
Abstract
Aims: We tested the usability and usefulness of the basic diagnostic headache diary (BDHD) for the diagnosis of migraine, tension-type headache and medication-overuse headache in European and Latin American countries.
Methods: Patients were subdivided into two groups according to a 1:1 randomization list. Those in group 1 were sent the BDHD before their first visit to the headache centre and asked to complete it for at least 1 month. Those in group 2 made their first visit to the headache centre without receiving the BDHD.
Results: A total of 626 patients from nine countries and 16 centres completed the study. The BDHD entries were complete in 97.5% of cases. BDHD information and clinical interview were, when taken together, considered complete for diagnosis in 97.7% of cases in group 1 whereas the information obtained by clinical interview alone in group 2 was considered complete in only 86.8% of cases (p < 0.001). The median number of diagnoses per patient in group 1 was significantly higher than in group 2 (p = 0.04). The BDHD was very well accepted by both patients and doctors.
Conclusions: It is concluded that the BDHD is a useful tool in the diagnostic assessment of the most frequent and disabling forms of primary headache and in headache management.
Introduction
In the absence of biological markers, headache diagnosis depends mainly on a detailed history and a normal physical examination. Precise diagnostic criteria for migraine and tension-type headache (TTH) – the two most common types of primary headache – have been available since the first International Classification of Headache Disorders (ICHD) in 1988 (1). In the 2004 2nd revised edition of the ICHD (ICHD-II), changes were limited to chronic forms of primary headache and some secondary headaches, including medication-overuse headache (MOH) (2). The correct application of the ICHD-II criteria for each type and subtype of headache should allow the precise diagnosis of these headache disorders consistently across neurologists and across countries. In clinical practice, however, patients often have difficulty recalling their headache characteristics, especially if they suffer from several types of headache, or their precise intake of symptomatic drugs, especially if they overuse them. Therefore, monitoring charts to detect and diagnose headache types becomes a necessary aid in the management of headache disorders.
Headache diaries and calendars provide the physician with important information by prospectively recording the characteristics of every attack and the frequency and temporal pattern of attacks over months, thereby minimizing recall bias and increasing adequacy in the description of headache features (3–5). In previous studies, some diagnostic diaries have proven to be valid for diagnosing migraine when compared to interviews (6–12). A basic diagnostic headache diary (BDHD) for migraine, TTH and MOH, based on the criteria of the ICHD-II, was tested in a pilot study in the specialized headache centres of the cities of Copenhagen (Denmark) and Pavia (Italy) (13). This simple diary was given to headache patients before their first consultations. The results of this pilot study suggested that the diary was easy for patients to complete and that its use yielded a very satisfactory rate of completion for the purpose of establishing the diagnoses of migraine, TTH and MOH. Comparison of diagnoses made by simply reviewing the diaries with those arrived at by the ‘gold standard’ procedure of direct interview of the patient by the physician showed a very satisfactory rate of concordance.
From this initial basic headache diary, and after these encouraging results, a modified and improved version of the BDHD was developed, and a multicentre study involving several European and Latin American countries was undertaken to assess its usability and usefulness in the diagnosis of migraine, TTH and MOH. The study tested the following hypotheses:
The diary is helpful for diagnostic assessment; The diary is well accepted and easy to use by patients and physicians; The diary is perceived as useful for headache management by physicians and patients.
Methods
Ethical approval
Ethical approval of the project was obtained in the two lead headache centres (Pavia and Copenhagen). Every other participating centre used this approval to obtain additional approval from its own national or local ethics committee, as required by local regulations.
Development of the BDHD
The modified version of the BDHD was slightly adjusted by means of data obtained in the pilot study (14) and following the suggestions of headache experts and authoritative representatives of patient associations in Europe who participated in three consensus meetings held in Valencia, Spain in April 2006, Pavia in October 2006 and Stockholm, Sweden in June 2007. As with the earlier version, the modified BDHD collected information relevant to the ICHD-II diagnostic criteria for migraine, TTH and MOH (Figure 1A) and on the consumption of symptomatic medication, and included a set of simple, but detailed instructions (Figure 1B). Both the BDHD and the instructions, as well as a questionnaire assessing its acceptability, were written in English and subsequently translated into the languages of the participating centres. Translations involved two independent forward translations by bilingual translators and reconciliation by a headache expert fluent in English.
