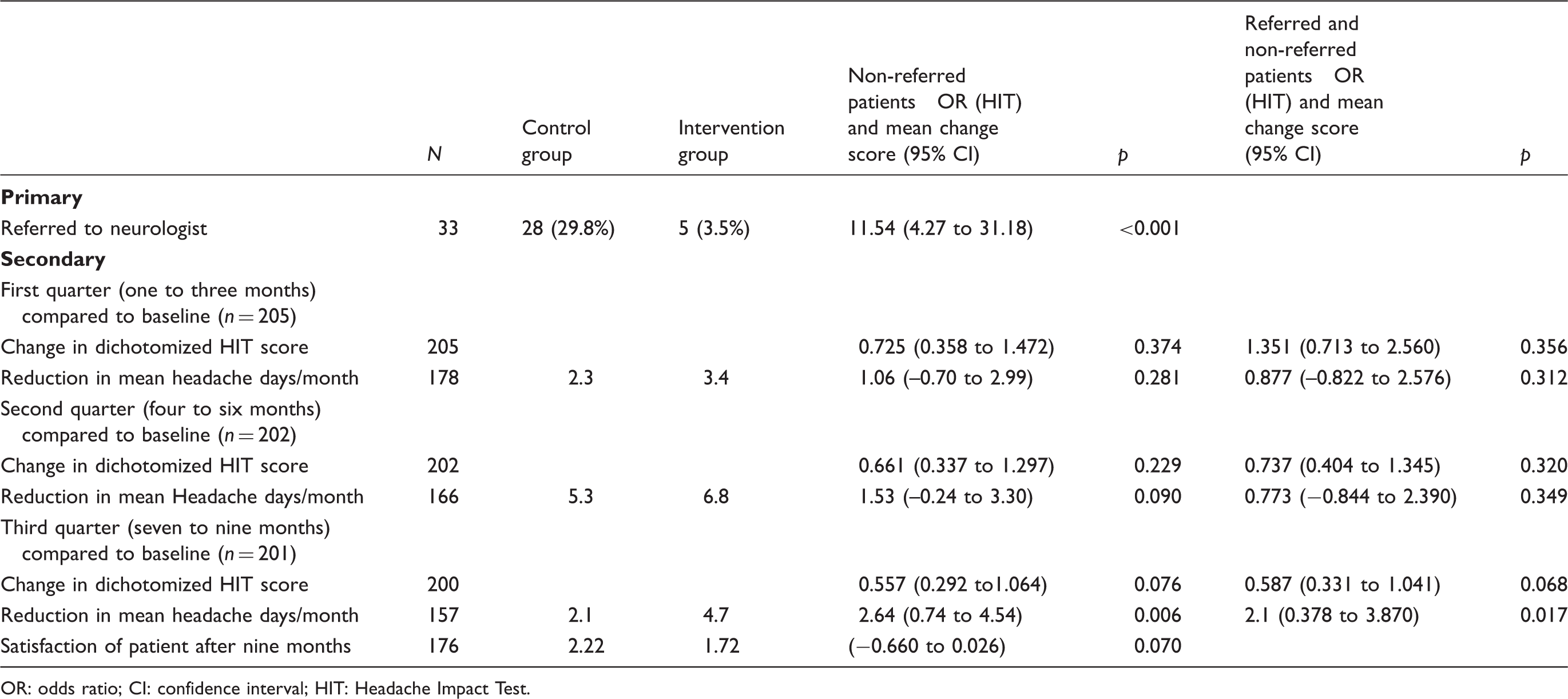
OR: odds ratio; CI: confidence interval; HIT: Headache Impact Test.
There was no statistical significant difference in using prophylactic medication between the intervention and control group after nine months (18% in the control group vs. 29.4% in the intervention group p = 0.172).
In the intervention group 110 patients visited the migraine nurse four times according to the study schedule, resulting in a total of 440 visits. The group of 31 patients who did not complete the entire follow-up had a total of 54 visits with the migraine nurse. In the intervention group during follow-up there were 26 visits to the GP; with the 120 visits at inclusion this came to a total of 146 visits to the GP. In the control group during follow-up, there were 80 visits to the GP, with the 94 visits at inclusion this came to a total of 174 visits to the GP. There were no phone contacts.
Main outcome measurements
In total 27 women and six men were referred to the neurologist for their migraine, with a mean age of 38 years. At baseline the patients, who were referred to a neurologist, experienced a mean HIT score of 62.76 (compared to 62.18 in the non-referred group), and at baseline a mean of 8.8 headache days per month (compared to 6.74 in the non-referred group).
Table 2 shows the data of the endpoints in comparison to baseline. There were no missing values on the variables used for the analysis on the primary endpoints. In the intervention group, fewer patients were referred to the neurologist. The reduction in mean headache days each month compared to baseline was larger in the intervention group at six months and nine months. The dichotomized HIT after three, six and nine months did not differ significantly in both groups. Satisfaction of patients with treatment compared to baseline after nine months did not differ significantly between the control group and intervention groups.
The significance of outcomes of the secondary endpoints in the non-referred population was consistent with those of the non-referred and referred patient population.
Discussion
Principal findings
To the best of our knowledge, this is the first study that investigated whether primary care nurses supervised by GPs could improve the treatment success of migraine in primary care patients. Patients with migraine treated by a nurse were less often referred to a neurologist because of their migraine, and experienced a larger reduction in headache days per month from baseline to nine months of follow-up.
