
Abstract
The syndrome of orthostatic (low pressure) headaches is well described and most commonly occurs following deliberate violation of the dura (e.g. lumbar puncture). This syndrome can also occur spontaneously and results from the leakage of CSF. We describe three patients who suffered from spontaneous CSF leaks secondary to bony pathology of the cervical spine, and propose that this may be a more common aetiology than originally thought. Often these patients are difficult to manage medically, and surgery may be necessary for symptomatic relief.
Introduction
The syndrome of orthostatic headaches as a consequence of CSF leaks is well recognized (1–3). The CSF leak is referred to as spontaneous when there is no proceeding history of major trauma or deliberate violation of the dura (lumbar puncture, surgical procedures, etc.) (3–7). Spontaneous CSF leaks often occur at the level of the lower cervical or upper thoracic spine, although they can occur at any level of the spine, or rarely at the cribiform plate (4, 5).
Characteristic cranial magnetic resonance imaging (MRI) changes include diffuse pachymeningeal enhancement, subdural fluid collections, cerebellar tonsilar herniation, and other signs of ‘brain sag’ (1). Radioisotope cisternography, spinal MRI, and computed tomography (CT)/myelography with water-soluble contrast dye frequently show abnormalities and may even reveal the site and/or source of the leak (1, 3). Although a combination of a trivial precipitating event (cough, exertion, etc.) in the setting of an underlying weakness of the spinal meninges is generally suspected, a definitive cause is often elusive (1, 3).
To our knowledge there has been only one case in the literature of a cervical bone spur causing a CSF leak resulting in orthostatic headaches (8). We discuss three additional cases, summarizing their clinical presentation, evaluation, treatment and outcome.
Case reports
Patient 1
A 44-year-old registered nurse developed the abrupt onset of a left frontal-parietal headache with associated nausea, left ear fullness, nasal ‘tightness’, paraesthesias involving both hands and feet, and bilateral retro-orbital pressure. She had an ovarian cystectomy under general anaesthesia 1 week previously. The headache was relieved in the supine position and worsened seconds after assuming an upright or inclined position.
Shortly after the onset of her headaches, she had an MRI of the brain and cervical spine (Fig. 1), which revealed abnormal dural enhancement at the level of the foramen magnum and upper cervical spine, with minimally abnormal enhancement of the dura over the convexities. Cerebrospinal fluid analysis was normal with the exception of a low opening pressure. A follow-up CT/myelogram showed a small midline disc herniation at the C5 interspace and corresponding posterior bony spurs superior and inferior to the C5 interspace which indented the thecal sac (Fig. 2). A thin anterior extra-arachnoid fluid collection was also present at the level of the superior margin of C6 just below the inferior spur. This fluid collection continued along the anterior margin of the spinal canal to approximately the level of T11.