(A) The basic diagnostic headache diary; (B) instructions for the completion of the basic diagnostic headache diary.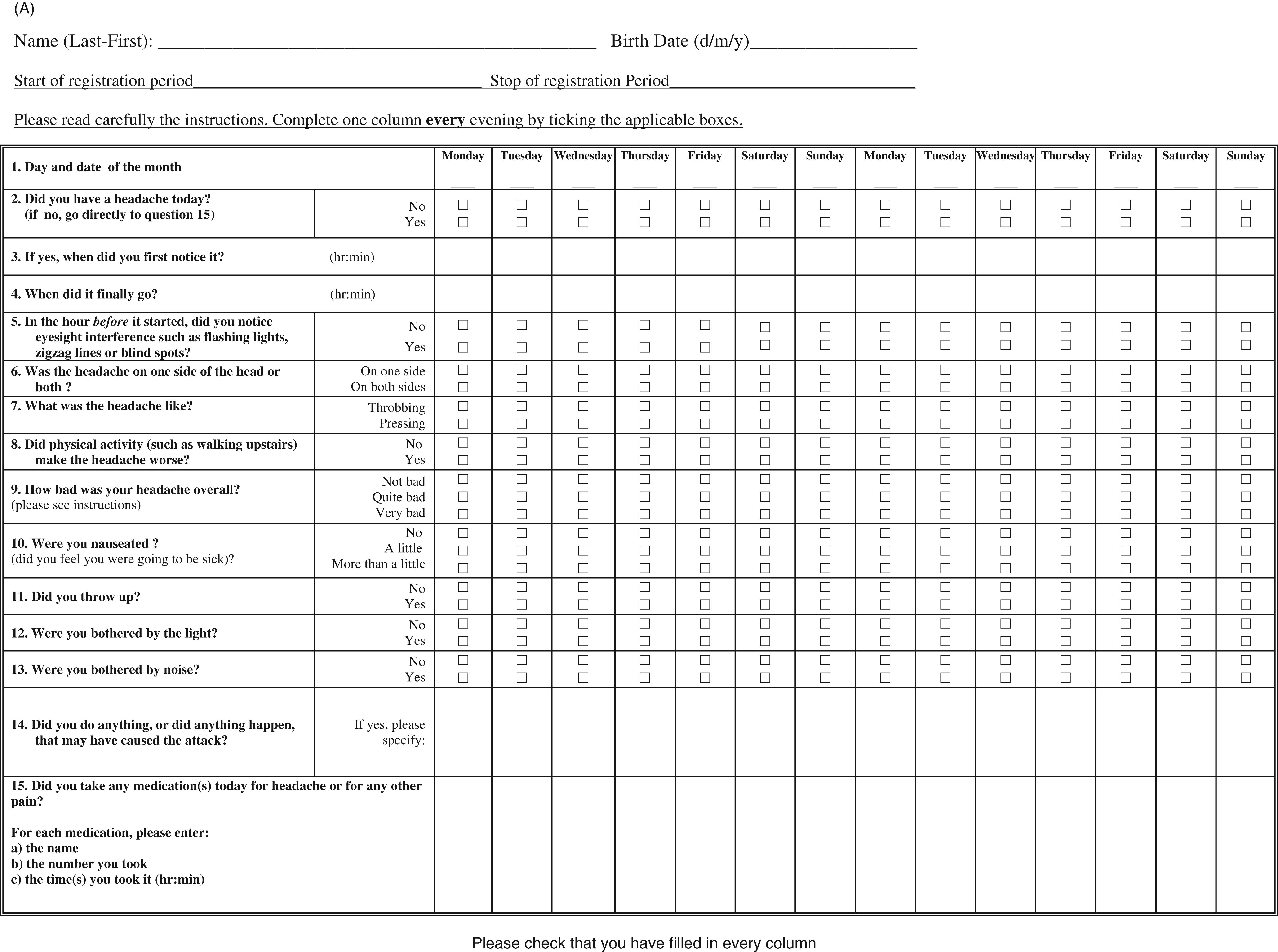
Evaluation
The study initially involved 20 headache centres from 14 countries in Europe and three from two countries in Latin America. Each centre was asked to enrol at least two blocks of 20 patients aged 18–65 years from their waiting lists between August 2007 and December 2008. Irrespective of their referral diagnosis, patients were allocated consecutively to one or the other of two groups according to a 1:1 randomization list:
Patients in group 1 were sent the BDHD by post, together with the set of instructions, at least 4 weeks prior to their first scheduled visit, and were asked to complete it each day for at least 4 weeks and bring it with them on the day of their appointment; Patients in group 2 made their first scheduled visit without having received the BDHD.
