
Abstract
Background
The present study aimed to investigate prescription patterns for patients aged over 17 years with headaches in the REZULT database.
Methods
We conducted a cross-sectional study (Study 1) of the proportion of over-prescription of acute medications (≥30 tablets/90 days for triptans, combination non-steroidal anti-inflammatory drugs (NSAIDs) and multiple types; ≥45 tablets/90 days for single NSAIDs) among patients with headache diagnosed in 2020. We longitudinally studied (Study 2) patients for >2 years from initial headache diagnosis (July 2010 to April 2022). The number of prescribed tablets was counted every 90 days.
Results
In Study 1, headache was diagnosed in 200,055 of 3,638,125 (5.5%) patients: 13,651/200,055 (6.8%) received acute medication. Single NSAIDs were prescribed to 12,297/13,651 (90.1%) patients and triptans to 1710/13,651 (12.5%). Over-prescription was found in 2262/13,651 (16.6%) patients and 1200/13,651 (8.8%) patients received prophylactic medication. In Study 2, 408,183/6,840,618 (6.0%) patients were first diagnosed with headaches, which persisted for ≥2 years. Over time, the proportion of patients over-prescribed acute medications increased. Over 2 years, 37,617/408,183 (9.2%) patients were over-prescribed acute medications and 29,313/408,183 (7.2%) patients were prescribed prophylaxis at least once.
Conclusions
According to real-world data, prophylaxis remains poorly prescribed, and both acute and prophylactic treatment rates for headaches have increased over time.
Introduction
Primary headaches are a widespread public health problem, with approximately 12% of migraine and up to 50% of tension-type headache (TTH) cases observed in the population (1,2). The International Classification of Headache Disorders, 3rd edition (ICHD-3) includes migraine, TTH and trigeminal autonomic cephalalgias as representative primary headaches, which greatly hinder patients’ daily activities. Primary headache management includes acute medications for headache attacks and prophylactic medications to reduce the frequency and severity of headache attacks (3). Inappropriate management without prophylactic medication for severe headache disorders sometimes increases the risk of chronic migraines, treatment resistance, comorbidities and medication-overuse headache (4,5). However, headache specialists remains few, and general physicians often treat primary headaches worldwide (6–9). Consequently, inappropriate and over-prescription of acute medications without the prescription of prophylactic medications is a concern.
Recently, National Health Insurance claims data-based research entailing numerous patient datasets as real-world data has been published (10–15). However, similar research in Japan is rare (16–18). Because big data research can shed light on inappropriate prescriptions by physicians in Japan, we investigated a health insurance database to clarify treatment patterns for headaches. In particular, using real-world data, we examined the over-prescription of acute medications by physicians. The present study differs from previous studies because of its large sample, cross-sectional evaluation of prescription patterns of acute medications in Japan and longitudinal evaluation of changes in prescription patterns, and the onset of over-prescriptions was investigated over 2 years from the time of first headache diagnosis.
Methods
All residents in Japan are required to have health insurance coverage offered by employee-based and community-based insurers, and the government sets fee schedules for medical services (16). Receipt data of employee-based insurers for >8 million patients have been registered in the REZULT database by Japan System Techniques Co., Ltd. Tokyo, Japan (https://www.jastlab.jast.jp/rezult_data). The REZULT database contains data on more than 420 million receipts from 147 insurance companies, permitting continuous longitudinal evaluation of prescriptions and treatments for patients for up to 12 years. It records the date, disease name for the insurance claim, age and sex of the patient, and medical treatment, including prescription and medical institution details. Each registered patient has an anonymous unique identification number, allowing complete prescription observation over time.
In Japan, combination analgesics and single analgesic agents can be purchased as over-the-counter (OTC) medicines. However, sales of triptans and prophylactic medication for migraine as OTCs are prohibited. In other words, prophylactic treatment and triptans can only be prescribed by physicians to patients diagnosed with migraines. Contrastingly, single and combination non-steroidal anti-inflammatory drugs (NSAIDs) can be prescribed for headaches without a migraine diagnosis. NSAIDs are also prescribed for other chronic pain disorders, including lower back pain. Unfortunately, the database used in the present study does not track the disease for which they were prescribed.
