
Abstract
We tested the usefulness and applicability of a simplified headache diary in the diagnosis of migraine (M), tension-type headache (TTH) and medication overuse headache (MOH). The diary was given to headache patients before their first consultation at the headache centre. Seventy-six naive headache patients completed the study. Their understanding of the diary proved highly satisfactory. The patients' level of compliance was also good, with 71± returning the diary completely filled in. The data entered in the diary were deemed complete for the diagnostic purpose in 93± of cases. The level of agreement between headache information gathered through clinical interview and the headache diary was satisfactory. When comparing the diary with the clinical interview, sensitivity was 92± for M, 75± for TTH and MOH. Specificity was 58± for M and TTH, 87± for MOH. Combined use of a diagnostic diary and clinical interview is recommended from the first consultation for headache.
Keywords
Introduction
The original International Headache Society (IHS) classification of headache disorders (1), now nearly two decades old, represented a pivotal advance in headache clinical practice and research, offering diagnostic criteria for the different primary and secondary forms. A revised version of these criteria, now universally adopted in headache centres, was recently published [International Classification of Headache Disorders, II Edition (ICHD-II), 2004] (2). In the case of primary headaches, the diagnosis rests almost entirely on the presence of specific clinical characteristics and is reached mainly through a detailed patient history, the finding of a negative physical examination, and the exclusion of local or systemic disease(s) that can cause secondary or symptomatic headache.
In clinical practice, it is known that patients may not easily identify and recall certain features of their headaches, such as the presence and type of aura symptoms, specific associated symptoms, and the coexistence of several types of headache.
Therefore, the use of monitoring instruments becomes crucial in the diagnosis of these disorders: in headache diaries and calendars, the characteristics of every attack can be recorded prospectively, increasing the accuracy of the description and making it possible to distinguish between coexisting headache types; moreover, headache diaries provide the physician with information concerning other important features, such as the frequency and temporal pattern of attacks, drug intake, and the presence of trigger factors. A recent review (3) has looked at the various applications and usefulness of headache diaries and calendars, and the authors showed that, in previous studies (4–8), some diagnostic diaries have been found to constitute a valid means of diagnosing migraine compared with interviews.
Diaries are usually given to patients at their first appointment. Integrated with the data collected during the clinical interview, the data collected through the diary can subsequently be used to define the frequency of attacks or to monitor the response to treatments. The aim of the present study was to test the applicability and potential usefulness of a simplified diagnostic diary intended to be used in the period prior to the patient's first evaluation. Our main concerns were to assess (i) the patients’ understanding of the instrument, (ii) their compliance and reliable entering of data, and (iii) the potential usefulness of the diary as a supporting diagnostic tool.
Methods
A basic diagnostic headache diary was devised based on previously tested formats (4, 8) and on the clinical expertise of the investigators, who met on several occasions to generate the final version that was adopted in the study. The diary is based on the ICHD-II diagnostic criteria for migraine (M), tension-type headache (TTH) and medication overuse headache (MOH) (Fig. 1). The diary comes with a set of simple, but detailed instructions (Fig. 2).

The basic headache diary.

Instructions attached to the basic headache diary.
The basic headache diary and the instructions were devised by the authors in English and subsequently translated into Danish and Italian. The diary, together with the instructions, were mailed to a random sample of 84 new headache patients awaiting a consultation at the headache centres of Pavia or Copenhagen, at least 4 weeks prior to their scheduled appointment.
In the instructions, patients were asked to start filling in the diary on a daily basis and to bring it with them on the day of their appointment.