During the first scheduled visit, each patient in either group was diagnosed by a senior physician conducting the standard history taking and physical examination. For patients in group 1, the physician considered the additional information contained in the BDHD.
As in the pilot study, the criteria for chronic TTH and MOH were modified on account of the short recording period (12,13): chronic TTH was diagnosed when TTH was present on ≥ 50% of days in the recording period; MOH was diagnosed when headache was present on ≥ 15 days per month and when the medication overuse criteria were met.
At the end of the first visit, a questionnaire was given to group 1 patients to assess the usability and usefulness of the BDHD (Figure 2). Physicians were requested to complete another questionnaire on the completeness of data entry by patients and on the usability and usefulness of the BDHD from their viewpoint (Figure 3).
The patient questionnaire. The physician questionnaire.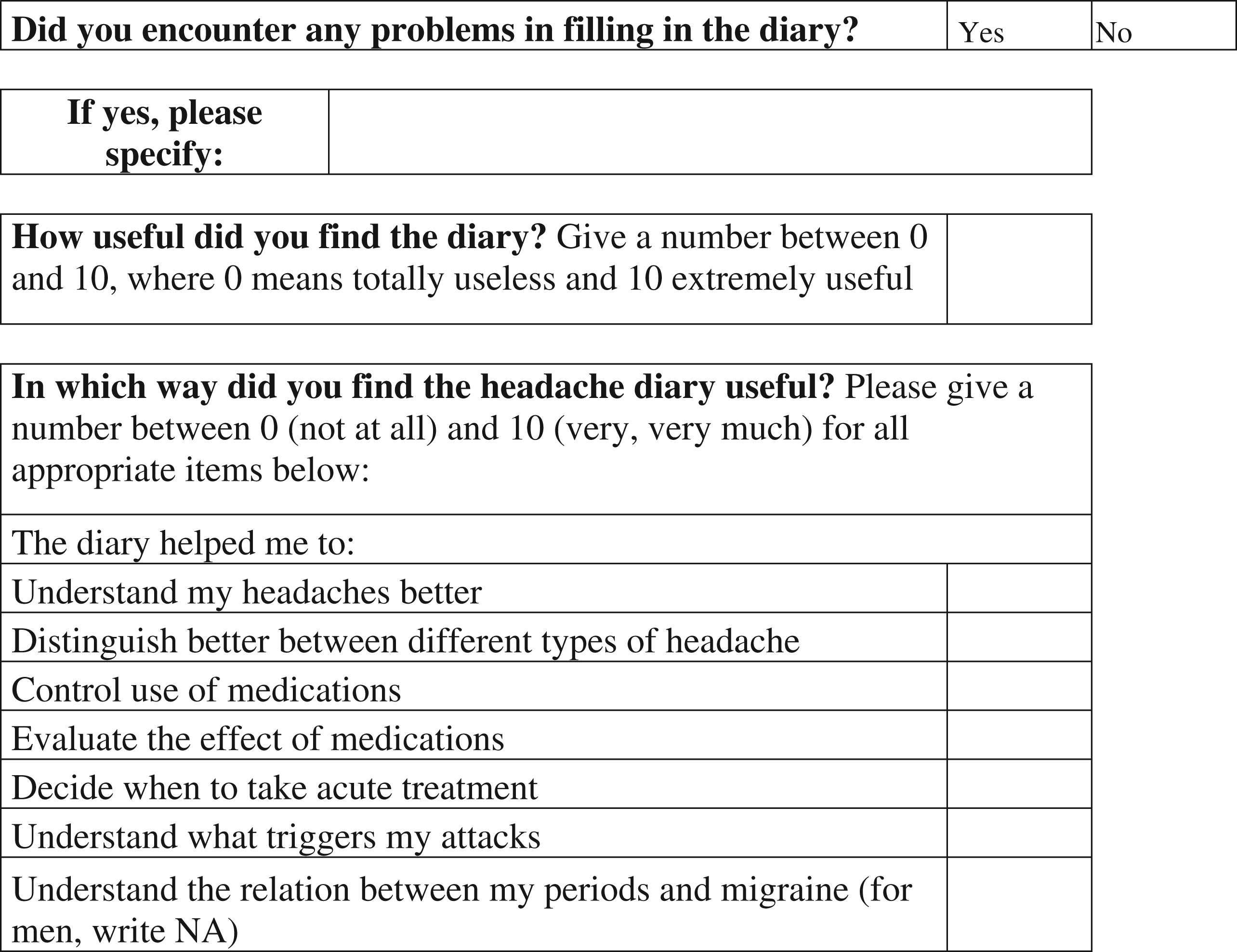

Data analysis and statistics
The following analyses were carried out:
Comparison of groups 1 and 2 for the number and nature of diagnoses; Comparison of diaries and physicians’ histories for data regarding the consumption of symptomatic drugs; Evaluation by physicians of the completeness of BDHD data: rated as complete when all the required information was present and incomplete when one or more items were missing; Evaluation by physicians of the adequacy of BDHD data for diagnosis: rated as adequate for diagnosis when all diagnostic criteria could be considered using only the information provided in the diary and inadequate when this information did not support a definite diagnosis; Evaluation by patients of the usability of the BDHD: rated as complete when a patient reported no difficulty in understanding it and in providing the required information and partial when a patient reported any issue with the BDHD; Evaluation by physicians of the usability of the BDHD: rated as complete when a physician reported no difficulty in interpreting data from it and partial when a physician reported any issue in interpreting data; Evaluation by patients of the subjective usefulness of the BDHD; Evaluation by physicians of the subjective usefulness of the BDHD.
