
Abstract
Background
The preset study aimed to explore whether work schedules and sleep disorders predict the onset of headache.
Methods
A longitudinal study was conducted with questionnaire data from 2014 (baseline) and 2017 (follow-up) on work schedule, number of night shifts, number of quick returns, insomnia, shift work disorder (SWD), restless legs syndrome (RLS) and validated headache diagnoses among 1560 Norwegian nurses. Associations were explored by multivariate regression analyses.
Results
Work related factors at baseline did not predict onset of headache three years later. In the adjusted logistic regressions, insomnia at baseline predicted increased risk of new onset of migraine (odds ratio (OR) = 1.58; 95% confidence interval (CI) = 1.08–2.33), chronic headache (OR = 2.02; 95% CI = 1.04–4.66) and medication-overuse headache (OR = 3.79; 95% CI = 1.26–11.42) at follow-up. SWD at baseline predicted new onset of migraine (OR = 1.64; 95% CI = 1.07–2.50) and RLS at baseline predicted new onset of headache ≥1 day per month (OR = 1.55; 95% CI = 1.01–2.36) and migraine (OR = 1.55; 95% CI = 1.03–2.32) at follow-up. No factors predicted tension-type headache.
Conclusions
Overall, work related factors did not predict the onset of headache three years later, whereas insomnia, SWD and RLS at baseline all increased the risk of future headaches.
Introduction
Studies show that shift work increases the risk of sleep disturbances, such as insomnia and shift work disorder (SWD), cardiovascular disease, metabolic disorders, and certain cancers (1). Night workers are on duty during their biological resting phase and are as such enforced to schedule sleep to their biological active phase. This has been proposed as a one causative factor for health problems (1). Also, night work and other shift work schedules, such as quick returns (QRs), defined as less than 11 hours of free time between two shifts, typically curtail sleep; hence, sleep deprivation is another mechanism by which shift work may impair health.
In line with the above, studies suggest that the number of night shifts per year and the number of QRs per year are associated with increased risk of health complaints and sick leave (2–4).
It is well-established that lack of sleep can trigger headache, and that sleep may also alleviate headache (5–7). Disturbed sleep as a result of shift work or insomnia are therefore likely to increase the risk of headache. Previous studies have found associations between sleep disorders such as insomnia, obstructive sleep apnea syndrome and restless legs syndrome (RLS) and headache disorders, although not consistently (8–12).
Still, very few studies have investigated the relationship between work related factors and headache. We have previously shown that nurses with SWD report higher prevalence of headache, but we did not find any associations between specific work schedules and headache (13). A Danish study found an association between headache and shift work, one study from China reported that number of night shifts was positively associated with prevalence of headache and another study from Taiwan suggested that shift work increases the risk of migraine (14–16).
However, almost all studies in this field suffer from methodological limitations, such as cross-sectional designs, highly selected populations, low number of participants and not using validated headache or sleep questions adhering to the criteria of the International Classification of Headache Disorders-3 (ICHD-3) or the International Classification of Sleep Disorders (13–20).
Based on the knowledge that headache and sleep problems often co-occur and the hypothesis that work schedule may trigger headache, we aimed to investigate whether work schedule, number of night shifts, number of QRs, sleep duration, insomnia, SWD and RLS predict the onset of any new headache or a primary headache disorder in a large sample of nurses followed over a period of three years.
Methods
Sample
The data stemmed from the ongoing longitudinal cohort study “SUrvey of Shift work, Sleep and Health (SUSSH)” among Norwegian nurses (Figure 1). The first data collection was conducted during 2008/2009 (wave 1) when a sample of 5400 nurses was randomly selected from the Norwegian Nurses Organisation’s membership roll and invited to participate. The sample was based on random sampling within stratas divided by time elapsed since graduation (less than 12 months, 1–3 years, >3–6 years, >6–9 years and >9–12 years). This sampling method was chosen to obtain sufficient variation in length of work experience among the nurses in the study sample. A total of 2059 (response rate = 38.1%) nurses completed the questionnaire at the first wave. To increase the size of the study population, an additional sample of 905 newly educated nurses (response rate =33.0%) was recruited to wave 1 in 2009. The total sample in wave 1 therefore included 2964 nurses (21). The nurses who responded to the first wave have been invited to participate in annual follow-ups by receiving questionnaires sent by postal mail with pre-paid envelopes for returning the completed forms. Up to two reminders in each wave were sent to nurses who did not respond. The nurses who returned the questionnaire took part in a lottery, in which 25 individuals won a gift card with a value of 500 NOK (approximately US$60). The present study reports findings based on data from the sixth (2014, here defined as baseline) and ninth (2017, defined as follow-up) wave, in which validated headache questions were included. In total, 2005 out of 2869 eligible nurses completed the questionnaire at wave 6, yielding a response rate of 69.4%. Only nurses who also completed the ninth wave were included in the present study (n = 1560).