The criteria for chronic TTH and for MOH were modified on account of the short recording period (8). The general requirement for diagnosing chronic TTH is headache on at least 15 days a month during at least 3 months. In this study, the criterion applied for diagnosing chronic TTH was the presence of TTH on at least a half or on more than half of the days in the recording period. Likewise, for MOH, the IHS criteria demand use of symptomatic drugs on a specific number of days/month for a period of 3 months and development/worsening of headache during medication overuse (9). Since these two criteria cannot be evaluated from a diary kept for 4 weeks, in our study MOH was diagnosed when the headache was present on at least 15 days per month and the relevant symptomatic overused drug criterion was met. During the initial evaluation, before seeing the diaries, a senior physician (examiner 1) with a pluridecennial experience in the field of headache (G.S. and R.J.) collected headache history, performed the physical examination and made the diagnoses. This diagnostic procedure was assumed to be the gold standard. The diagnostic headache diaries filled in by the patients were then evaluated and discussed with them to ascertain their understanding of it, compliance with it and the completeness, for diagnostic purposes, of the information collected. Two additional senior physicians (examiners 2 and 3), who were blind both to the patients’ history and to the diagnoses made by the first physician, were asked to formulate diagnoses exclusively on the basis of the information contained in the diaries.
Data analysis and statistics
As mentioned above, the following variables relating to the diaries were evaluated:
The headache diagnoses were recorded in the order by examiner 1. All data were analysed using the
Results
Of the 84 patients on the waiting list contacted by mail, 78 arrived at the centre with their diary filled in for at least 4 weeks and were therefore enrolled in the study; six patients did not show up on the day of the scheduled appointment for unknown reasons. Forty-five subjects were evaluated at the headache centre in Copenhagen, Denmark, and 33 at the headache centre in Pavia, Italy. At the interview, two patients proved to be suffering from cluster headache and were therefore excluded from the analysis. The final group of patients evaluated (
As regards the patients’ understanding of the diary (Fig. 3A), 93% reported no difficulty whatsoever in understanding and providing the required information; just 4% reported some problems, mainly concerning the exact duration and intensity of the headache, and the lack of space on the page for recording the medications used. Three percent of the patients failed to provide information regarding their understanding of the diary.
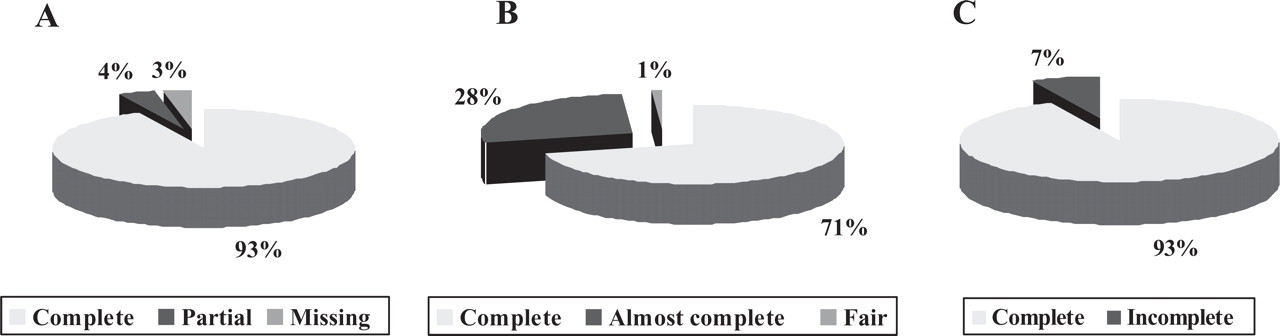
Patients’ understanding (A), patients’ compliance (B), and completeness, for diagnostic purposes, of the data entered (C).
Assessment of patients’ compliance showed that it was complete in 71% of cases, almost complete in 28% and fair in just 1% (Fig. 3B). The item most frequently missing was the time of headache onset or disappearance. In fewer cases, patients omitted to tick the ‘NO’ option in the diary items regarding associated symptoms, even though such symptoms were, in fact, absent.
The data entered in the diary were complete, thus allowing the reaching of a definite diagnosis, in 93% of patients, whereas in the other 7% the missing data precluded a definite diagnosis (Fig. 3C), while allowing, in all cases, a diagnosis of probability.