All relevant data at each participating centre were collected in an electronic database and sent, after the end of the enrolment phase, to the Pavia centre for statistical analysis. Non-parametric tests were used for comparisons between groups (Mann–Whitney, Kruskal–Wallis tests and chi-square test) because of the skewed distribution of data. Statistical analyses were carried out using SPSS version 16.0 for Windows (SPSS Inc., Chicago, Illinois, USA).
Results
Patients enrolled by each participating country and adequacy of the BDHD + interview and interview alone

BDHD: basic diagnostic headache diary.
Indicates two centres per country. bIndicates three centres per country. cSix missing data, p < 0.001. There were no significant differences between countries.
Socio-demographic variables and headache features of patients by group a

Data are expressed as median, maximum and minimum value. NS: not significant.
Number, types and distribution of headache diagnoses by group

Data from 6 patients are missing. TTH: tension-type headache, MOH: medication overuse headache, NS: not significant.
Use of symptomatic drugs by group a

Data are expressed as median (minimum and maximum value). NS: not significant.
BDHD data were rated complete in 313 out of 321 cases (97.5%). The adequacy of BDHD data for diagnosis was rated complete in 95.9% of cases, with no significant differences between participating centres. BDHD data and clinical interview together yielded information considered complete for diagnosis in 97.7% of cases, whereas the information obtained from clinical interview alone in group 2 patients was considered complete in 86.8% of cases (p < 0.001); there were no significant differences between participating centres (Table 1).
