
Abstract
Objective
Spontaneous intracranial hypotension is caused by spinal cerebrospinal fluid leakage. Patients with orthostatic headaches and cerebrospinal fluid leakage show a decrease in optic nerve sheath diameter upon movement from supine to upright position. We hypothesized that the decrease in optic nerve sheath diameter upon gravitational challenge would cease after closure of the leak.
Methods
We included 29 patients with spontaneous intracranial hypotension and refractory symptoms admitted from 2013 to 2016. The systematic workup included: Optic nerve sheath diameter sonography, spinal MRI and dynamic myelography with subsequent CT. Microsurgical sealing of the cerebrospinal fluid leak was the aim in all cases.
Results
Of 29 patients with a proven cerebrospinal fluid leak, one declined surgery. A single patient was lost to follow-up. In 27 cases, the cerebrospinal fluid leak was successfully sealed by microsurgery. The width of the optic nerve sheath diameter in supine position increased from 5.08 ± 0.66 mm before to 5.36 ± 0.53 mm after surgery (p = 0.03). Comparing the response of the optic nerve sheath diameter to gravitational challenge, there was a significant change from before (−0.36 ± 0.32 mm) to after surgery (0.00 ± 0.19 mm, p < 0.01). In parallel, spontaneous intracranial hypotension-related symptoms resolved in 26, decreased in one and persisted in a single patient despite recovery of gait.
Conclusions
The sonographic assessment of the optic nerve sheath diameter with gravitational challenge can distinguish open from closed spinal cerebrospinal fluid fistulas in spontaneous intracranial hypotension patients. A response to the gravitational challenge, that is, no more collapse of the optic nerve sheath while standing up, can be seen after successful treatment and correlates with the resolution of clinical symptoms. Sonography of the optic nerve sheath diameter may be utilized for non-invasive follow-up in spontaneous intracranial hypotension.
Keywords
Introduction
Spontaneous intracranial hypotension (SIH) is an increasingly recognized disease characterized by orthostatic headache (OH). Pathophysiological concepts describe leakage of cerebrospinal fluid (CSF) through a spinal dural fistula (1–4).
High-resolution transorbital sonography of the optic nerve sheath diameter (ONSD) is increasingly used for the assessment of SIH as well as in patients with increased intracranial pressure. In patients with OH, transorbital sonography is able to discriminate between patients with SIH and those without SIH (5,6). A collapse of the optic nerve sheath (ONS) when moving from the supine to the upright body position (gravitational challenge) in SIH patients has been demonstrated in parallel to the evolvement of clinical symptoms (5). However, the literature on ultrasound diagnostics in patients with SIH is still sparse and consists only of a case study and an investigation in 10 patients on the effect of epidural blood patch on ONSD and ophthalmic venous flow, respectively (7–9). Sonography is a simple, cost-effective, non-invasive tool for use during diagnosis and follow-up after conservative or surgical treatment and may contribute to a better understanding of the pathophysiology of SIH.
Based on pathophysiological considerations and our previous results, we hypothesized that the decrease in ONSD upon the aforementioned gravitational challenge seen in patients with an open leak should cease after closure of the leak (Figure 1). We evaluated ONSD by performing two high-resolution orbital ultrasound assessments in the supine and upright positions, in a longitudinal study of patients with SIH, before and after successful microsurgical closure of the dural fistula.
Patient with spontaneous intracranial hypotension, orthostatic headaches and open CSF leakage show a significant collapse of the optic nerve sheath diameter when changing from supine (1) to upright (2) position (“gravitational challenge”). We hypothesize that the decrease in ONSD upon the gravitational challenge should cease after closure of the leak.
Methods
Patient characteristics
This is a retrospective analysis of a non-controlled consecutive cohort. The study cohort included all patients with confirmed SIH and intractable symptoms refractory to conservative treatment admitted between January 2013 and December 2016. All patients had a proven spinal CSF leak. Microsurgical sealing of the CSF leak was aimed at in all cases.