When the diagnoses obtained with the gold standard procedure were compared with those based only on the diary information (Table 1), the first remarkable finding was the higher number of diagnoses yielded by the diary analyses: 115 diagnoses were made on the basis of the clinical interviews (1.5 per patient), whereas evaluation of the diaries resulted in 141 diagnoses (1.8 per patient in the case of examiner 2).
Types and distributions of headache diagnoses made using the gold standard method (examiner 1) or the diary alone (examiners 2 and 3)

MoA, migraine without aura; MA, migraine with aura; M?, probable migraine; ETTH, episodic tension-type headache; CTTH, chronic tension-type headache; TTH?, probable tension-type headache; MOH, medication overuse headache.
Another important finding to emerge from comparison of the diary-based with the gold standard approach was the higher number of migraine with aura cases in the diary-based diagnoses: 15 for examiner 2, even more (
A high rate of agreement as regards the distribution of diagnoses was instead observed for both migraine without aura and episodic TTH, with only minor differences in the total number of diagnoses emerging between the gold standard and examiners 2 and 3. As regards MOH, this form was diagnosed in 16 subjects through interview and in 18 subjects through the use of the diary (both examiners).
The level of agreement between the diagnoses reached by examiners 2 and 3 was fairly good for all types of headaches, with a κ value of 0.50, 0.47 and 0.49, for M, TTH and MOH, respectively. It is noteworthy that when the level of agreement between examiners 2 and 3 was calculated, irrespective of the order of their diagnoses, but simply considering the presence of the first diagnosis made by the gold standard procedure, the κ value rose to 0.63, to suggest a quite high level of agreement.
When analysing diagnoses based on clinical interview with those based on the diary, sensitivity and specificity levels were 92 and 58%, respectively, for M, 75 and 58%, respectively, for TTH and 75 and 87%, respectively, for MOH (see Table 2).
Comparison of diagnoses of migraine (A), tension-type headache (B) and medication overuse headache (C) based on clinical interview (examiner 1) and based on the diary (examiner 2)
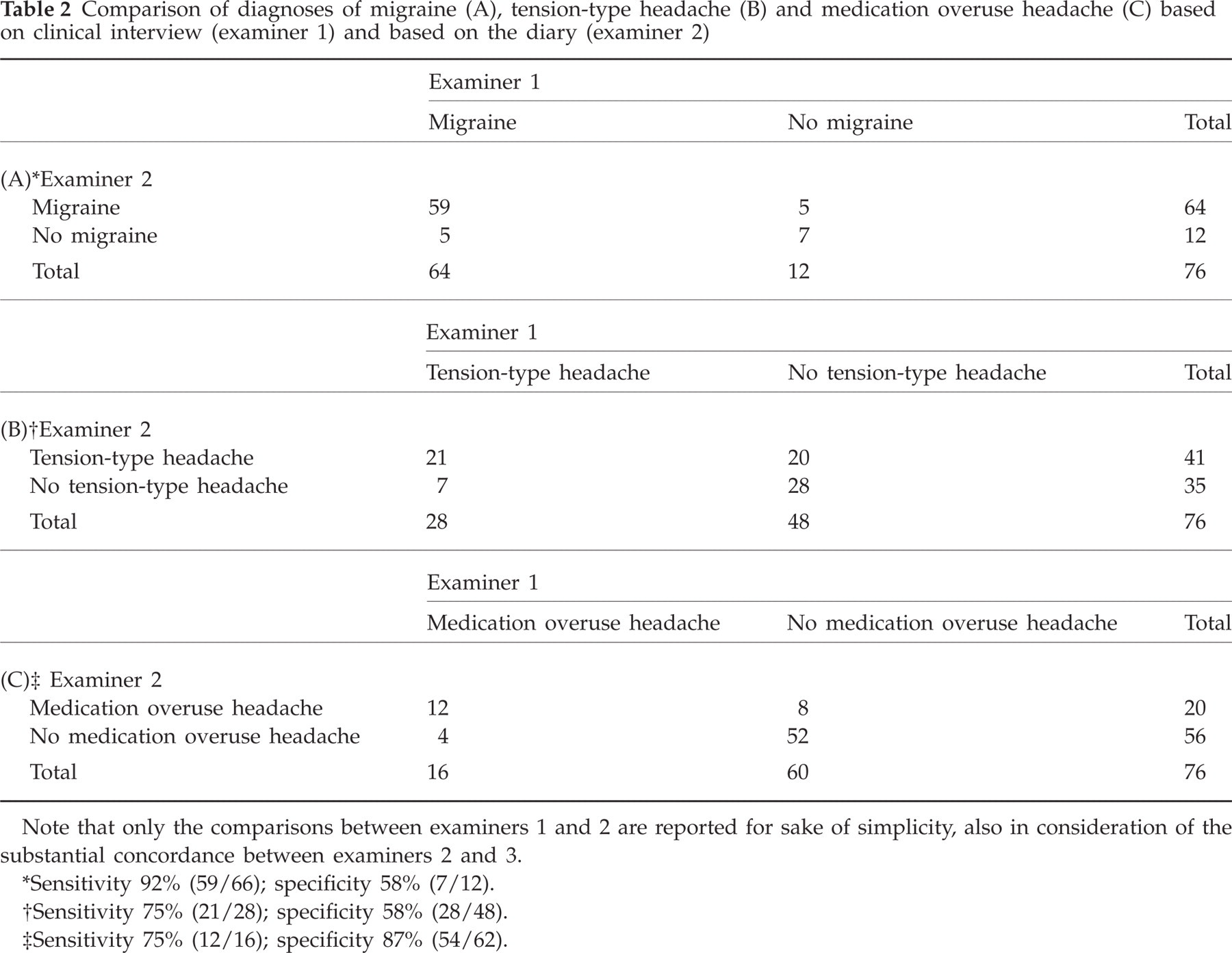
Note that only the comparisons between examiners 1 and 2 are reported for sake of simplicity, also in consideration of the substantial concordance between examiners 2 and 3.
Sensitivity 92% (59/66); specificity 58% (7/12).
Sensitivity 75% (21/28); specificity 58% (28/48).