Patient and physician usability of the basic diagnostic headache diary

Regarding the questionnaire on the usefulness of the BDHD, the records of 24 of 29 group 1 patients from Portugal were lost from the source database, so this country was excluded from this analysis. The majority of patients expressed positive evaluations of the usefulness of the BDHD for every proposed item, while significant differences emerged between different items (Kruskal–Wallis Test, H = 27.62; p < 0.0001). Patients evaluated the diary as especially useful for making them aware of medication usage and as less useful for understanding headache triggers or deciding when to treat headache (Figure 4). Significant differences also emerged between countries, with German patients providing the most negative impression and Latin American and Georgian patients expressing very positive ratings.
Patient evaluation of the usefulness of the basic diagnostic headache diary. Data are expressed as median values of the scores (0 not at all, 10 very much) for each of the six different items of the questionnaire. Kruskal–Wallis test: H = 27.62; p < 0.0001. Understand triggers: understand what triggers my attacks, When to treat: decide when to take acute treatment, Effect of med: evaluate the effect of medications, Awareness of med: become aware of the use of medications, Distinguish H: distinguish better between different types of headache, Understand H: understand my headaches better.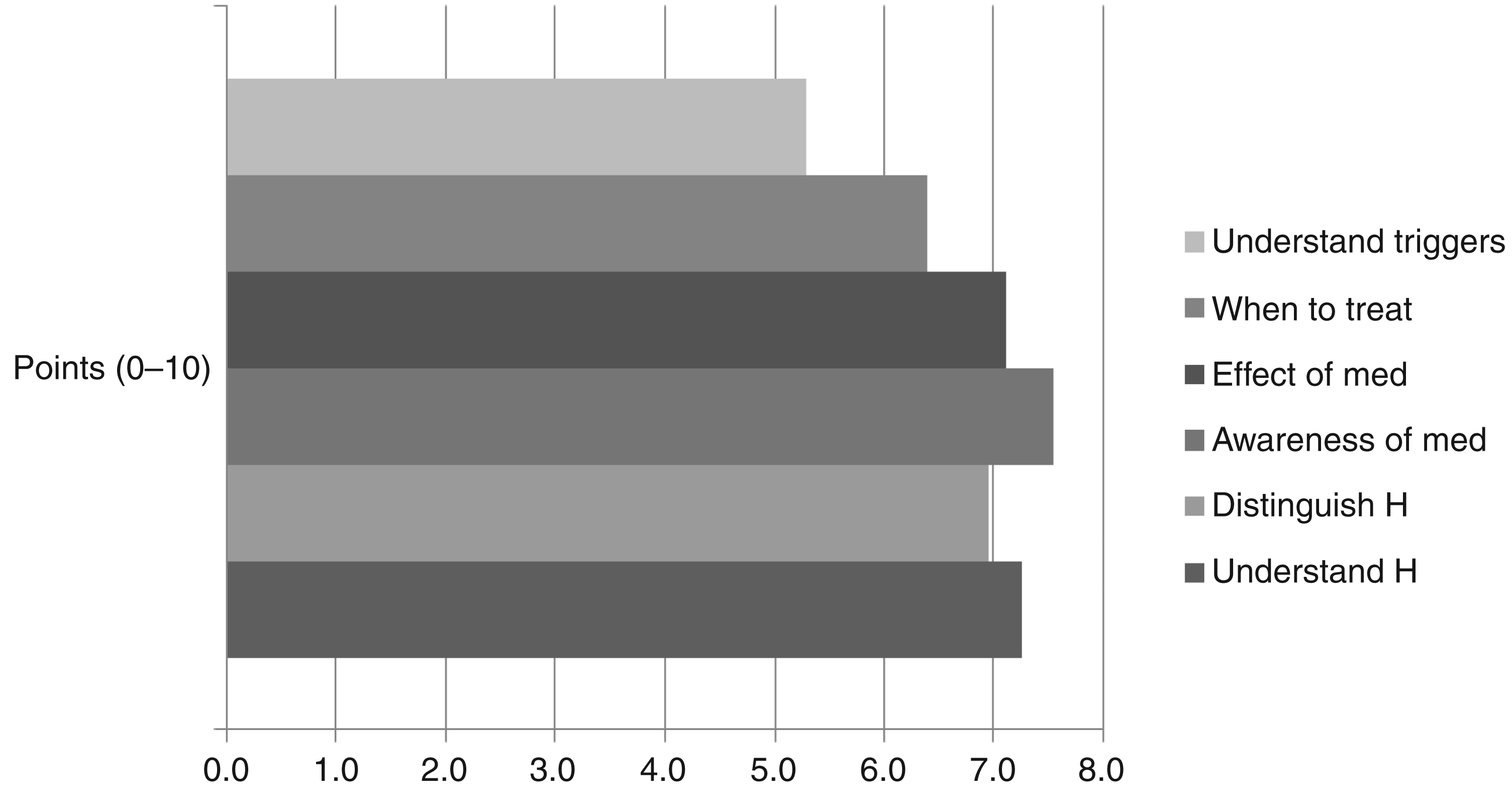
Physicians expressed very positive evaluations of usefulness for every item, but again significant differences emerged between items (Kruskal–Wallis test, H = 37.6; p < 0.0001): physicians evaluated the diary as very helpful in diagnosing MOH and in informing patients about medication intake, and as less useful in informing about headache triggers (Figure 5). Significant differences again emerged between countries, with Latin American, Serbian and Georgian physicians expressing the highest ratings and German and Italian physicians expressing the lowest.