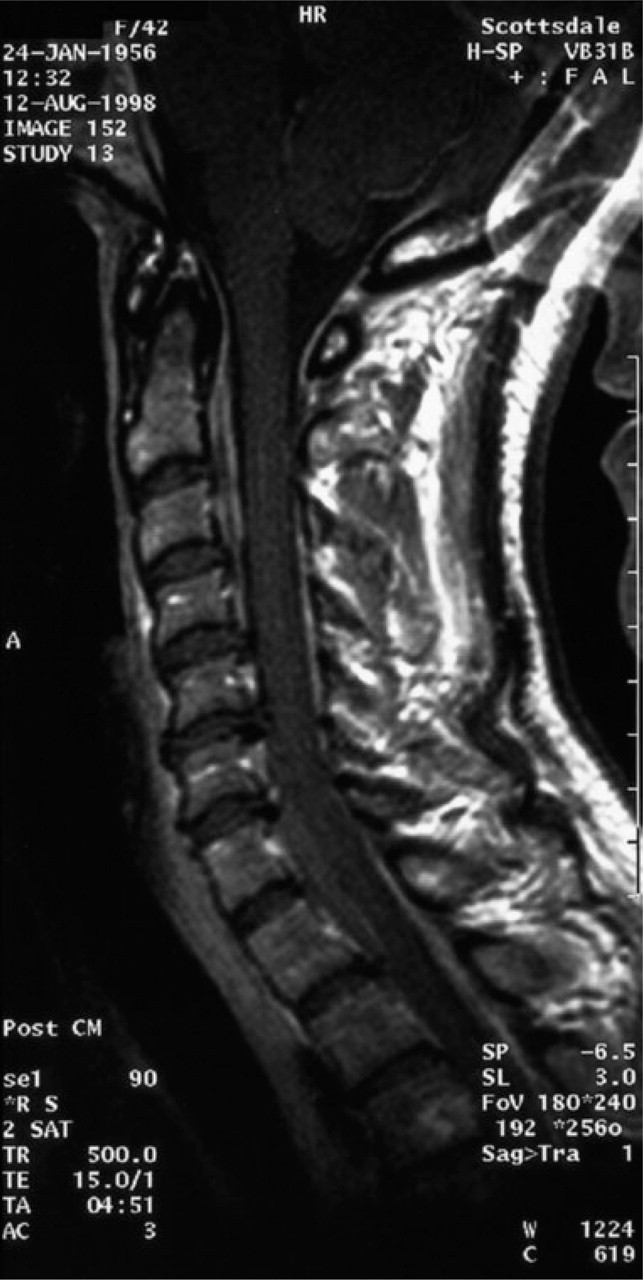
A sagittal gadolinium enhanced T1-weighted image demonstrates abnormally enhancing dura and fluid collections best seen at the C2 and C3 levels anterior to the thecal sac. The disc–osteophyte complex is seen at C5–C6 on this midline image.

An axial computed tomography myelogram at the level of C5–C6 shows an anterior epidural fluid collection and a midline bone spur.
Initial management included a cervical epidural autologous blood patch (6 cm3) which failed to provide relief. Treatment with vigorous i.v. fluid hydration, i.v. caffeine, continuous epidural saline infusion, an infusion of epidural dextran, and oral medications (including opioids and triptans) were also unsuccessful. Finally, after failing to respond to a second cervical epidural blood patch (40 cm3), the patient underwent a C5 discectomy and partial C5/C6 corpectomy. At surgery the bony osteophyte was found to penetrate the dura. In an attempt to expose the margins of the dural tear (which were annealed to the inferior bone spur at C5), the defect enlarged. Numerous other surgeries were performed in an attempt to repair the dural defect, including removal of the spur, C6–C7 corpectomies, and placement of a lumboperitoneal shunt. Twenty-four months after the onset of her symptoms, she continued to be incapacitated with orthostatic headaches. She spent the majority of each day working on a laptop, and remained on long-term disability. The follow-up MRI of the brain and spine revealed no evidence of pachymeningeal enhancement or brain sag, but there was a small anterior extra-arachnoid fluid collection extending from T2 to T4. A small amount of markedly hypointense signal along the dorsal dura was seen at the level of T3 and T4, probably representing haemosiderin. The patient underwent another 20 cm3 lumbar epidural blood patch which provided no relief. A CT myelogram was performed 1 month later which demonstrated a thin extra-arachnoid fluid collection containing contrast material consistent with a CSF leak in the anterior epidural space extending from T3 to T9. There were also a few small focal calcifications in the anterior spinal canal presumably in the anterior longitudinal ligament, the most prominent of which was at the T7–T8 interspace in the midline. This caused prominent indentation of the thecal sac and of the ventral fluid collection. Opening pressure measure at that time was 4.5 cm H2O. The patient underwent placement of a second lumboperitoneal shunt at an outside institution. This was removed 2 months later because it provided no relief of her orthostatic headaches. During her last follow-up visit, 32 months after onset of symptoms, she refused any further surgical intervention and remains disabled with orthostatic headache.