Study 1 (cross-sectional study): prescription pattern for patients with headache
Data were obtained from the REZULT database. We extracted data of patients aged >17 years with one-year continued diagnosis of headache (International Statistical Classification of Diseases and Related Health Problems (ICD)-10 code R51) or other headache syndromes (ICD-10 code G44) in 2020 and those who were prescribed certain medications listed in Table 1 to investigate the number of patients treated with an over-prescription of acute medications. No distinction was made based on whether or not the patient had a diagnosis of migraine (ICD-10 code G43). Drug price list codes are shown in supplementary File 1. Acute treatment was defined as the prescription of a single NSAIDS, a combination of NSAIDs or triptans. Prophylactic treatments included the prescription of lomerizine, propranolol, valproic acid, amitriptyline, verapamil and Japanese herbal Kampo medicine as defined by the Japanese guidelines (3). The number of tablets of acute medications prescribed from January 2020 to December 2020 was counted, and the proportion of over-prescriptions was evaluated. Referring to a previous report on triptan overuse (10), over-prescription was defined according to the ICHD-3 criteria as ‘use of triptans or combination NSAIDs on more than ten days (tablets) a month for three months (≥30 tablets/90 days), that of single NSAIDs on more than 15 days (tablets) a month (≥45 tablets/90 days) or that of any combination of single, combination and/or triptans (≥30 tablets/90 days) as well as one that does not constitute over-prescription for a single drug. As it was not possible to determine the number of days for which acute care drugs were actually used over the study period, ‘number of tablets per 90 days’ was counted instead of the ‘number of days per month when acute medications were used’.
Summary of acute and prophylactic medications.

The 90-day period for which the highest number of acute medications were prescribed was selected for each patient, and the prescription pattern was examined. Each table shows the prescribing pattern over the 90-day period when each drug was most prescribed. Prophylactic treatment was defined as ‘more than one tablet prescription during the 90 days’. Most prophylactic medications for headaches have multiple indications, including hypertension, epilepsy and depression.
Study 2 (longitudinal study): over-prescription during the 2 years from the initial diagnosis
We tracked changes in prescription patterns over 2 years from the initial headache diagnosis to determine how many individuals were over-prescribed with too many acute medications. Data for 6,840,618 patients aged over 17 years from the REZULT database who could be followed up for >2 years from the initial headache diagnosis (July 2010 to April 2022) were analysed. The number of prescribed tablets was counted every 90 days from the initial headache diagnosis. We analysed the proportion of patients who experienced over-prescription during the study period. Age, sex, time when patients fell into over-prescription of acute medication, prescription amount of the acute medication during the first 90 days and prescription of prophylactic medication during the first 90 days were investigated. A Mann–Whitney U-test was used to compare the number of medical facilities at which doctors prescribed headache medication, including whether or not the patient was over-prescribed over 2 years. Cox regression analysis was performed to identify factors related to the time for which patients were over-prescribed acute medication. No prescriptions for calcitonin gene-related peptide (CGRP)-related drugs were observed in the data set during this period.
Finally, an artificial intelligence (AI)-based model was developed as a sensitivity analysis, with the number of prescribed acute and prophylactic tablets in the first 90 days as the ‘explanatory variable’ and whether the patient was over-prescribed acute medications during the 2 years from the initial headache diagnosis as the ‘objective variable’. The model was developed as previously reported (19,20) and in accordance with relevant guidelines (21). The Python code is provided in supplementary File 2. The sensitivity, specificity, and area under the receiver operating characteristic (ROC) curve (AUC) were evaluated, and the accuracy of the model was evaluated. Important variables were evaluated by their gain, the common variables were statistically identified using Cox regression models and a sensitivity analysis was conducted.
Statistical analysis
Normal distribution was confirmed using the Shapiro–Wilk test. Variables with a normal distribution are presented as the mean ± SD, whereas those with a non-normal distribution are presented as the median (interquartile range). A log-minus-log plot was used to check whether the assumption of proportional hazards was satisfied. p < 0.05 (two-tailed) was considered statistically significant. SPS, version 29.0.0 (IBM Corp., Armonk, NY, USA), Python, version 3.9.0 (https://www.python.org/), Pandas, version 2.0.2 (https://pandas.pydata.org/), PyCaret, version 3.1.0 (https://pycaret.org/), scikit-survival, version 0.21.0 (https://scikit-survival.readthedocs.io/en/stable/) and Matplotlib, version 3.5.1 (https://matplotlib.org/) were used.
Ethics
The study was approved by the Itoigawa General Hospital Ethics Committee (approval number: 2022-2, 2022-10). The requirement for written informed consent was waived as a result of the anonymous and retrospective nature of the study. All experiments were performed in accordance with the tenets of the Declaration of Helsinki and conducted according to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines and the Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis guidelines.
Results
Study 1 (cross-sectional study): prescription pattern for patients with headache
Among 3,638,125 patients aged >17 years in the 2020 REZULT database, 200,055 (5.50%) were diagnosed with headaches via the health insurance system. Furthermore, 13,651/200,055 (6.82%) patients received at least one prescription of acute medication in 2020; their mean (SD) age was 31.82 ± 12.23 years with median 31 (range 18–74) years and 8889/13,651 (65.12%) were female. Single NSAIDs (acetaminophen and loxoprofen made up the majority) were the most frequently prescribed acute medications (12,297/13,651 patients; 90.08%) and triptans were prescribed to 1710/13,651 (12.53%) patients. Most patients received only acute treatment (12,451/13,651 patients; 91.21%) and 1200/13,651 (8.79%) patients received prophylactic treatment. The number of patients over-prescribed with at least one single NSAIDs (≥45 tablets/90 days), combination NSAIDs, triptans or combination of those (≥30 tablets/90 days) was 2262/13,651 (16.57%) (Table 2). Among 2262 over-prescribed patients, 303/2262 (13.40%) received prophylactic treatment.