However, the HIT score didn’t significantly decrease in the intervention group in comparison to the control group. This might be explained by the HIT score being a measuring tool for the qualitative aspects of migraine and does not directly measure the quantitative aspects of migraine. Therefore, the HIT score cannot explain the difference in referral rate to the neurologist between groups. This might be due to other factors, such as consultation frequency, patient anxiety and concern about their headache symptoms (13). The nurses are probably responsible for the lower referral rates because they are spending more time with the patients, reassuring them, and giving information and education about migraine.
The decrease from baseline in headache days per month in the intervention group is probably explained by the non-pharmacological management administered by the nurses, as there was no significant increase in consumption of prophylactic medication in the intervention group. Educating patients with migraine may help them to identify situations that could trigger migraine attacks, and improve lifestyle changes. Education of migraine patients improves the quality of life in these patients (14).
In time, the number of headache days decreased both in the control and the intervention groups. The reason for the decrease in the control group might be related to the natural course of migraine and regression to the mean (15).
We chose “referral of a migraine patient to the neurologist” as the primary endpoint of our study because we believe that this is a valid indication that the treatment of the migraine patient in primary care is not adequate. There are several reasons for a referral to specialist care, all of which are related to inadequate treatment, often resulting in a patient being dissatisfied, including an inability to reassure a patient or a GP who feels unable to manage a patient’s care without the input of a specialist. A referral is often not just a simple process but a highly complex interaction that involves multiple stakeholders and is influenced by a wide range of factors (16).
Comparison with other studies
As noted in the introduction, two studies suggested a beneficial role of nurses in the treatment of headache (8,9). The two pilot studies have investigated whether health education delivered by a nurse in primary care could improve migraine outcome. One study involved an experimental group (n = 19) and a control group (n = 25). After six months, the authors did not find a statistically significant reduction in frequency (p = 0.664), and duration (p = 0.235) of headaches, and in the Migraine Disability Assessment (MIDAS) score (p = 0.535) in the intervention group (8). The intervention and the control group consisted of patients with a variety in migraine severity, and patients with other primary headaches diagnoses. Another pilot study of 195 patients concluded that advice on headache management given by a nurse can lead to significantly improved patient outcome (total MIDAS score, headache frequency, headache severity and physician consultations for headache). However, not every patient received the same treatment, as only the patients with severe migraine were subsequently offered an appointment with a headache specialist physician for diagnosis and interventions. A shortcoming mentioned by the authors is the sample sizes got smaller as the visits proceeded, but no numbers were named in the article (17). Furthermore, there was no control group in this study. The authors of these studies suggest that education of patients by a primary care nurse may decrease the perception of the disability in migraine patients. In addition to non-pharmacological treatment, the nurses in our study evaluated the pharmacological treatment and if needed this was changed after consultation with the GP.
Studies investigating the contribution of primary care nurses in other illnesses showed that patients preferred nurse practitioners over only GPs for their treatment (18,19). In these studies, patients who consulted nurse practitioners received longer consultations, were given more information and were generally more satisfied. We found no significant difference between the control group and the intervention group in change in patient satisfaction scores, although a trend was observed toward more satisfaction in the intervention group.
Strengths and limitations
The strengths of this study are the multiple assessments across the follow-up period, which allowed us to examine changes in migraine at several times during the study period.
A limitation of this study is that the GP practices were not randomized. The practices in the intervention group were chosen because they already employed primary care nurses for other diseases. Because of budgetary constraints, we were not able to hire our own nurses and randomly assign them to primary care practices. However, in the control group six of the eight practices were also working with specialized primary care nurses for other diseases. Furthermore, the GP practices in the intervention and the control groups were of comparable size. The average number of GPs working in the intervention group was 4.5 and 3.5 in the control group. The GPs and nurses were blinded to the outcomes.
The GPs in both groups may not have included migraine patients in the study consecutively at an equal pace. However, the main characteristics, mean headache days per month and HIT score of patients in the control and intervention groups were comparable at baseline.
Clinical implications
In a non-randomized, controlled prospective trial a specialized nurse in primary care, supervised by a general practitioner, managing patients with migraine reduces the migraine-related referral rate to the hospital, and results in a larger reduction in headache days per month. The question remains whether the care provided by a nurse performing migraine management in primary care is cost effective. This did not affect the change in Headache Impact Test (HIT) scores between the groups.
Footnotes
Acknowledgements
General practitioners: MAG Broeren, H Dijk, C Hartman, H Post, MC Wennemers, DH Zwanenburg, K Hofstee, CR Meeder, Chr Meyer, HJW Pruijs, JCF Lokin-Kleeman, RM Oosterhout, MC de Vries, A de Lange, A Meutstege, TJ Jansen, JMHP Lemmens, WCG Seegers, SO Driessen, S Zwart, R vdHoef, R Bruintjes, L Bruintjes-Kolleman, J Posthouwer, R Sanaan, AJM Groot, O Schwantje, R Sikkema, J Meijer, J Schmitz, H Speijers, FGW Cleveringa, GK Beintema, DHM van Grieken, FS Oldenhof, FN Ridderbos, EJ van Apeldoorn, JE Brouwer, MF Luiting, PM Roseboom and AJFA de Ruiter.
Migraine nurses: AD Riphagen, H de Lange and R Ebbink.
Research nurses: G van Vemde and M Hulsmann.
Funding
This work was partially supported by a grant from Achmea Health Insurance.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.