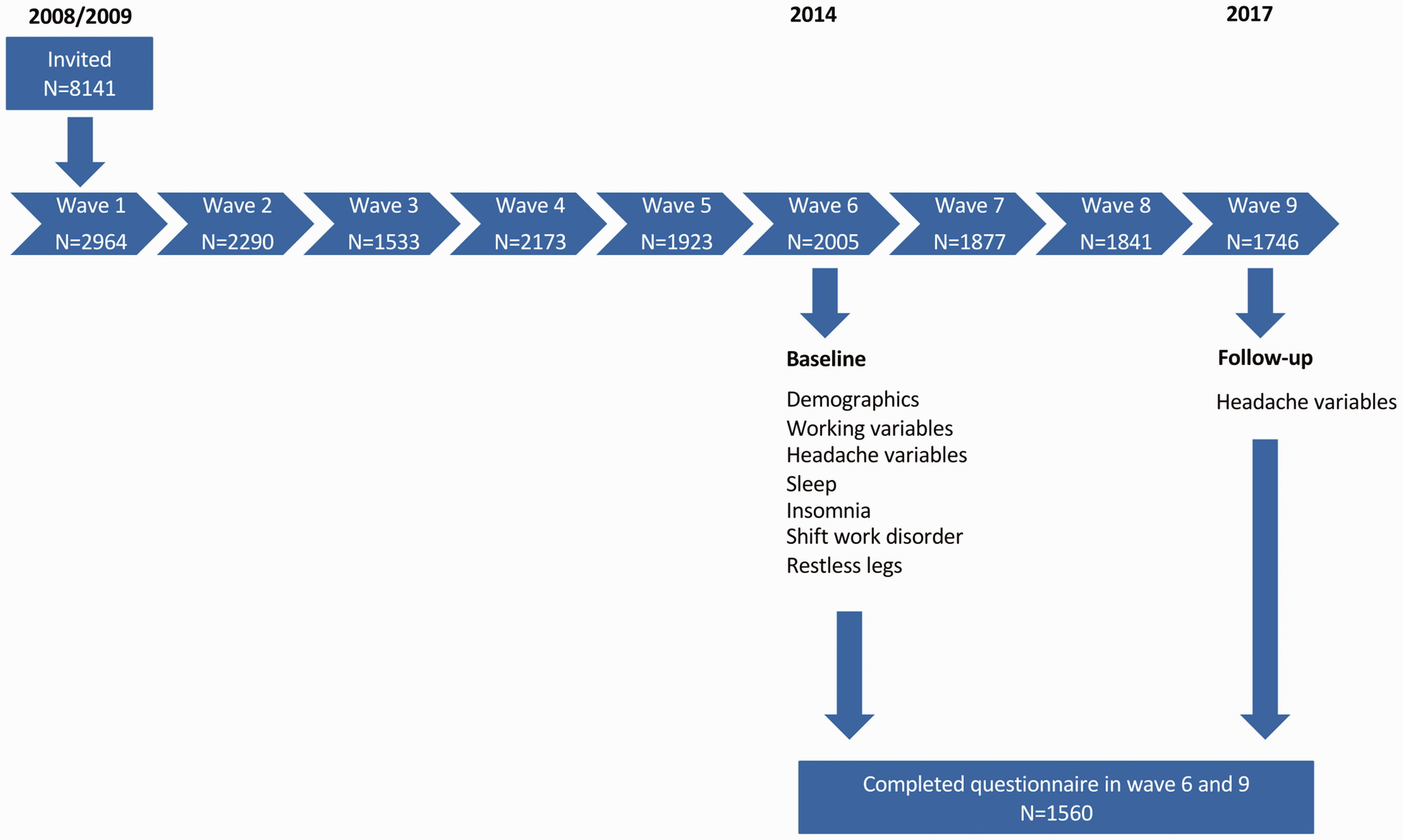
Flowchart of the SUrvey of Shift work, Sleep and Health (SUSSH).