Treatment pattern for headache patients.

NSAIDs, non-steroidal anti-inflammatory drugs.
Single NSAIDs were prescribed to 12,297/13,651 (90.08%) patients with headache (Table 3). The mean ± SD and median number of tablets of a single NSAIDs during 90 days were 27.63 ± 34.88 and 18, respectively. Prophylactic treatment was prescribed to 899/12,297 (7.31%) patients. The number of patients over-prescribed with a single NSAIDs (≥45 tablets/90 days) was 1739/12,297 (14.14%); however, the mean ± SD number of tablets was 87.44 ± 56.22. Among those patients, 174/1739 (10.01%) received prophylactic treatment.
Treatment pattern of single NSAIDs.

NSAIDs, non-steroidal anti-inflammatory drugs.
Combination NSAIDs were prescribed to 659 (4.83%) of 13,651 patients with headaches (see supplementary Table 1). The number of patients treated with over-prescriptions of combination NSAIDs (≥30 tablets/90 days) was 156/659 (23.67%). Among them, 24/156 (15.39%) patients received prophylactic treatment.
Triptans were prescribed to 1710 of 13,651 (12.53%) patients with headache (Table 4) and 106/1710 (6.20%) were over-prescribed with triptans (≥30 tablets/90 days). Among them, 44/106 (41.51%) patients received prophylactic treatment.
Treatment pattern of triptans.

NSAIDs, non-steroidal anti-inflammatory drugs.
Any combination of single, combination, and/or triptans, as well as one that does not constitute over-prescription for a single drug, was over-prescribed (≥30 tablets/90 days) to 296 of 13,651 (2.17%) patients with headache (see supplementary Table 2). Among them, 70/296 (23.65%) patients received prophylactic treatment.
Study 2 (longitudinal study): over-prescription during the study period
Among 6,840,618 patients from the REZULT database, 408,183 (5.97%) were first diagnosed with headaches and this diagnosis persisted for at least two consecutive years during the studied period (July 2010 to April 2022). The mean ± SD age was 35.23 ± 10.71 years, and 271,846 (66.60%) patients were women. During the first 90 days after headache diagnosis, 3258/408,183 (0.80%) patients received >45 tablets of a single NSAIDs, 188/408,183 (0.05%) received >30 tablets of combination NSAIDs and 91/408,183 (0.02%) received >30 tablets of triptans. At 22–24 months after the initial visit, the number of patients over-prescribed acute medications (≥30 or 45 tablets/90 days) increased (7733/408,183 patients, 1.89%) (Figure 1a and Table 5). Throughout the two years, 37,617/408,183 (9.22%) patients were over-prescribed acute medications in 90 days at least once.

Prescription pattern during the two years from the initial diagnosis. (a) Percentage of over-prescriptions with acute medications. Two years after the initial visit, the number of patients over-prescribed with acute medications (≥30 or 45 tablets/90 days) increased with time. During the two years, 37,617/408,183 (9.22%) patients were over-prescribed with many acute medications in 90 days on at least one occasion and (b) Percentage of prescriptions for prophylactic medication. During the two years, 29,313/408,183 (7.18%) patients were prescribed prophylactic medication on at least one occasion.
Changes in prescribing patterns over time.