Physician evaluation of the usefulness of the basic diagnostic headache diary. Data are expressed as median values of the scores (0 not at all, 10 very much) for the six different items of the questionnaire. Kruskal–Wallis test, H = 37.6, p < 0.0001. Inform about trigger: inform the patient about trigger factors, Inform about med: inform the patient about medication intake, Effect of med: evaluate the effect of medications, Diagnose MOH: diagnose overuse of medications, Distinguish H: distinguish better between different types of headache, Diagnose H: diagnose the headaches better.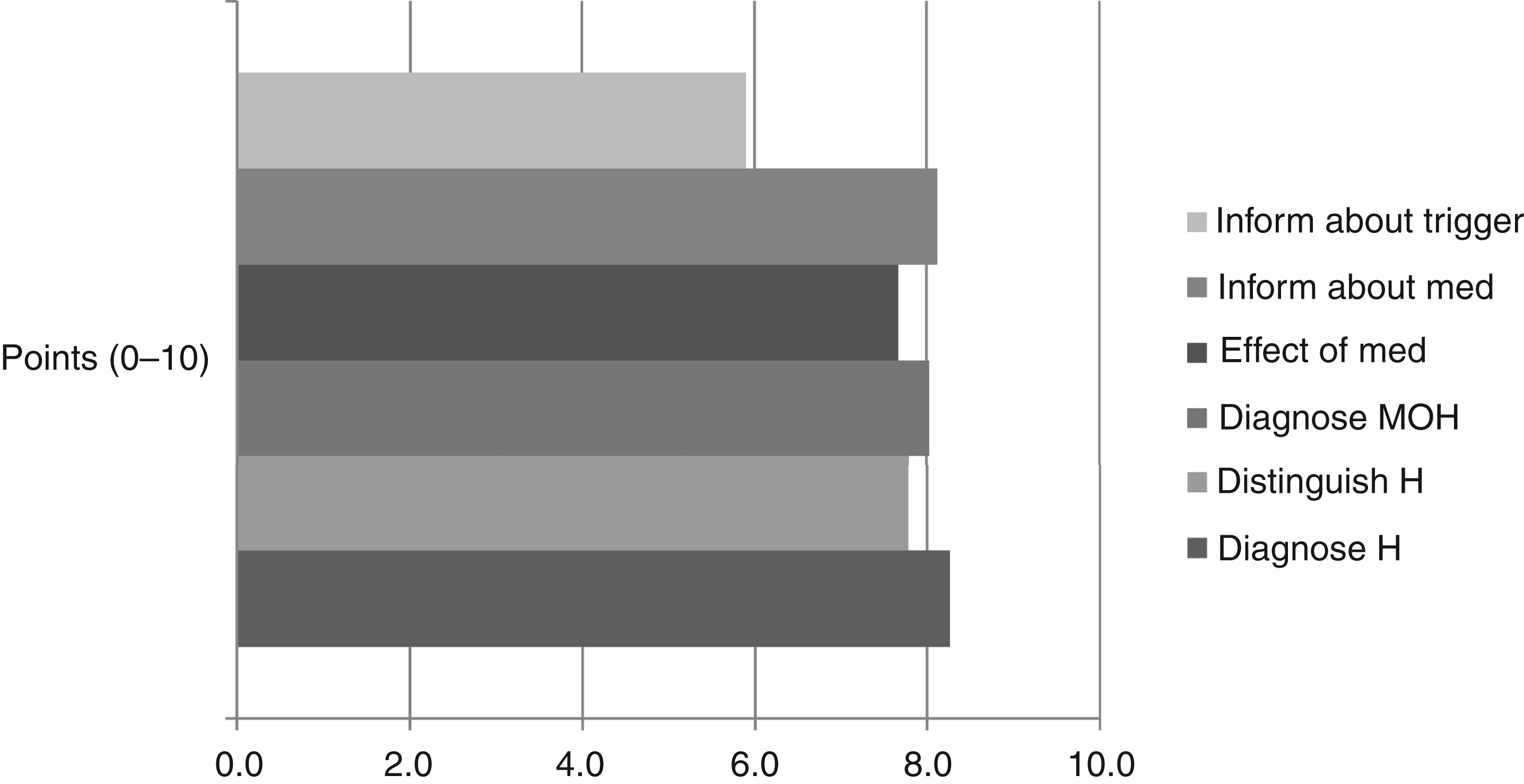
Discussion
In this study we tested the usability and usefulness of the BDHD, translated into eight languages, in the diagnosis of migraine, TTH and MOH in a large population of patients recruited in nine countries in Europe and Latin America. Following a pilot study (13), the BDHD was used in an innovative way, being completed by naïve patients waiting for their first scheduled visits to the participating headache centres. The only instructions received by the patients were those sent by post with the BDHD. The completion rate by patients was very high (97.5%, as rated by physicians). The same percentage of patients reported no difficulty in understanding the BDHD and in providing the required information. Physicians also reported very little difficulty in understanding and interpreting BDHD data (97% having no difficulty). Previous studies have reported unsatisfactory levels of compliance (14,15), a discrepancy that may reflect increased motivation in our patients, who were eager to use every resource available to ensure the best possible management from their first appointment and/or the provision of simple but detailed and easy-to-understand instructions on completing each single item of the BDHD.