Demographics and working variables
The demographic variables were assessed in wave 6 (Figure 1). The nurses responded to questions about marital status (married/cohabiting; yes/no), children living at home (yes/no), percentage of full-time equivalent (<50%, 50–75%, 76–90%, >90% position), average working hours per week (≤20.0, 20.1–39.9, ≥40 hours), work schedule (day only, evening only, two-shift rotation (day and evening), night only, three-shift rotation (day, evening and night) and other schedules including night work), number of night shifts worked last year, number of quick returns (defined as less than 11 hours between consecutive work shifts) worked last year. Few nurses worked “evening only” (n = 4) and “other schedules including night work” (n = 50) and data from respondents working these shifts were therefore excluded from the analysis of the association between work schedule and headache. Some participants (n = 6) reported having >150 QR during the last year. These figures were deemed erroneous and replaced by 150 because we considered this the maximum realistic number of QR one person can possibly have in one year. Three participants reported >200 night shifts during the last year. These figures were replaced with 200 for the same reason as above.
Headache classification
The comprehensive headache questionnaire used at baseline and follow-up was designed to determine whether the nurses suffered from headache, and complied with the International Classification of Headache Disorders (ICHD) 3 criteria for migraine, tension-type headache (TTH) and medication-overuse headache (MOH) (22). The nurses were first screened: “Have you suffered from headache during the last year?” and only nurses who answered “yes” were asked to respond to the subsequent headache items. Those screening positive for headache were asked to report frequency, attack duration, intensity and accompanying headache symptoms to classify migraine and TTH, accordingly. The diagnoses of migraine and TTH were mutually exclusive. Chronic headache was defined as headache >14 days per month, independently of underlying subtype. MOH was defined as chronic headache and intake of acute headache medication ≥10 days last month. The questionnaire-based headache diagnoses used here have previously been validated in a large unselected general population sample (23). For the questionnaire-based status of having headache, a sensitivity of 88%, a specificity of 86% and a kappa statistic of 0.70 were found. Chronic headache and MOH were diagnosed with a specificity of >99%, a sensitivity of 69 and 75%, and a kappa statistic of 0.75. Lower figures were found for the diagnoses of migraine and TTH. For individuals with headache >1 day per month, a sensitivity of 58% (migraine) and 96% (TTH), a specificity of 91 and 69%, and a kappa statistic of 0.54 and 0.44, were found, respectively (23).
Sleep classification
SWD was measured with three previous used questions based on the minimal criteria listed in the International Classification of Sleep Disorders (ICSD-2) (24). The questions were: (i) Do you experience either difficulties sleeping or experience excessive sleepiness? (yes/no); (ii) Is the sleep or sleepiness problem related to a work schedule that makes you work when you normally would sleep? (yes/no); and (iii) Have you had this sleep or sleepiness problem related to the work schedule for at least one month? (yes/no). Participants were classified as having SWD if they endorsed all three questions (25).
Insomnia symptoms were evaluated with Bergen Insomnia Scale (BIS) (26). The BIS consists of six items, and was developed based on the diagnostic criteria for insomnia according to 4th version of the Diagnostic and Statistical Manual for Mental Disorders (DSM-IV) (27). The items are scored along an eight-point scale indicating the number of days per week for which a specific insomnia symptom is experienced (0–7 days). The items refer to sleep onset (sleep latency exceeding 30 minutes), wake after sleep onset (more than 30 minutes), early morning awakening (more than 30 minutes), non-restorative sleep, daytime impairment and dissatisfaction with sleep. The time frame is insomnia symptoms experienced during the past month. According to DSM-IV-TR criteria (27), insomnia disorder is defined as scoring three days per week or more on at least one of the first three items as well as three days per week or more on at least one of the latter two items. Missing responses to any of the insomnia questions were treated as not reporting that specific insomnia symptom. The scale has acceptable test–retest reliability, and good convergent and discriminative validity in relation to other self-report measures as well as to polysomnographic data (26). Cronbach’s alpha for the BIS was 0.79 in the present sample.