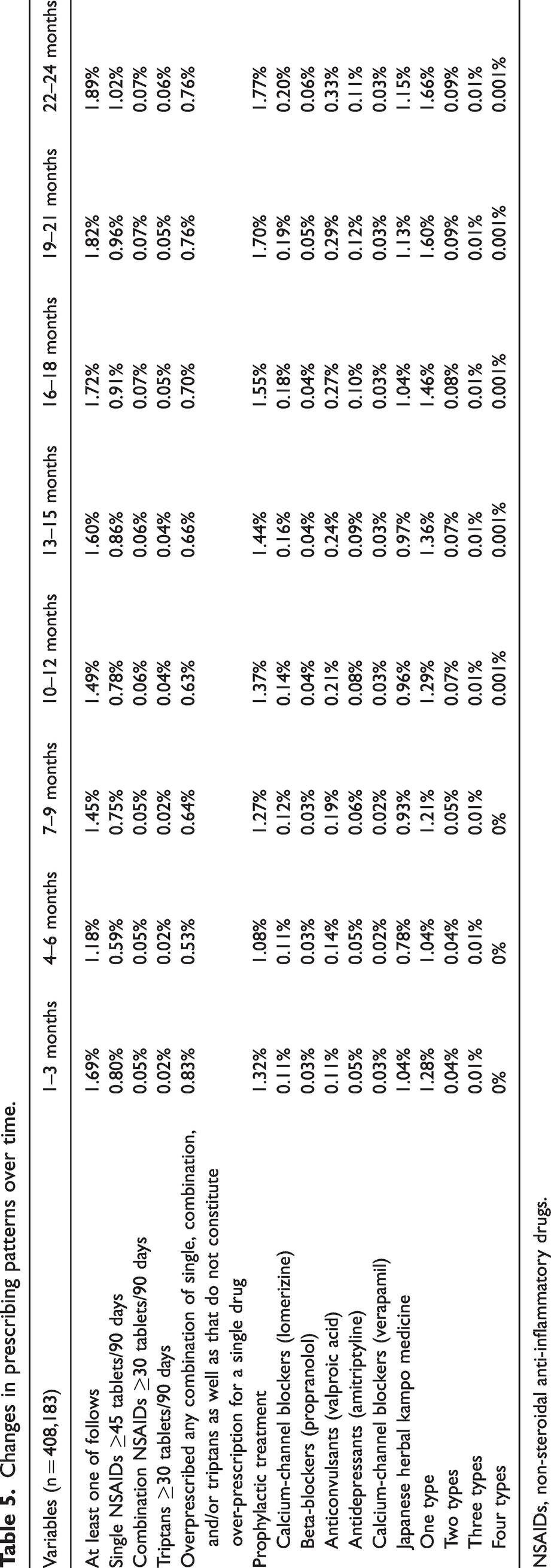
NSAIDs, non-steroidal anti-inflammatory drugs.
Prophylactic medication was initiated in the first 90 days in 5388/408,183 (1.32%) patients, which increased to 7208/408,183 (1.77%) patients after 2 years (Figure 1b). Throughout the 2 years, 29,313/408,183 (7.18%) patients with headaches were prescribed prophylactic medications on at least one occasion. The details of the prescription pattern for the 2 years from the initial diagnosis are shown in Table 5.
Among 408,183 patients, 37,617 (9.22%) were over-prescribed medications during the 2-year observational period. The mean ± SD age was 36.58 ± 10.71 years, and 25,039/37,617 (66.56%) patients were female. The mean ± SD duration of the first instance of over-prescription was 4.29 ± 2.02 terms of 90 days, conprising approximately 12–15 months (Figure 2a). The mean ± SD number of medical facilities at which doctors prescribed headache medication without over-prescription was 1.14 ± 0.45 (range 1–8) and those facilities that over-prescribed (1.52 ± 0.85, range 1–11) differed significantly (p < 0.001). Sub-analysis revealed that the number of patients over-prescribed with a single NSAIDs (≥45 tablets/90 days), combination NSAIDs, triptans, or any combination of single, combination and/or triptans, as well as that not constituting over-prescription for a single drug (≥30 tablets/90 days), was 19,820/408,183 (4.86%), 1,101/408,183 (0.27%), 842/408,183 (0.21%) and 20,108/408,183 (4.93%), respectively.

Cox regression analysis for over-prescription during the two years from the initial diagnosis. (a) Trends in over-prescription in patients with a persisting headache diagnosis for two years from the initial diagnosis. (b) Patients prescribed prophylactic medication in the first three months were more likely to be over-prescribed. Sub-analyses for (c, d) single non-steroidal anti-inflammatory drugs (NSAIDs), (e, f) combination NSAIDs, (g, h) triptans and (i, j) any combination of single, combination and/or triptans, as well as any that do not constitute over-prescription for a single drug. x-axis, time; y-axis, proportion of over-prescription.
According to the sub-analysis, 3064/408,183 (0.75%) patients remained over-prescribed with a single NSAIDs (≥45 tablets/90 days) for two terms (4–6 months), 350/408,183 (0.09%) patients for four terms (10–12 months) and 18/408,183 (0.01%) patients for eight terms (22–24 months). Then, 286/408,183 (0.07%) patients remained over-prescribed with combination NSAIDs (≥30 tablets/90 days) for two terms (4–6 months), 59/408,183 (0.01%) patients for four terms (10–12 months) and 4/408,183 (0.001%) patients for eight terms (22–24 months). Also, 136/408,183 (0.03%) patients remained over-prescribed with triptans (≥30 tablets/90 days) for two terms (4–6 months), 15/408,183 (0.01%) patients for four terms (10–12 months) and no patients for eight terms (22–24 months). Finally, the number of patients who remained over-prescribed with any combination of single, combination and/or triptans, as well as that not constituting over-prescription for a single drug (≥30 tablets/90 days), was 877/408,183 (0.21%) for two terms (4–6 months), 11/408,183 (0.01%) for four terms (10–12 months) and zero for eight terms (22–24 months).
