
Abstract
We present a prospective 4-year follow-up study of 96 patients with medication overuse headache following withdrawal. Complete datasets were available from 85 patients (89%) 6 months, from 79 patients (82%) 1 year and from 75 patients (78%) 4 years after withdrawal. Twenty-six patients (31%) relapsed within the first 6 months after withdrawal. The number of relapses increased to 32 (41%) 1 year and to 34 (45%) 4 years after withdrawal. The 4-year relapse rate was lower in migraine than in tension-type headache (32% vs. 91%, P ≤ 0.001) and combination of migraine and tension-type headache (32% vs. 70%, P ≤ 0.027) and also lower in patients overusing triptans than analgesics (21% vs. 71%, P ≤ 0.001). The study suggests that the majority of relapses occur within the first year after withdrawal and that the long-term success of withdrawal depends on the type of primary headache and the type of overused medication.
Introduction
Medication overuse headache (MOH) is a chronic headache (≥15 days/month) which develops following overuse of acute headache medication and vanishes after withdrawal (1). Although the vast majority of patients report an improvement of headache shortly after withdrawal, long-term studies indicate that 30–45% of them relapse and develop MOH again despite of an initially successful withdrawal therapy (2–14). Rates of relapse between 22% and 44% were found during the first year after withdrawal (3, 6, 7, 9). Studies with longer observation periods of up to 6 years reported relapse rates of between 24% and 43% (2, 4, 5, 8, 10–14), indicating that the majority of relapses occur within the first year after withdrawal. This hypothesis, however, has not been confirmed prospectively in a longitudinal study.
Another important issue in patients with MOH is the evaluation of possible predictors for relapse. The above-mentioned studies reported contradicting results. Only few studies had a prospective design (3–5, 8–10). Most of them were performed in the 1980s or early 1990s and did not cover triptan-induced MOH.
Therefore, the aim of the current study was to assess the rate of relapse and to evaluate possible predictors of relapse in patients with MOH after initially successful withdrawal. Furthermore, the prospective longitudinal study design enabled us to identify the most critical period for relapse. Data for this patient cohort regarding clinical features of MOH (15), clinical features of withdrawal (16) and 1-year follow-up (9) have been published previously.
Methods
The study was approved by the ethics committee of the University of Essen, Germany. Written consent was obtained from all patients prior to enrolling in the study. Study design and demography of the patient population were published previously (9, 15, 16).
Patients
Briefly, 98 patients with MOH (International Headache Society criteria) were included in the study (15). Patients with major depression as well as patients overusing more than one headache drug on more than 5 days per month were excluded. All patients underwent standard in-patient withdrawal (9).
Study design
The following baseline items were documented: (i) demography; (ii) type and duration of primary headache [migraine (MH), tension-type headache (TTH) and combination of migraine and tension-type headache (CH)]; (iii) type of overused medication as well as frequency and duration of drug intake. Overused medication was divided into analgesics, ergots and triptans; and (iv) preventive and acute treatment at time of discharge.
Six-month, 12-month and 4-year follow-up
Follow-ups were performed by a telephone interview using a standard questionnaire. The following items were assessed: (i) frequency and intensity of primary headache; (ii) presence of daily headache; (iii) type and frequency of currently used acute headache medication; (iv) type of currently used preventive medication and compliance of drug intake. Relapse was defined as frequent use of any kind of acute headache medication on more than 15 days per month for at least 3 months.
Statistical analysis
Relapse rates independent of duration of primary headache and duration of drug overuse (interval data) were compared using two-sample t-tests. Comparison of relapse rates independent of type of primary headache and type of overused acute headache medication (ordinal data) was performed by χ2 test (Fisher's exact test). Because of multiple testing (four tests) the level of significance was adjusted to P < 0.0125. All statistics were calculated with the SPSS program (9.0.1).
Results
Patient population
Demographic and clinical characteristics of the patient population have been reported previously (9, 15). Two of 98 patients did not improve 1 month after withdrawal and were excluded from the study. Of the remaining 96 patients, 78 women and 18 men, with mean age 43 years (range 23–65 years), 69 (71%) suffered from MH, 13 (14%) from TTH and 14 (15%) from a combination of MH and TTH. Mean duration of primary headache was 22 years (range 3–44 years). Forty-six (48%) patients overused analgesics, 12 (13%) ergots and 38 (39%) overused triptans. Mean duration of drug overuse was 6.5 years (range 0.5–25 years).
Follow-up data
Six months after withdrawal complete datasets were available from 85 patients (89%), after 12 months from 79 patients (82%), after 4 years from 75 patients (78%). No significant differences in demographic and clinical parameters (gender, age, type of primary headache, type of overused medication, duration of primary headache and duration of drug overuse) were found between available patients and those who were lost to follow-up.
Relapse rates
Twenty-six patients (31%) relapsed within 6 months, six additional patients (32 patients, 41%) within 1 year and two subsequent patients (overall 34 patients, 45%) 4 years after withdrawal. Hence, 94% (32 of 34) of patients relapsed within the first year after withdrawal (Fig. 1).

Time course of relapse in patients with medication overuse headache 6 months, 12 months and 4 years after withdrawal. TTH, Tension-type headache; CH, combination headache; MH, migraine.