RLS was diagnosed with four questions based on the ICSD-2 (24): (i) during the past three months, have you had an urge to move the legs or arms, usually accompanied with discomfort or unpleasant sensations in the legs or arms? (ii) If yes, does this urge start or increase when you are resting, such as when lying or sitting? (iii) Is the urge to move or the unpleasant sensation partially or completely relieved when you are moving, such as when walking or stretching? (iv) Is the urge to move or unpleasant sensation worse late in the day or at night compared with the rest of the day? All four questions were rated “yes” or “no.” Only those nurses who answered endorsed all four diagnostic criteria were defined as having RLS (28).
Ethics
The study was approved by the Regional Committee for Medical and Health Research Ethics of Western Norway (REK-West, no 088.08). Written informed consent was obtained from all participants.
Statistical analysis
Descriptive data are presented as proportions, medians, and interquartile ranges (IQR) for categorical variables and in terms of the mean ± SD for continuous variables. Groups were compared using the t-test/Wilcoxon signed-rank test (continuous data) or the chi-squared test (categorical data).
Separate crude and adjusted (with age, sex, marital status, children living at home and as covariates) logistic regression analyses were performed to assess new onset of headache, headache ≥1 day per month, chronic headache, migraine, TTH and MOH at follow-up as dependent variables with average working hours per week (20.1–39.9 as reference compared to ≤20.0 and ≥40 hours), work schedule (day only as a reference, compared to two-shift rotation, night only and three-shift rotation), number of night shifts last year (0 as reference compared to 1–20 and >20 night shifts), number of QRs last year (0 as reference compared to 1–20 and >20 QRs), sleep duration (6–8 hours as reference as compared to <6 hours and >8 hours), chronic insomnia (no insomnia as reference), SWD (no SWD as reference) and RLS (no RLS as reference) as predictors (all collected at baseline). New onset was defined as not having headache at baseline, but at follow-up.
p < 0.05 (two-tailed) was considered statistically significant. Statistical analyses were performed using SPSS, version 29.00 (IBM Corp., Armonk, NY, USA).
Results
The baseline data of the nurses are presented in Table 1.
Baseline characteristics of the Norwegian nurses in the study (n = 1560).

IQR, interquartile range. n, number of nurses.
The median age at baseline was 36 (IQR = 31–42, range 27–69) and 91.4% (n = 1418) were female.
Headache data from baseline and follow-up are presented in Table 2. More participants reported headache last year at follow-up compared to baseline (60.5 vs. 55.9%, p < 0.001).
Headache data from baseline (n = 1554) and follow-up (n = 1551).
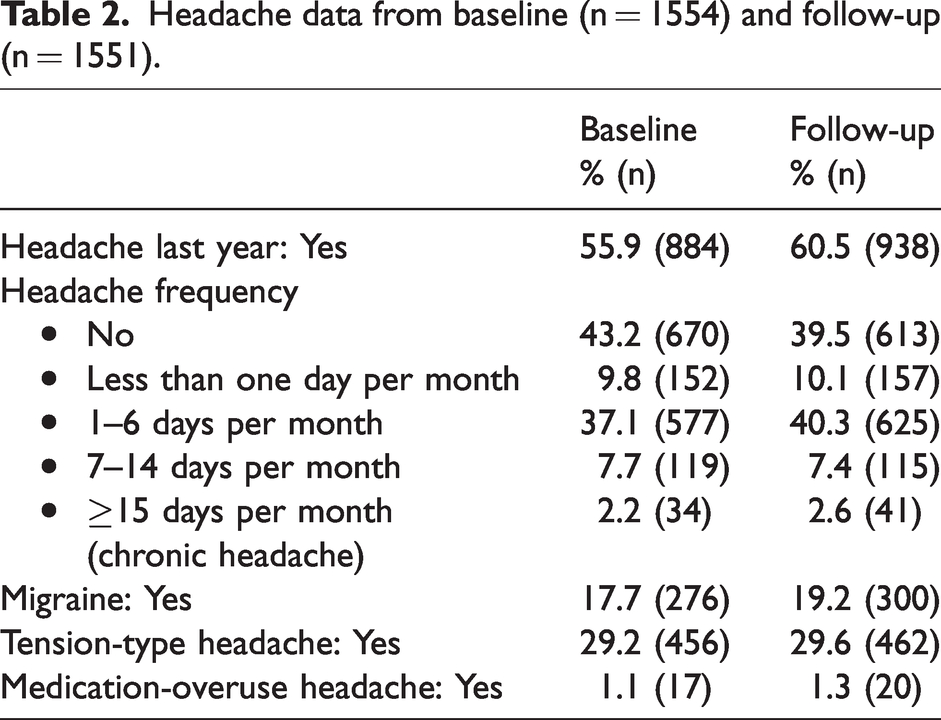
The proportions having no headache at all or headache less than one day per month were 53.0% (n = 822) at baseline and 49.6% (n = 770) at follow-up. The prevalence of migraine increased from 17.7% to 19.2% (p < 0.001).