Sensitivity 75% (12/16); specificity 87% (54/62).
Discussion
The present study was conducted on a small population of headache patients and was planned as a pilot study. The sample size was chosen on a clinical basis and experience from two tertiary headache clinics, not a result of a proper power calculation. The number of patients included was considered sufficient to test properly the applicability of the diary in a short period of time. In this phase we were mainly focused on evaluating the patients’ acceptance, comprehensibility and compliance. The variation in the general impact among patients from different clinical settings, the actual performance of the diary as a diagnostic tool as well as the detailed characterization of responders and non-responders represent important issues that will be thoroughly analysed in the subsequent, large multicentre study. Our simple diary was based on the ICHD-II classification criteria for M, TTH and MOH (2), and was used in a totally innovative way, being compiled by naive patients waiting to be seen in our headache centres. The only instructions obtained by the patients were those received by mail along with the diary. Patients’ understanding of the instrument was highly satisfactory (complete in 93% of cases), but the most interesting observation was the high compliance shown by patients in filling in the diary, which determined a high rate of completeness for diagnosis. Previous studies have reported unsatisfactory levels of compliance (10, 11), and this discrepancy may be related either to increased motivation on the part of our patients, who were eager to use every resource available to ensure the best possible management of their disorder from their first appointment or, alternatively, to the provision of simple but detailed instructions on how to fill in each single item of the diary.
In agreement with previous reports (4), our data suggest that the use of diaries allows the detection of an increased number of diagnoses per patient. In most cases, this seems to be due to the increased number of diagnoses of probability (e.g. probable M or probable TTH). This phenomenon has a likely explanation in the possibility to detect and record attacks that are not full-blown—e.g. when they are aborted precociously by symptomatic drugs—and therefore do not satisfy all the diagnostic requirements. In the interview, patients are more likely to report their most severe, full-blown attacks, forgetting to describe incomplete ones. In a minority of cases, thanks to the analytical prospective record of drug intake, the diaries led to the diagnosis of additional cases of MOH.