The most interesting finding about BDHD usability is that, in combination with the clinical interview, the BDHD was adequate for the diagnosis of almost 96% of patients, with no differences between centres. The most remarkable finding regarding its usefulness was that the combination of BDHD data and clinical interview significantly increased the adequacy of the diagnostic process even beyond that of the ‘gold standard’ procedure. Furthermore, as found in other studies of diaries (6,13), the use of the BDHD supported an increase in diagnoses per patient – a clear benefit in headache centres where many patients have multiple headache disorders. In this study this was specifically due to an increased rate of diagnosing TTH (episodic, chronic or probable), a phenomenon probably explained by the common experience that, in the diagnostic interview, patients focus on their most severe headache attacks, forgetting to describe their milder ones.
Perhaps surprisingly, the prospective analytical record of medication usage intake in the BDHD did not lead to an increased number of diagnoses of MOH, and no significant difference was found in the usage of symptomatic drugs between the groups of patients diagnosed by the BDHD plus clinical interview and those diagnosed only by clinical interview. This finding may reflect the often-observed fact that chronic headache disorders occurring on ≥ 15 days/month are rather stable with regard to headache frequency and medication use, and indicate that, in clinical practice, little is lost by modifying the ICHD-II criterion for diagnosing MOH from 3 months of overuse to 1 month (as was done here). It does not suggest a lack of usefulness of the BDHD in MOH: rather, when asked, patients considered it as especially useful for ‘becoming aware of the use of medication’ and physicians considered it very helpful in ‘diagnosing MOH’ and ‘in informing the patients about medication intake’. Because the most reasonable strategy to manage MOH is to prevent its development (16), these findings may even indicate that the use of a diary can in itself have a preventive effect. Thus, the BDHD offers usefulness beyond diagnosis and appears to be an easy and well-accepted instrument for the instruction and monitoring of headache patients.