Among those without any type of headache at all at baseline (n = 667), 223 reported headache at follow-up, 149 reported headache ≥1 day per month, 30 reported migraine, 142 reported TTH, zero reported MOH and six reported chronic headache at follow-up.
Overall (n = 1551) 127 nurses reported no migraine at baseline (they could have reported other headache at baseline), but migraine at follow-up. The corresponding figures for TTH, MOH and chronic headache were 221, 14 and 29 nurses, respectively.
In the crude analyses age, female sex and children living at home all predicted increased risk of reporting new onset of headache at follow-up, whereas working three-shift schedule predicted reduced the risk of new onset of headache (Table 3). Working three-shift schedule remained a significant predictor with a decreased (odds ratio (OR) = 0.55; 95% confidence interval (CI) = 0.34–0.91) probability of new onset of headache at follow-up in the adjusted regression analyses (Table 3).
Logistic regression analyses predicting new onset of headache (n = 223) at follow-up among those with no headache at baseline (n = 667)

Significant findings are shown in bold.
Female sex and children living at home predicted increased risk of reporting new onset of headache ≥1 day per month at follow-up in the crude analyses (Table 4). The adjusting factors married/cohabiting and children living at home were significantly predicting a decreased and increased risk of new onset of headache ≥1 day per month, respectively (Table 4). RLS was the only significant predictor for new onset of headache ≥1 day per month at follow-up in the adjusted analyses (Table 4).
Logistic regression analyses predicting new onset of headache ≥1 day per month (n = 149) at follow-up among those with no headache at baseline (n = 667)

Significant findings are shown in bold.
Insomnia (OR = 2.02; 95% CI = 1.04–4.66) was the only significant predictor of new onset of chronic headache at follow-up (n = 29) among those without chronic headache at baseline (n = 1519) in separate adjusted logistic regression analyses (complete data not shown).
Female sex, children living at home, sleep duration <6 hours and insomnia all predicted new onset of migraine from baseline to follow-up in the crude analyses (Table 5). Female sex and children living at home still significantly predicted increased risk of developing migraine in all the adjusted models. In the adjusted regression analyses sleep duration <6 hours (OR = 2.75; 95% CI = 1.51–4.99), insomnia (OR =1.58; 95% CI = 1.08–2.33), SWD (OR = 1.64; 95% CI = 1.07–2.50) and RLS (OR = 1.55; 95% CI = 1.03–2.32) predicted increased risk of developing migraine from baseline to follow-up (Table 5).
Logistic regression analyses predicting new onset of migraine at follow-up (n = 127) among those without migraine at baseline (n = 1283)

Significant findings are shown in bold.
No factors predicted new onset of TTH from baseline to follow-up (Table 6). Insomnia and sleep duration <6 hours at baseline were the only two predictors of new onset of MOH at follow-up with an OR 3.79 (95% CI = 1.26–11.42) and OR 4.20 (95% CI = 1.14–15.45), respectively (data not shown).