Cox regression analysis revealed that older age, more prescriptions of single, combination NSAIDs and triptans in the first three months, and prescription of prophylactic medication during the first three months were related to early over-prescription in the two years (all p < 0.001) (Table 6). Early use of prophylactic medication during the first three months (n = 5388/408,183 patients; 1.32%) was related to early over-prescription (Figure 2b). Sub-analyses for single NSAIDs, combination NSAIDs, triptans or any combination of single, combination and/or triptans, as well as that not constituting over-prescription for a single drug, showed similar trends (Figure 2c–h and Table 6). Log-minus-log plots confirmed that the assumption of proportional hazards was satisfied (see supplementary Figure 1).
Hazard ratio for overprescription using Cox regression.
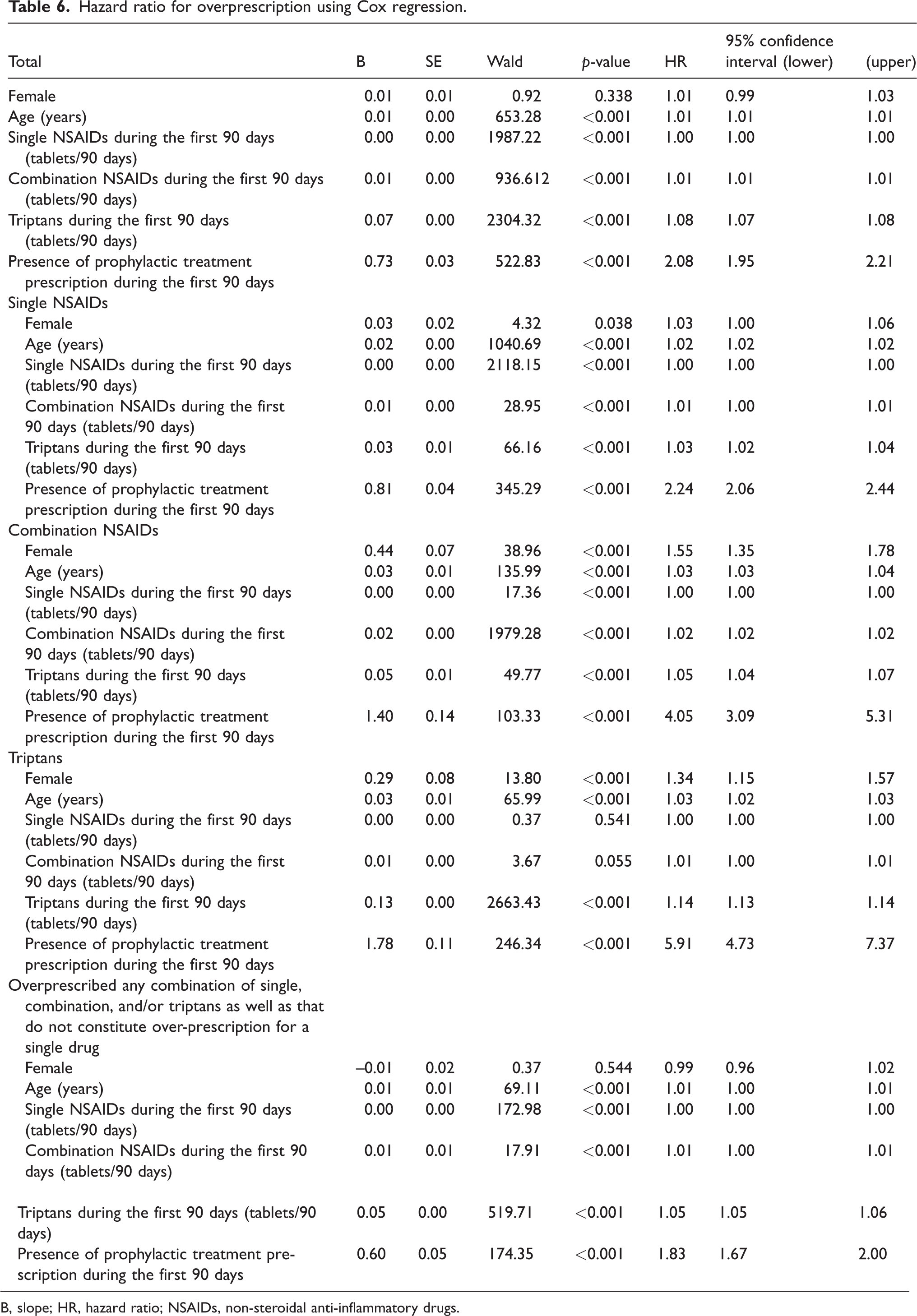
B, slope; HR, hazard ratio; NSAIDs, non-steroidal anti-inflammatory drugs.