In every patient, diagnosis of SIH was made according to the criteria of the International Headache Society (10). These criteria are:
(A) Any headache fulfilling criterion C; (B) Either or both of the following:
low CSF pressure (<60 mm CSF); 2. Evidence of CSF leakage on imaging (brain imaging showing brain sagging or pachymeningeal enhancement, or spine imaging (spine MRI, or MRI, CT or digital subtraction myelography) showing extradural CSF; (C) Headache has developed in temporal relation to the low CSF pressure or CSF leakage, or has led to its discovery; (D) not better accounted for by another International Classification of Headache Disorders 3rd edition (ICHD-3) diagnosis.
All patients with confirmed SIH showed evidence of CSF leakage on imaging as required by criterion (B) above (10).
Diagnostic protocol in patients with SIH
Routine workup comprised a systematic stepwise diagnostic protocol with sonography of the ONS, first in the supine and secondly in the upright body position; spinal thin-sliced magnetic resonance imaging (MRI) with and without intrathecal contrast, dynamic myelography and post-myelography computed tomography (CT) (5,11).
The MRIs were performed on a 1.5 T Magnetom Aera Siemens scanner (Siemens, Erlangen, Germany). The protocol included an MRI of the entire spine without contrast including sagittal T1WI and T2WI, and isotropic 3D T2W turbo spin echo (SE) sequence with fat saturation. After intrathecal contrast injection, an isotropic 3D T1W gradient echo (gre) sequence with fat saturation was performed.
CT images were acquired using a 128-slice multi-detector-row CT scanner (SOMATOM Definition Edge, Siemens, Erlangen, Germany) with 0.5-second gantry rotation time, 180 × 180 mm field of view, 128 × 0.6 mm collimation, pitch 0.8 in head-first position. Automatic exposure control (CARE Dose 4D, care kV, Siemens Healthcare) was switched on, so the radiation output was automatically adjusted according to the patient's size.
The lumbar opening pressure was measured before intrathecal application of 0.5 ml of a gadolinium based contrast agent (Gadopentetate dimeglumine (Gd-DTPA2) in a dose of 0.25 mmol by 0.5 ml) in supine position. In accordance with our clinical protocol, gadolinium was administered intrathecally 1–2 hours prior to the MRI. The exact anatomical site of the leak was identified according to a stepwise protocol (12). The diagnostic protocol is stopped if patients respond successfully to conservative treatment. Conservative treatment included epidural blood patch with infusion of 20–40 ml autologous blood into the L3–L4 level. If conservative treatment failed and the exact site of the CSF leak was identified, microsurgical exploration was performed. Thus, the study population included all patients with confirmed SIH and intractable symptoms refractory to conservative treatment, including epidural blood patch.
The choice of postoperative imaging depended on the patients’ clinical course. Although transorbital sonography was performed in every patient, spinal or cranial MRI was not routinely done in every patient.
Microsurgery for SIH
Intraoperatively, the cause of SIH was identified in all patients as a longitudinal dural slit. Discogenic microspurs were removed and the dural slits were sutured (Figure 2). The nature of the CSF leak and the underlying causative microspurs has been described previously (11).
(a) Schematic artist drawing of the intraoperative view angle to the dura perforating disc spur. The red dot represents the disc spur. The red shaded area is the view angle of the surgeon under the operating microscope. (b) Intraoperative view, identical to the schematic artist drawing with a red dot marking the disc spur.
Assessment of the ONSD
All SIH patients received a preoperative ultrasound scan within 2 weeks prior to surgery. Postoperative transorbital ultrasound was done 27.1 ± 30.7 days (mean ± SD; range 2–104 days) after surgery in all patients. The postoperative ultrasound examination took place either during the hospital stay or at the outpatient center. The timing was also dependent on the clinical course of the patients’ illness (i.e. first done if fully mobilized and free of OH). One patient, although no longer bedridden, complained of persistent OH after surgery and one patient was lost to follow-up. In all other patients, symptoms of SIH had resolved (n = 26) or were ameliorated (n = 1) at the time of the follow-up examination. The ONSD was performed using a 7–15 Mhz linear array transducer attached to a color-Duplex machine (IU22, Philips, Amsterdam, Netherlands). The transducer was placed on the upper eyelid with a layer of gel. ONSD is measured on each eye. First, the examination is done in the supine position. Directly after the measurements in the the supine position, transorbital sonography is done in the upright position while the patient stands upright for 2 minutes (Figure 3).