Logistic regression analyses predicting new onset of tension-type headache at follow-up (n = 221) among those without tension-type headache at baseline (n = 1104)
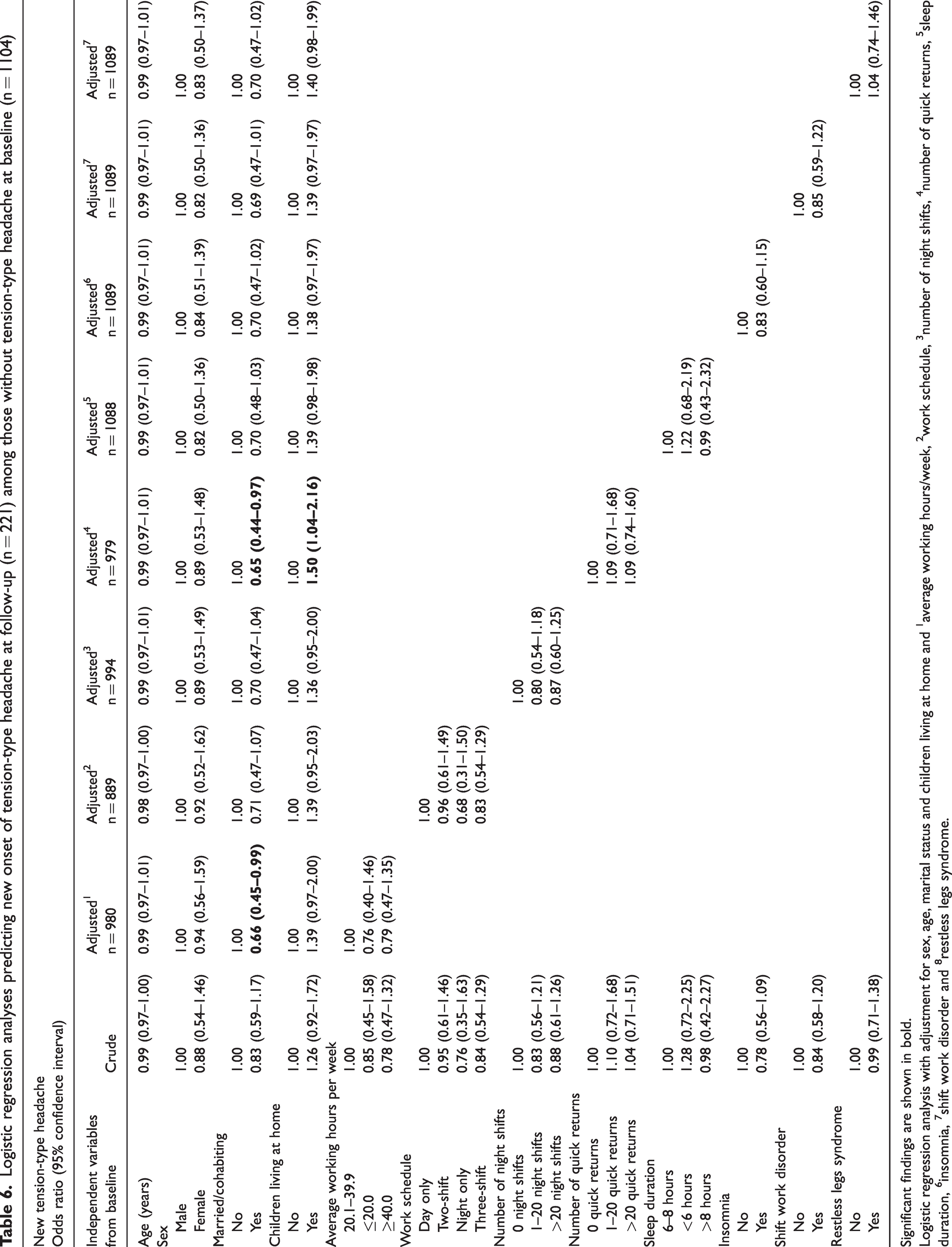
Significant findings are shown in bold.
Among those with 1–6 headache days per month at baseline the following factors predicted increased headache frequency (≥7 headache days per month) at follow-up compared to still having headache 1–6 days at follow-up in the adjusted logistic regression analyses: insomnia (OR = 2.39; 95% CI = 1.47–3.88) and SWD (OR = 1.79; 95% CI = 1.09–2.94) (data not shown).