The identification of trigger factors or precipitants is frequently recommended as a basic strategy in the management of migraine and TTH (17,18). In our study, both patients and physicians, especially those from Germany and Italy, considered the BDHD less useful for understanding and informing about headache triggers than for other aspects of headache management. This finding was not unexpected because the BDHD was not designed to identify headache triggers (no list of triggers or other information about potential triggers was provided). From a practical point of view, this indicates that, for a deeper investigation of headache triggers, differently designed and specific diaries are necessary.
In the context of a generally positive perception of usefulness of the BDHD expressed by both patients and physicians, significant differences emerged between countries. For instance, German and Italian patients rated, on average, the diary as less useful in every single item when compared to Latin American, Serbian and Georgian patients, whereas less marked differences emerged between physicians. These differences possibly reflected variations in sociocultural identities and traditions, and should encourage researchers to perform studies of this kind on a national basis, and physicians to consider cultural diversity, to better meet their patients’ needs.
As with other tested diaries, some limitations are intrinsic to the use of the BDHD. For example, our diary should not replace the clinical interview and cannot replace the neurological examination, both being of key importance in the diagnosis of other primary headaches, particularly cluster headache and other short-lasting headaches, and, even more so, in the recognition of secondary headaches. In addition, the BDHD does not go beyond the first or second diagnostic level: therefore, it is necessary to develop new diaries for specific types of primary headache, for example, migraine with aura, menstrual migraine, trigeminal autonomic cephalalgias, or for particular populations, for example, children. Likewise, it maybe difficult to record hour-to-hour variation, peak intensities of pain and response to abortive medication in a BDHD. However, such diagnostic tools are created as a compromise between an acceptable level of detail and patient compliance over time. As discussed in the preliminary study (13), a delicate issue is also how long patients should keep a diary for before their first appointment. In this study we required this for only 4 weeks, which prompted the modification of the ICHD-II criterion for MOH. This was a deliberate compromise between practicality and ideal. This period may be too short for infrequent and variable forms of headache while, for the majority of patients with headache on ≥ 15 days/month, 3 months of systematic recording following the first visit very rarely changes the diagnosis based on 4 weeks’ worth of recordings. On the other hand, unnecessarily delaying the first visit of patients seeking advice for painful and disabling disorders is unkind, and represents poor management. Compliance with diaries suffers over longer periods, and selection bias among patients who complete diaries for 3 months may impair their usefulness as diagnostic tools. Future studies must address these issues.
These satisfactory findings regarding the usability and usefulness of the BDHD underline the desirability, whenever possible, of starting a diary before each patient's first consultation: it may provide additional educational value to the patient, as well as information to be integrated with the findings at interview; and, not least, it may shorten the time to definitive diagnosis and encourage more complete diagnosis (especially when multiple headache types coexist). It is important that the headache community uses the same diagnostic diary in order to standardize headache diagnosis. The diary presented here is the only one resulting from a dedicated developmental effort and also the only one with proven utility in many different countries and within different settings. We therefore suggest that the BDHD presented in this paper is adopted by headache centres and practising neurologists throughout the world.
In summary, we have demonstrated that the BDHD is a helpful tool in the diagnostic assessment of the most frequent and disabling types of primary headache. It is very well accepted and easy to use by patients and physicians, and is perceived as useful in headache management. This represents a major step towards achieving a homogeneous approach to the process of diagnosing headache in different countries and settings.
Footnotes
Funding
This research was partially supported by a grant from the European Commission (Eurohead Project) and by a grant from the Italian Ministry of Health (Ricerca Corrente 2008) to the Istituto Mondino.