(a) Schematic drawing of the optic nerve sheath diameter (ONSD) measurement in the supine and upright position. (b) An ultrasound image of the ONSD measurement obtained in the typical manner. + : distance behind the papilla; x: ONSD.
ONSD was measured 3 mm behind the echogenic lamina cribrosa in the axial planes. A perpendicular axis was used (5,9). The ONSD was calculated as the mean of six values (three measurements on each eye). All examinations were made by an examiner trained in ONS ultrasound diagnostics.
Ultrasound safety and ethical considerations
In accordance with the guidelines of the British Medical Ultrasound Society and the US Federal Drug Administration, the mechanical index was reduced to less than or equal to 0.23. The analysis was conducted in accordance with good clinical practice guidelines, the Swiss Academy of Medical Sciences and the Declaration of Helsinki. The study was approved by the local ethics board.
Outcome measures and statistical analysis
For the primary analysis, we compared the changes of the ONS before and after microsurgical closure of the CSF fistula. We also recorded changes in the ONSD when moving from the supine to the upright position (“gravitational challenge”) in patients before and after surgery. Values are described as mean ± standard deviation (mm).
Between the two groups, analysis was performed using the Wilcoxon rank sum test. All statistical tests were two-sided with a 5% significance level. Patients' database was based on REDCap Software, version 5.9.0 (© 2014 Vanderbilt University, Nashville, TN). Statistics were generated with SPSS (© 2017 IBM Corporation, Armonk, NY). Graphs were drawn with GraphPad Prism 7.03 (© 1992–2017 GraphPad Software, Inc., La Jolla, CA).
Results
Between January 2013 and December 2016, 29 patients with refractory clinical symptoms of SIH were proven to have a CSF leak by extrathecal contrast accumulation after intrathecal contrast application. Of these, two patients were excluded. One patient declined surgery and one was lost to follow-up. The final analysis comprised 27 patients (19 women, eight men; mean age 45 (range 26–70) years). Before surgery, all patients suffered from refractory orthostatic symptoms and had been diagnosed with SIH according to the criteria of the International Headache Society with a direct proof of a CSF leakage obtained from imaging.