Sensitivity analysis which only included nurses aged <35 years at baseline showed no significant differences or shift in results compared to the main analysis (data not shown).
Discussion
In this large follow-up study of nurses using validated questionnaires for sleep and headache classifications, insomnia, SWD and RLS at baseline were found to be significant predictors of new onset of headache and/or migraine at follow-up.
We hypothesized that night work, number of night shifts and quick returns would predict new onset of headache at follow-up. This was based on the association between short sleep duration and headache, and the fact that both rotating shift work schedules and night work normally will cause circadian rhythm misalignment as well as sleep deprivation. As expected, sleep duration <6 hours at baseline predicted an increased risk of new onset of migraine and MOH at follow-up confirming previous studies (29). However, surprisingly, the present study showed that work related factors did not predict new onset of headache three years later. Indeed, three-shift schedule actually predicted reduced risk of new onset of headache. This may be a spurious finding because there is no clear biological rationale. One interpretation may be that nurses working on a three-shift schedule are nurses who tolerate such working conditions, in line with the notion of the healthy worker effect (30). Another explanation is that work factors may influence headache but through sleep problems such as insomnia and SWD, which were related to several types of headache. The findings from other studies on work schedule and headache are conflicting (8,13–16,19,20). Almost all of them are cross-sectional, using different criteria for headache disorders and sleep disorders, and the various work schedules included, together with various confounding factors, do not allow extrapolation of conclusions on the work schedule and headache relationship. One Danish longitudinal study found higher odds of unspecific headache (OR = 1.25) and migraine (OR = 1.72) among shift workers compared with day workers (14). However, that study did not use the headache classification for migraine, the definition of shift work was very broad, the authors did not have the opportunity to include number of night shifts or quick returns in the analyses, and sleep problems were defined based on different parts of sleep questionnaires.
Even though shift work and quick returns did not increase the risk of new onset of headache by themselves, there is a subgroup of people who do not cope well with shift work and may develop SWD. SWD and its relationship to headache disorders has never been investigated in prospective studies before. Nurses with SWD at baseline had increased odds of new onset of migraine. Among those with 1–6 headache days at baseline, SWD also predicted increased odds for having ≥7 headache days per month compared to 1–6 headache days per month at follow-up.
These novel findings suggest that nurses with SWD are at increased risk of developing more frequent headache and migraine later in life. This is important and adds to the emerging evidence that SWD leads to future risks of developing other health complaints.
Previous cross-sectional population based studies have supported an association between insomnia, RLS and headache disorders (11,31–33). One of very few prospective studies of the general population that used the same headache questions as the present study found that insomnia at baseline significantly increased the relative risk for new onset of migraine, TTH and MOH 11 years later (18). The study also found a significant association between insomnia at baseline and headache frequency at follow-up. A limitation of that study was the lack of a validated insomnia questionnaire. Our prospective study of nurses lend support to the notion that insomnia at baseline increases the odds of developing migraine, MOH and chronic headache three years later also when using validated sleep and headache instruments. The pathological mechanism underlying the association between migraine, headache chronification and insomnia is not yet fully understood and even a bidirectional relationship has been suggested (6,10).
RLS and migraine have been extensively investigated in cross-sectional studies with a prevalence of RLS in migraine patients varying from 14% to 25% (11,12). Studies have shown a bidirectional association and a potential dose-response in the relationship, meaning that frequent RLS is associated with headache frequency and vice versa. To our knowledge, the present prospective study is the first to show that RLS at baseline increases the odds for new onset of headache and/or migraine later. The association between RLS and migraine has been suggested to be the result of a shared dopaminergic dysfunction in the hypothalamus (10,12).
Age and female sex both predicted increased risk of new onset of headache at follow-up. These findings are in line with previous findings and are thus not unexpected. Females are known to have a higher prevalence of headache and migraine and the prevalence increases with age until a peak is reached during the fourth decade (34). Having children living at home predicted increased risk of reporting new onset of headache and migraine in both the crude and adjusted analysis. This risk was increased independently of the other adjusting factors. To our knowledge, this is a novel finding not previously described. Future studies should investigate whether it is pregnancy and the subsequent child birth itself, having the responsibility for a child living at home or other factors that increase the risk for developing new headache.