For sensitivity analysis, we developed an AI-based model predicting the occurrence of over-prescriptions during the two years from the initial headache diagnosis based on the prescription amount in the initial 90 days. A gradient-boosting classifier was used. The confusion matrix is shown in Figure 3a. Sensitivity and specificity were 20.36% and 99.97%, respectively. The micro- and macro-average AUC of the ROC were 0.95 (95% confidence interval (CI) = 0.92–0.98) and 0.79 (95% CI = 0.70–0.88), respectively (Figure 3b). The important variables and their gains are shown in Figure 3c. Single NSAIDs, triptans, combination NSAIDs, Japanese herbal Kampo medicine, lomerizine, verapamil, propranolol, amitriptyline, valproic acid (tablets or packets/90 days for all) and sex were significant in that order. The learning curve and calibration plot are shown in Figure 3d,e. Of the survival prediction model using random survival forest, Harrell’s concordance index (22) was 0.80. In other words, this AI-based predictive model was highly accurate, and its important variables (Figure 3c) were similar to those that were identified as important in Cox regression analysis (Table 6).

Performance of the artificial intelligence (AI)-based model to predict over-prescription. (a) Confusion matrix. (b) Micro- and macro-average area under the curve (AUC) of the receiver operating characteristic curve (ROC). (c) The important variables and their gains. (d) Learning curve and (e) Calibration plot.
Discussion
We used the big health insurance REZULT database to perform two investigations on prescription patterns of headache medications. First, in the cross-sectional study, among 13,651 patients diagnosed with headaches and treated with prescribed medication in 2020, only 1200/13,651 (8.79%) received prophylactic medication. The number of patients over-prescribed with at least one single NSAIDs, combination NSAIDs or triptans was 2262/13,651 (16.57%). Second, in the longitudinal study, we evaluated 408,183 patients diagnosed with headaches, which persisted for at least two consecutive years. Throughout these two years, 37,617/408,183 (9.22%) patients were over-prescribed acute medications in 90 days on at least one occasion, and 29,313/408,183 (7.18%) patients were prescribed prophylactic medications on at least one occasion. Patients with over-prescription were prescribed headache medications by multiple healthcare providers compared with those that were not over-prescribed. Notably, early use of prophylactic medication during the first three months (5388/408,183 patients, 1.32%) was related to early acute medication over-prescription. Younger age, more prescriptions of single, combination NSAIDs and triptans in the first three months were also related factors.
Investigation of foreign health insurance claims databases
In the present study, we describe recent reports on triptan over-prescription because, unlike NSAIDs, triptans cannot be prescribed without a diagnosis of migraine in Japan. Analysis of the Dutch Health Care Insurance Board Database of 2005, comprising data for 46% of the total population, revealed that triptans were used by 1.3%, and 10.4% of these were suspected overusers. They also found that almotriptan tended to be overused, whereas sumatriptan was not (10). An investigation of the French General Health Insurance System in 2010 and 2011 revealed that 2243 of 99,450 patients (2.3%) prescribed with triptans could be overusers. Older age and the use of prophylactic medications, benzodiazepines and antidepressants were risk factors for triptan overuse (15). A 2012 study conducted in two provinces in Italy showed that approximately 10% of triptan users were frequent users (≥10 tablets/month). Approximately two-thirds of the frequent users maintained their frequent triptan use for an additional three months (14). An Austrian research of 5,918,487 people found that 0.56% were triptan users and 6.0% were overusers. Overusers were older than non-overusers (12).
Compared with results of reports worldwide, our results showed similar trends. Triptans were prescribed to 1710 of 13,651 (12.53%) patients with headaches; 106/1710 (6.20%) were suspected overusers. Therefore, awareness of the appropriate use of triptans and prevention of overuse/over-prescription are needed worldwide.
Previous Japanese studies using health insurance claims data
Meyers et al. (16) investigated patients with migraines and their treatment patterns using data from the Japan Medical Data Centre database. In three years, among 16,433 patients with migraines, 9873 (60.1%) received only acute medication, 3022 (18.4%) received prophylactic medications and 3548 (21.6%) were not prescribed any medication. After 61.2 ± 65.3 days of initial prophylactic treatment, 62.2% patients discontinued it; among them, 15.2% reinitiated the initial treatment and 7.0% switched the treatment regimen within one year. Therefore, the use rate of prophylactic medications was low, with a high discontinuation rate following a brief treatment period. Additionally, we observed lower prevalence (1.4%) of migraines than previous prevalence studies (23). This underestimation may be because 69.4% of patients with migraines had never consulted a physician for headaches, and only 11.6% of patients were aware that their headaches were migraines (23). Calcium channel blockers and anticonvulsants were the most common prophylactic medications reported in the database. In the present study, although the prevalence of migraine could not be directly compared with the study by Meyers et al. (16) because of the different sampling methods, the lower prevalence of migraine compared with that in previous epidemiological studies (23,24) could be for the same reasons; patients with migraine may have refrained from seeing a doctor (2) or those who did may not have been prescribed prophylactic medications (25). Furthermore, Japanese herbal Kampo medicines (4) were most commonly prescribed; however, besides that, the trends appeared to be similar. By contrast to the findings of Meyer et al. (16), in the present study, the rate of prescriptions for preventive medications increased over time (Figure 1 and Table 5). Our patients retained their headache diagnosis for two years; therefore, they may have been treated longer than patients in Mayer’s study, which may have caused titration of acute and prophylactic medications.