Predictors for relapse
Migraine patients had a significantly lower relapse rate (17 of 54 patients, 32%) compared with patients with TTH (10 of 11 patients, 91%) and CH (seven of 10 patients, 70%, Table 1). Patients overusing triptans had the lowest relapse rate (six of 29 patients, 21%), followed by patients overusing ergots (three of 11 patients, 27%) and analgesics (25 of 35 patients, 71%, Table 2).
Number of patients with relapses 4 years after withdrawal and the type of primary headache, N = 75
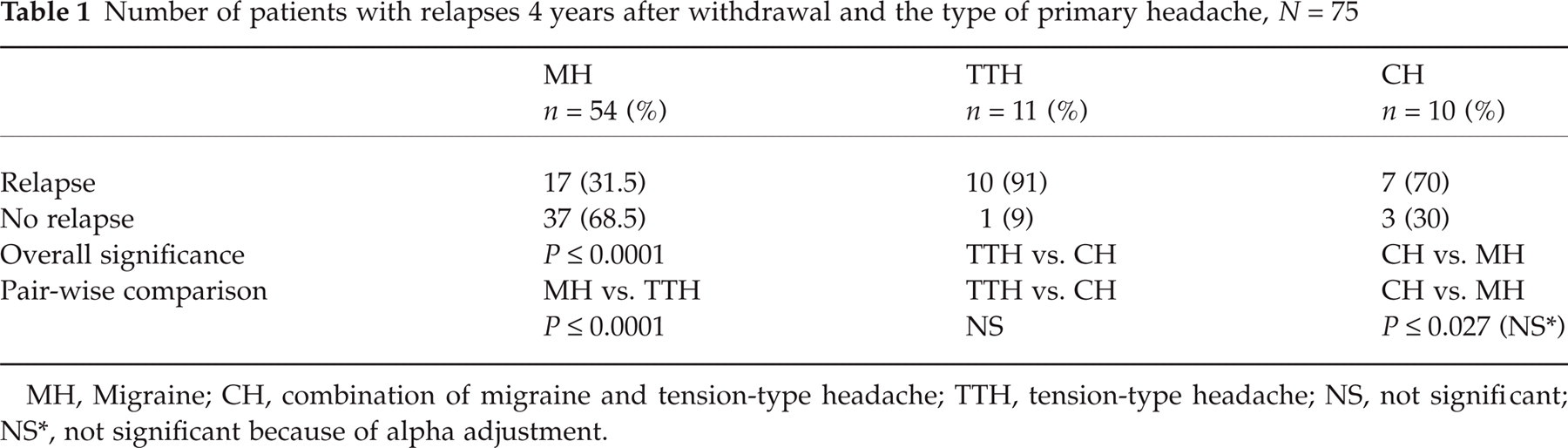
MH, Migraine; CH, combination of migraine and tension-type headache; TTH, tension-type headache; NS, not significant; NS
, not significant because of alpha adjustment.
Number of patients with relapses 1 year after withdrawal and the type of overused medication, N = 75

NS, Not significant.
Since triptans are used by patients with migraine but not by patients with TTH we performed an additional analysis for the subpopulation of patients with MH and CH. The findings were similar to those in the entire patient population. Patients who over-used triptans had the lowest relapse rate (five of 28 patients, 18%), followed by patients overusing ergots (two of nine patients, 22%) and analgesics (17 of 26 patients, 65%).
None of the other investigated variables, such as duration of primary headache, duration of drug overuse and intake vs. no intake of preventive medication, reached significance.
Discussion
The relapse rate 4 years after withdrawal was 45%, which is comparable to previous results (10, 13, 14) and clearly demonstrates the insufficient effectiveness of the current management of patients with MOH. To the best of our knowledge the current study is the first prospective longitudinal investigation on the time course of relapses in a cohort of patients with MOH. An important finding is that the vast majority (94%) of patients relapsed within the first year after withdrawal, clearly indicating that the first year after withdrawal is the most critical phase for relapse. This aspect is of clinical importance since it suggests close follow-up visits and guidance within the first year after withdrawal as a possible therapeutic approach to reduce the likelihood of relapses. This hypothesis, however, has to be challenged in further clinical investigations.
In parallel to the previous 1-year follow-up report of this cohort (9), we found two predictors of relapse: the type of primary headache and the type of overused headache medication. Patients with MH had a lower relapse rate than patients with TTH or CH, confirming previous studies of other groups (4, 10, 11). Another predictor of relapse was the type of overused medication. Patients overusing triptans had a lower relapse rate than patients overusing analgesics. This finding confirms results of a recent retrospective study (13). Previously, higher rates of relapse were found in patients who overused a combination of analgesics with codeine or barbiturates (4, 6, 8, 11). No other predictors of long-term success of withdrawal, such as gender, age, duration of primary headache, duration of drug overuse or intake of preventive medications, were found.
The current study was a sequence of manuscript series describing development and clinical features, withdrawal and rates and predictors of relapse in follow-up observations in patients with MOH, which were published elsewhere (9, 13, 16, 17). Taking all the data together, we were able to demonstrate that all these aspects of MOH are mainly determined by two factors: the type of primary headache and the pharmacological properties of overused headache medication. However, we excluded patients with psychiatric comorbidity, which could be an important predictor of relapse. This issue has to be addressed in further studies.
Finally, the fact that the vast majority of patients relapsed within the first year calls for a more frequent and intensified follow-up programme for patients with MOH during the first year after withdrawal in order to avoid relapse.