Patient 2
A 39-year-old female with a pertinent past medical history of hypertension and obesity was referred to our clinic with a 6-year history of headache. These headaches began in dramatic fashion one afternoon when she was returning to her office by car after having lunch with some co-workers when she was thunderstruck by an explosive headache. Despite losing control of her vehicle, she did not lose consciousness, nor did she sustain any injury. The headache was associated with neck stiffness, nausea, recurrent vomiting, and exquisite sensitivity to changes in position, particularly rolling, sitting, or standing. The pain was primarily in the left occipital region, but also included the vertex of her head while standing, at which time the pain was unbearable. The severity dramatically decreased upon assuming a recumbent position.
Over the following 6-year period the patient had numerous diagnostic procedures performed, including CTs of the brain, MRIs of the brain and spine, lumbar punctures and a radionucleotide cisternogram. Despite the cisternogram being consistent with a CSF leak (delayed uptake over the hemispheres), all of the neuroimaging studies were read as normal with the exception of mild degenerative changes in the cervical and lumbar spine. The MRI of the brain with gadolinium showed no evidence of dural enhancement, bowing of the optic chiasm, Chiari malformation or other signs of ‘brain sag’. A lumbar puncture (LP) revealed on opening pressure of 5 cm of water and a normal CSF analysis. Because of the abnormal cisternogram and low opening pressure on LP, the patient underwent three separate lumbar autologous blood patches over a year. None of them was effective. She also had three epidural saline infusions which provided her with the best relief, taking the pain down to a manageable 2–4 out of 10. Unfortunately, shortly (10–12 h) after the infusions were removed, the headaches returned to baseline. Other therapeutic attempts including opioids, NSAIDs, triptans, indomethacin, serotonin specific reuptake inhibitors, anti-epileptics, tricyclic anti-depressants, anti-hypertensives, and inhaled oxygen were unsuccessful.
After essentially being restricted to the supine position for years, the patient lost her job, was divorced by her husband and suffered from depression. Interestingly, she had periods marked by gradual improvement in her headache, only to suffer severe setbacks in the form of recurrent thunderclap headaches occurring approximately three to five times each year. After each thunderclap headache she returned to her baseline state of absolute immobility and misery. At the time that we first saw her, she was able to remain upright for 0.5 to 4 h maximum.
A follow-up MRI of the brain at our institution was normal, but a CT myelogram of the spine revealed a contained extra-thecal CSF leak extending from C6 to T2, which retrospectively was present on earlier scans. There was also evidence of mild posterior bony ridging at C3–C4, a small left sided disc herniation at C4–C5, and a prominent posterior bone spur and superimposed disc just to the right of midline at the C7–T1 interspace (Fig. 3). Based on the patient's clinical picture and these findings, an anterior cervical discectomy/osteophytectomy and fusion at the C7–T1 level with an allograph and metal plate was performed. The C7–T1 disc–osteophyte complex was noted to be intimately related to a 3-mm tear in the dura. Primary closure of the dural tear was performed, and a lumbar drain was placed in an effort to ensure closure. Currently, at 1-month follow-up, the patient states that she has experienced a near 50% improvement in her headaches. Most notably, she is able to remain upright for longer periods of time and experiences quicker relief upon assuming a recumbent position. Long-term follow-up will be necessary before determining the overall effectiveness of the surgery.

Axial images from a computed tomography myelogram of the cervical spine show a prominent posterior bone spur and superimposed disc protruding into an epidural fluid collection.
Patient 3
A 46-year-old man with a past medical history of ulcerative colitis and varicose vein surgery presented with a severe, explosive, generalized headache while giving a presentation at a prolonged ‘stand-up’ meeting. The day before he had gone for an uneventful bicycle ride followed by mild posterior neck pain. His headache was associated with right-sided tinnitus and recurrent epistaxis, which occurred each morning for several months. The headache was immediately relieved with recumbancy and provoked by an upright posture. A CT scan of the brain performed the day after the headache started was unremarkable. Despite bed rest, fluid hydration and opioid analgesics, he was bedridden for 2 weeks. He returned to work but the postural headache persisted, and his productivity was reduced over the ensuing 3 months.