The higher number of diagnoses of migraine with aura obtained through the diary approach is the result of some patients’ misunderstanding of the question on aura, which they confused with photophobia or premonitory symptoms. This was ascertained by means of a cross re-evaluation of the diaries and interviews.
The analysis of specificity and sensitivity was limited to the first diagnostic level due to the small number of patients and to the pilot nature of the study. Specificity was higher than sensitivity in M and TTH, probably as a direct result of the higher number of diary-based diagnoses, i.e. the diaries allowed the identification not only of the true positive subjects, also identified by the interview, but also of an extra group of sufferers who were detected only from the diaries. In the case of MOH, both sensitivity and specificity were more than satisfactory, probably as a result of the small difference between the number of MOH cases diagnosed through interview and the number diagnosed from the diaries. Pursuit of this line of reasoning leads us to question the very concept of interview + physical examination as the gold standard, and to ask ourselves whether it should not be replaced by the combination interview + physical examination + diary.
Minor adjustments (e.g. the question regarding the aura) and further testing of this basic headache diary in a large-scale, ad hoc study are needed to evaluate extensively its usefulness in supporting the diagnosis of M, TTH and MOH.
This pilot study has confirmed the acceptability of the diary to patients and their high compliance with its requirements. In this phase we performed a very limited analysis of how filling in the diary might improve the process of diagnosing primary headaches. It is likely, however, that its real usefulness may lie in its capacity to furnish data on the frequency of different headache types, to disclose trigger and precipitating factors, and to allow real assessments of the medications taken by patients in situations of suspected drug overuse.
As with other tested diaries, some limitations are intrinsic to the use of this diary. For example, our diary cannot replace the clinical interview in the diagnosis of other forms of primary headache, particularly cluster headache and other primary short-lasting headaches, and even more so in the diagnosis of secondary headaches. In addition, our diary does not go beyond the first or second diagnostic level. It is therefore both necessary and desirable to develop new diaries for specific types of primary headache (e.g. migraine with aura, menstrual migraine, trigeminal autonomic cephalalgias) or for particular populations (e.g. children). Another delicate issue to be defined is for how long the patients should fill in the diary before their first appointment. In this study, we required the diary to be filled in for only 4 weeks, which prompted the adaptation of ICHD-II criteria. However, this was a deliberate choice from the investigators and represents a compromise between practical use and the ideal world. The period may be too short for the infrequent forms of headache, most often seen in primary or secondary care. In tertiary care the vast majority of patients suffer from chronic or very frequent headaches, and it was the authors’ opinion that 3 months’ systematic recordings only very rarely change their initial diagnosis based on 4 weeks’ recordings. Likewise, selection bias of those patients that complete diaries for 3 months may also impair the usefulness of such a diagnostic instrument. Future studies will need to address these issues.
The satisfactory findings regarding comprehension, compliance and completeness, for diagnostic purposes, of the data entered in the diaries underline the usefulness, whenever possible, of adopting the diary before patient's first consultation, as this may provide additional information that can be integrated with the data collected through the interview and may ultimately shorten the time to definite diagnosis and allow a more complete diagnosis (especially in the event of coexisting forms of headache).
A multicentre study involving several European countries is currently underway to evaluate an improved version of the basic headache diary presented here. The improvements made are based on decisions taken at a consensus meeting attended by a large panel of experts. The availability of a valid and validated common instrument that can be used to support the diagnosis of the most frequent and disabling forms of primary headache will be a major step towards achieving a homogeneous approach to the process of diagnosing headache in different countries and settings.
Acknowledgements
The study was supported by the Eurohead project (LSHM-CT-2004-504837). The authors gratefully thank Dr A. Citterio and Professor C. Montomoli for their support in the statistical analysis of the data, and Dr P. Torelli for her valuable suggestions during the preparation of the diary.