Sakai et al. (17) investigated anonymised online survey data coupled with medical claims data of individuals aged 19–74 years. Migraine prevalence was 3.2% (691/21,480) and was the highest among 30–39-year-olds. Among them, 81.0% (560/691) of patients did not consult a doctor and 57.8% (362/691) used OTC drugs only. However, only 6.1% (38/691) of patients used prescription medicines. The findings of an epidemiological study conducted 20 years ago (23), as well as those of another study (17) suggested that, even with the advent of triptans and CGRP-related drugs and the paradigm shift that has occurred, a lack of appropriate consultation behaviour and use of prophylactic treatment persist (26).
Hirata et al. (18) analysed prevalence and burden according to headache subtypes in 21,480 patients. They noted that the irrational behaviour of refraining from seeing a doctor was observed in all headache subtypes. By combining an epidemiological and a questionnaire survey, the researchers reported that patients with headaches are still burdened by the disease, refrain from seeing their doctors, and do not receive prophylactic treatment. The few patients for whom prophylactic treatment was prescribed was similarly noted in our study.
Timing of initial consultation
Generally, prophylactic medications should decrease the frequency and severity of headaches and reduce the frequency of acute care medications (3). However, in our longitudinal study, the group receiving prophylactic treatment within the first 90 days experienced over-prescription of acute medications earlier than the group that did not receive prophylactic medications. This suggests that patients who potentially require follow-up for >2 years may have had their first hospital consultation when the migraine had already progressed and become intractable.
It has been proposed that migraine is a progressive disease (27). Episodic migraine is estimated to progress to chronic migraine at a rate of 2.5% per year and may be underestimated as a result of the diagnostic criteria for chronic migraine, which remains under debate (28). Factors associated with migraine progression include a high frequency of migraine attacks, medication overuse, comorbid pain syndromes and obesity (27). We observed a similar trend: patients with prescriptions of combination NSAIDs and triptans in the first three months were related to early over-prescribing of acute medications.
Hirata et al. (18) found that 14–38% of patients with headaches did not visit a hospital because of the effectiveness of OTC medicines. By contrast, some patients first visited a doctor because OTC had become ineffective (48/691, 6.9%) or their headaches had increased in frequency (55/691, 8.0%). Prophylactic treatment can be terminated relatively early after migraine remission (3,4,17). Prophylactic treatment is not well-performed in Japan (1,25). We hypothesised that patients who encourage their physicians to prescribe prophylactic treatments and those for whom early prophylactic treatment is prescribed may have already begun to develop chronicity from the initial consultation. If so, further educational efforts (2,29) are needed, and patients should consult doctors during the period when they have relatively mild episodic migraine.
A similar trend is suspected in other countries. One study showed that approximately one in three migraine patients take acute prescription medications for a migraine attack, whereas less than one in five patients take preventive prescription medications (9). Additionally, misdiagnosis and delayed diagnosis of chronic migraine are problematic (30). Although the situation differs from country to country regarding accessibility to medical care, differences in advertising methods and different drugs available through insurance, similar trends may be applicable worldwide, given that reports similar to Japan's have been published from various countries (31,32). Large-scale longitudinal surveys are expected in the future.
Number of medical facilities visited
In clinical practice, patient education is important; however, obtaining a long-term perspective is difficult, and patients often drop out and avail of multiple medical services (33). Our results showed that patients were over-prescribed headache medications, and these prescriptions may have been provided by multiple healthcare providers. This may cause a lack of trust in doctors and healthcare facilities. In the future, it will be necessary to build trust between doctors and patients and plan treatment based on shared decision-making (34).
Limitations
This study had some limitations. First, it has a sampling bias. In cross-sectional Study 1, we selected a 90-day period during which the highest number of acute medications (tablet number) were prescribed. Additionally, because it was impossible to determine the number of days for which the acute medications were actually used over the study period, ‘number of tablets per 90 days’ was counted instead of the ‘number of days per month when acute medications were used’. Although this calculation method was based on previously established methodology (10), accurate recording using headache diaries or other methods is desirable. In longitudinal Study 2, we selected patients who continued to be labelled with headaches for two years after their first diagnosis. This may have resulted in a large number of patients with relatively severe headaches. Additionally, severely ill patients may have been included when their migraines had already begun to progress. Moreover, because NSAIDs were not only prescribed for headaches, patients who were regularly prescribed analgesics for other types of chronic pain, including back pain, could not be excluded. Therefore, for studying migraines specifically, it may be better to focus only on triptans in future studies.