Patient characteristics. * Two patients were excluded. One patient declined surgery and one was lost to follow-up.
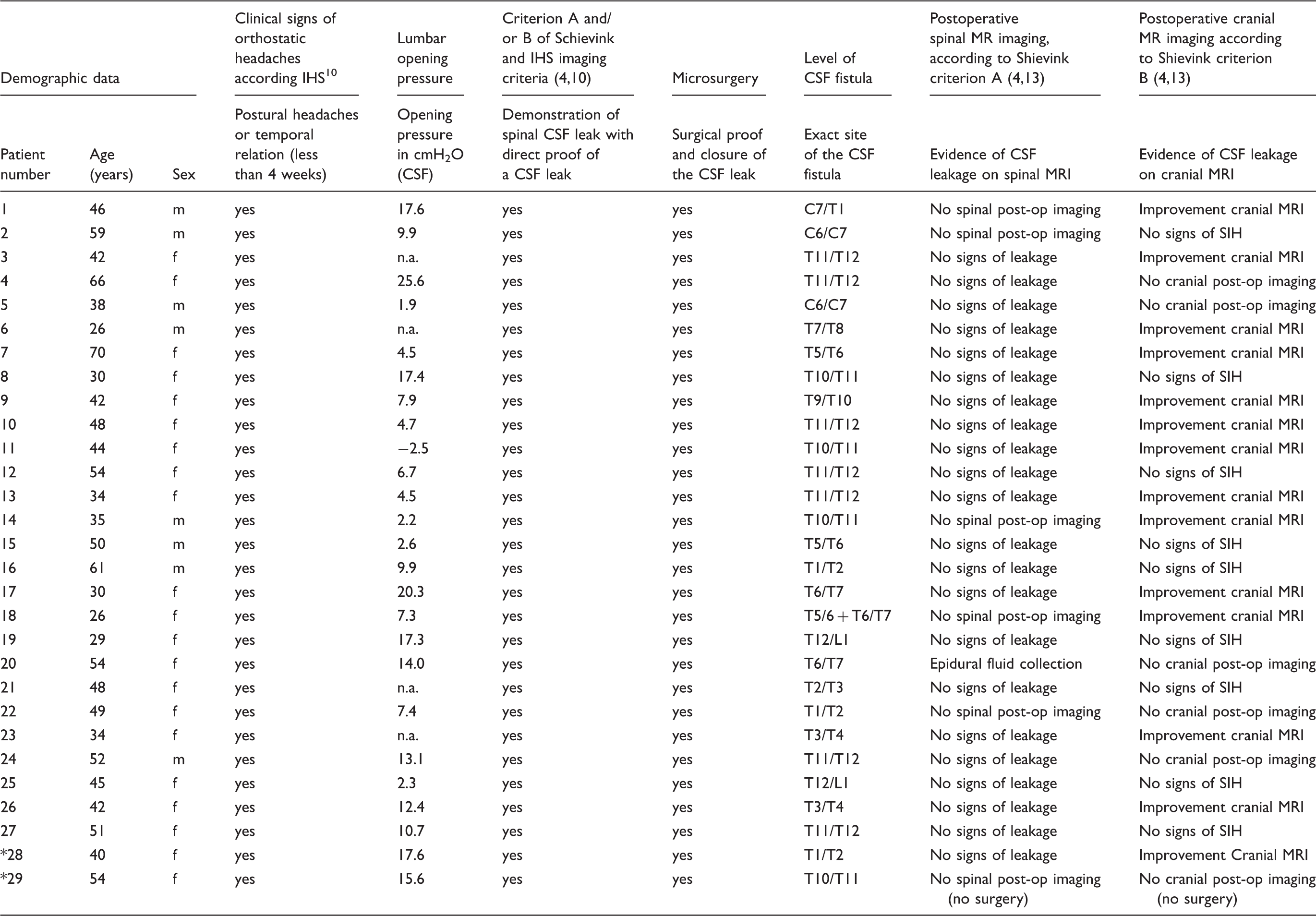
In all but 4 patients (data were missing) the lumbar opening pressure was 9.5 ± 6.9 (cmH2O/CSF). Of the 27 patients included in the analysis, only 8/27 (29.6%) patients had a lumbar opening pressure of less than 6cmH2O (Table 1).
Ultrasound of the ONSD before microsurgical closure of the CSF fistula
A significant decrease (collapse) of 7% in the ONSD could be demonstrated in patients with an open CSF fistula when moving from a supine to an upright position before surgical treatment. Transorbital ultrasound showed a mean diameter of 5.08 ± 0.66 mm in the supine position. Upon gravitational challenge, ONSD decreased to a mean of 4.73 ± 0.69 mm. The difference in the ONSD with gravitational challenge was statistically significant (p < 0.01; Wilcoxon rank sum test) with a mean Δ-ONSD of −0.36 ± 0.32 mm.
Ultrasound of the ONSD after microsurgical closure of the CSF fistula
Transorbital ultrasound after microsurgical closure of the CSF fistula showed a mean diameter of 5.36 ± 0.53 mm in the supine position. Upon gravitational challenge, the ONSD showed the same mean diameter of 5.36 ± 0.65 mm in the upright position. There was no statistically significant difference between the supine and upright positions (p = 0.98; Wilcoxon rank sum test) with a mean Δ-ONSD of 0.00 ± 0.22 mm.
Comparison of the ONSD before and after microsurgical closure of the CSF fistula
Comparing the mean diameter of the ONSD measured in the supine position alone, there was a significant increase of 5.5% from the pre- to the postoperative ONSD after microsurgical closure of the CSF leak (5.08 ± 0.66 mm before surgery versus 5.36 ± 0.53 mm after surgery, p = 0.03; Wilcoxon rank sum test, Figure 4(a)).