A MRI of the brain and C-spine (9 days after headache onset) and a CT/myelography of the entire spine (27 days after headache onset) revealed diffuse prominent pachymeningeal enhancement, an extra-arachnoid subdural fluid collection from C2 to T2 (most prominent at C6–C7), and a disc–osteophyte complex at C4–C5 indenting the thecal sac.
Three months after the onset of the headache, the patient underwent a lumbar epidural blood patch with 18 cm3 of autologous blood. He experienced immediate improvement with complete pain relief in 48 h. However, he developed recurrent neck pain which was posturally exacerbated and when severe, would be accompanied by a headache which was aggravated by shaking his head, flexing his neck, bending, and riding in the car. Follow-up 2 months later showed he was improved, but still requiring propoxyphene for valsalva-induced headache.
A MRI 5 months after the onset of the headache showed an overall decrease in the enhancement of the dura and engorgement of the epidural venous plexus.
There was evidence of a small amount of residual epidural fluid at C2–C5 and C7. The patient, however, declined further treatment.
Discussion
Schaltenbrand, in 1938, described what he referred to as ‘spontaneous aliquorrhea’, a name which has now been replaced by the term spontaneous intracranial hypotension (SIH) (9). Schaltenbrand postulated that SIH was the result of either decreased CSF production, increased CSF absorption, or leakage of CSF through small tears in the dura (9). We now know that SIH results from spontaneous CSF leaks, although the aetiology behind the leak is unclear in many cases (4, 6). These spontaneous leaks are presumed to be secondary to either mild trauma (coughing, sneezing, lifting, etc.) or a pre-existing dural weakness (e.g. meningeal diverticula) (2–4, 6). More recently, dural tears from a spondylotic spur resulting in a CSF leak with low pressure headache have been suggested in the literature (8).
All three of our patients developed abrupt and spontaneous orthostatic headaches without antecedent trauma in the setting of an underlying calcified disc–osteophyte complex indenting the thecal sac in the lower cervical region. The clinical features of these patients were consistent with the syndrome of SIH. Furthermore, in all three cases MRI and CT myelography revealed a CSF leak with prominent extra-axial fluid collections juxtaposed to their underlying bony pathology. All three patients remained refractory to aggressive medical treatment, including autologous blood patches. Two of the three patients underwent surgical repair of the dural tear, which was found to be intimately associated with a posterior osteophyte. One of the patients who underwent surgery has experienced a significant initial improvement with her long-term outcome yet to be determined. Another, despite several surgical attempts to repair the dural defect and placement of a lumboperitoneal shunt on two separate occasions, remains disabled with evidence of a persistent CSF leak in the mid-thoracic region, which radiographically may be related to a separate bony osteophyte at the level of T8–T9. This patient refused any further surgical intervention. The third patient, despite the persistence of symptoms and evidence of CSF leak on MRI, refused surgical exploration after partially responding to an autologous blood patch.
Our experience leads us to make the following conclusions. First, bony pathology of the cervical spine, particularly posterior osteophytes, may lead to dural tears resulting in a CSF leak and the syndrome of SIH with orthostatic headache. Such headaches may present in a sudden and dramatic fashion and must be included in the differential diagnosis of thunderclap headache. Second, because of the prevalence of bony pathology of the cervical spine and the preponderance of CSF leaks in the lower cervical region, this aetiology may be a more common cause of spontaneous CSF leaks than previously recognized. With this in mind, a diligent search for bony pathology should be sought in patients with a CSF leak involving the cervical region. Third, CT/myelography may be necessary to identify the bony abnormality and location of the CSF leak in patients with persistent symptoms despite MRI which may appear unremarkable. Finally, because of the presence of a structural lesion (osteophyte), the dural defect and CSF leak may persist (or be reinitiated), resulting in symptoms refractory to medical management including continuous epidural saline infusion, direct mechanical compression and autologous blood patches (10, 11). In these patients, surgical repair of the underlying dural tear and osteophyte complex may be necessary for symptom relief (12).