Second, a retrospective analysis of administrative claims data for billing was performed. Patients were identified only based on information available in the database, and we could not determine migraine severity, the actual number of medications taken per day, and OTC medicine use. Some migraine treatments have multiple indications (e.g. anticonvulsants and antidepressants) and patients may have been incorrectly considered to have received treatment for migraine, when it was actually intended for another comorbid condition.
Third, we could not track those patients who used insurance systems not included in the REZULT database. Fourth, it was impossible to identify patients with only migraine because all types of headaches were put under one category; reanalysis of only migraines will be further considered. The apparent prevalence of headache disorders may have increased because the disease was named for the sake of insurance claims, and the disease labels were kept or forgotten to be removed. Fifth, 21.6% of patients with migraines were not prescribed medications in a previous health insurance-based study (16) and such patients could not be evaluated. Sixth, it is undeniable that a large percentage of medication-overuse headaches attributed to multiple drug classes not individually overused (ICHD-3 code 8.2.6) patients may be overcounted as a result of the method of counting the number of tablets. Finally, we will continue to track how this prescribing pattern changes with headache awareness (2) and the introduction of new drugs, including CGRP-related drugs and lasmiditan.
Conclusions
We used REZULT, a big health insurance database, to investigate prescription patterns in headaches and found that only 8.79% (1200/13,651) of patients diagnosed with headaches received prophylactic medication. Among patients who received acute medications (NSAIDs or triptans), 16.57% (2262/13,651) were over-prescribed. In the two-year longitudinal study, 10.76% (37,617/408,183) of patients were over-prescribed acute medications and 29,313/408,183 (7.18%) patients with headaches were prescribed prophylactic medications in 90 days on at least one occasion. Early use of prophylactic medication during the first three months, younger age, more prescriptions of single, combination NSAIDs and triptans in the first three months were related to early over-prescription.
Clinical implications
Among 13,651 patients with headache and with prescriptions, 16.6% were over-prescribed acute medications (NSAIDs or triptans). In 408,183 patients with headaches for two consecutive years, 10.8% were over-prescribed acute medications during 90 days on at least one occasion. Throughout the two-year period, 7.2% of the 408,183 patients with headache were prescribed prophylactic medications on at least one occasion.
Supplemental Material
sj-xlsx-1-cep-10.1177_03331024231226177 - Supplemental material for Treatment patterns and characteristics of headache in patients in Japan: A retrospective cross-sectional and longitudinal analysis of health insurance claims data
Supplemental material, sj-xlsx-1-cep-10.1177_03331024231226177 for Treatment patterns and characteristics of headache in patients in Japan: A retrospective cross-sectional and longitudinal analysis of health insurance claims data by Masahito Katsuki, Yasuhiko Matsumori, Taisuke Ichihara, Yuya Yamada, Shin Kawamura, Kenta Kashiwagi, Akihito Koh, Tetsuya Goto, Kazuma Kaneko, Naomichi Wada and Fuminori Yamagishi in Cephalalgia
Supplemental Material
sj-pdf-2-cep-10.1177_03331024231226177 - Supplemental material for Treatment patterns and characteristics of headache in patients in Japan: A retrospective cross-sectional and longitudinal analysis of health insurance claims data
Supplemental material, sj-pdf-2-cep-10.1177_03331024231226177 for Treatment patterns and characteristics of headache in patients in Japan: A retrospective cross-sectional and longitudinal analysis of health insurance claims data by Masahito Katsuki, Yasuhiko Matsumori, Taisuke Ichihara, Yuya Yamada, Shin Kawamura, Kenta Kashiwagi, Akihito Koh, Tetsuya Goto, Kazuma Kaneko, Naomichi Wada and Fuminori Yamagishi in Cephalalgia
Footnotes
Acknowledgements
We are thankful for the help provided by the medical staff.
Data availability
The datasets generated and/or analysed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
Masahito Katsuki received personal consultancy fees from Amgen Astellas BioPharma K.K., Daiichi Sankyo Company, Limited, Eli Lilly Japan K.K. and Otsuka Pharmaceutical Co., Ltd. during the conduct of the study.
Yasuhiko Matsumori received personal consultancy fees from Amgen Astellas BioPharma K.K., Daiichi Sankyo Company, Limited, Eli Lilly Japan K.K. and Otsuka Pharmaceutical Co., Ltd. during the conduct of the study.
Taisuke Ichihara and Yuya Yamada are employees of Japan System Techniques Co. Ltd.
The other authors report no conflicts of interest concerning the materials or methods used in this study or the findings presented in this paper. This article and contents of this study were not published nor presented previously.
Funding
The study was funded by Bio-Medicines, Japan Drug Development & Medical Affairs at Eli Lilly Japan K.K.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.