The present study was based on a large and homogeneous sample of nurses that limits the influence from possible confounding variables. Other strengths were the prospective design, the use of validated headache diagnoses and validated insomnia and RLS scales as well as criteria-based SWD diagnostics (18,25,26,28). Furthermore, the study did not have a primary focus on headache because it was one of many health outcomes. Thus, a possible selection bias related to headache was consequently considered unlikely. In terms of limitations, it should be noted that the response rate in the first wave was low, which may make the interpretation of the data and conclusions less generalizable. Still, the response rates in waves 6 and 9, in which the headache questions were included, were high. As a result of the high number of participants in our survey, it was not feasible to apply the gold standard (i.e. a clinical interview by a physician experienced in headache and sleep diagnostics). For the same reason, prospective headache and sleep diaries were not feasible to administer.
Including nurses older than 40 years (up to 69 years) may be a limitation because the bell-shaped curve of migraine prevalence decreases from the age of 40 years (34) However, most nurses were younger than 40 years at baseline. We also performed sensitivity analysis including only nurses <35 years with no significant differences compared to the total sample.
The questionnaire-based headache diagnostic procedures have been validated and included in several previous large population-based studies (23). A limitation is that migraine and TTH are mutually exclusive, meaning that the questionnaire only allows the same participant to be diagnosed with the most bothersome headache subtype even though some might suffer from both migraine and TTH. Because migraine is hierarchically more important in the headache classification than TTH, it is likely that there is an underestimation of TTH in the sample. and the findings of TTH should therefore be interpreted with caution. The headache questionnaire asked about bothersome headache, implying that some nurses with very mild and few headaches may have been excluded from the headache group. Additionally, headache is usually regarded as a symptom, while migraine, TTH and MOH are categorized as headache disorders. Another limitation with the questionnaire used in the present study is that it does not report life-time prevalence of migraine, only headache during the last year. It will therefore not capture those with migraine having less than one headache day per year. This makes detecting new onset of migraine a challenge from a methodological perspective. Furthermore, the true prevalence of those with less than one migraine day per year is disputed, but probably higher in those >60 years (35,36).
As for other studies using self-reported data, we cannot rule out that there are people having migraine without being aware of it. However, in the present study, categorizing migraine was based on respondents reporting different sets of symptoms and not a self-reported migraine diagnosis.
The number of participants with changed headache frequency between baseline and follow-up was low, limiting the statistical power for analyses related to change.
Furthermore, it should be acknowledged that BIS may not accurately differentiate between insomnia and other sleep disorders. For example, participants with obstructive sleep apnea and circadian rhythm sleep–wake disorders may also fulfill the criteria for insomnia based on BIS. 37 However, this limitation may pertain to all insomnia scales. Another limitation is that our study is based on nurses and the findings may therefore not be generalizable to the general population. Still, the findings may be of relevance and importance to the public health and occupational medicine field because many workers are part of a rotating shift schedule.
Conclusions
Sleep disorders reported at baseline, such as insomnia, SWD and restless legs syndrome, were found to be significant predictors of new onset of headache and migraine at three years follow-up. Overall, work related factors did not predict onset of headache disorders.
Clinical implications
There is a lack of prospective studies investigating the role of work factors and sleep problems on the risk of headache disorders In this prospective three-year follow-up study using validated headache and sleep questionnaires, insomnia, shift work disorder and restless legs syndrome at baseline all predicted increased risk of new onset of headache The association of restless legs syndrome and migraine has previously been proposed, but never shown in a prospective study before The present study is the first to show that shift work disorder increases the risk of migraine and headache frequency Nurses, employers and clinicians should pay attention to the possible risk of headache related to sleep disorders
Footnotes
Acknowledgments
We are grateful to all nurses participating in the study and to the Norwegian Nurses Organisation for funding and help with recruitment.
Data availability
Declaration of conflicting interests
The authors declare that there are no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
SUSSH was partly funded from the Norwegian Nurses Organisation and Nordforsk, Nordic Programme on Health and Welfare (74809).