(a) Bee swarm data with means and standard deviations (SDs) showing differences between the same patients in supine and upright position before (green dots) and after (red dots) successful closure of a cerebrospinal fluid fistula. (*) shows the data of a healthy control group, recently published (5); (b) shows the difference between the supine and the upright position (Δ-ONSD) in the gravitational challenge. Two patients on graph 4(b) are highlighted (yellow) because they showed an increase of the Δ-ONSD after surgical treatment.
The Δ-ONSD during gravitational challenge before surgery (−0.36 ± 0.32 mm; −7.0%) was statistically significantly different to the Δ-ONSD after microsurgical closure of the CSF fistula (0.00 ± 0.22 mm; 0.0%) (p < 0.01; Wilcoxon rank sum test; Figure 4(b)). Two patients did not respond to the treatment as expected. In these patients, the decrease in ONSD upon gravitational challenge did not cease after closure of the CSF leak. In contrast to the other patients, the Δ-ONSD upon gravitational challenge increased after treatment. We highlighted these two patients in Figure 4(b).
Comparison of the ONSD before and after microsurgical closure of the CSF fistula
The results in the Δ-ONSD after microsurgical closure of spinal CSF fistula in our current patient series, show no statistically-significant difference from that of a recently published control group of 39 subjects without any symptoms of SIH (0.00 ± 0.22 mm vs. 0.01 ± 0.38 mm, p = 0.58; Wilcoxon rank sum test; Figure 4(b)) (5).
Discussion
The ONSD is related to the intracranial pressure (5,14–18). Hansen et al. demonstrated an immediate response of the ONS after a lumbar infusion test. This is in line with previously published results, showing that the reduced CSF volume led to a reduced intracranial pressure in symptomatic patients (15,16,19).
We showed that a proven, open dural leak is associated with the collapse of the ONS. Microsurgical suturing of the spinal CSF leak not only led to an increased ONSD but also ameliorated the collapse of the ONS, thus corroborating a causal relationship between a high-flow spinal CSF fistula and the ONSD. These findings correlate with the resolution of clinical symptoms.
Relationship of the Δ-ONSD with dynamic aspects of SIH in patients with an open CSF fistula
Many patients with SIH are asymptomatic or oligosymptomatic while lying in the supine position but exhibit symptoms when in the upright position. As previously described in patients with SIH and OH, a significant decrease (collapse) of 10.0% in the ONSD upon gravitational challenge could be demonstrated (5).
The current analysis corroborates the link between an open leak and concurrent symptoms together with CSF changes in the intracranial compartment, and symptoms that are reversed in the same patients once the system is closed, as reflected by a “normalized” reaction to gravitational challenge. These findings are supported by the comparison of the Δ-ONSD in successfully treated patients in our current analysis with results in recently published control group (Figure 4(b)) (5).
From the pathophysiological point of view, these results support the thesis of a reduced intracranial pressure with an increased craniospinal compliance (16,19,20).
Two patients (highlighted in Figure 4(b)) showed an “inverse” response of the ONS after closure of the spinal CSF leak. Even though the CSF leak had been closed, the Δ-ONSD upon gravitational challenge increased after treatment. Despite the low number of patients concerned (n = 2), these findings are very interesting. We hypothesize that the CSF leak was not completely closed. Another possibility could be the occurrence of further CSF leakage. This further CSF leakage could be concealed in preoperative spinal imaging. To reveal whether there was further CSF leakage, we have reviewed the postoperative imaging for these patients. Both patients underwent spinal thin sliced MRI after surgery, but this revealed no evidence of CSF leakage. In parallel, SIH-related symptoms resolved in these two patients. Thus, the reason for the observed increase in postoperative Δ-ONSD remains speculative.
The patients studied in our current series, all suffered from OH and had a spinal CSF leak with an outflow of CSF that was sufficient to trigger an immediate change in the intracranial CSF compartment and, most likely, to intracranial pressure in the upright body position. This association is not trivial, given the many patients with blunted symptoms, “inverse” symptoms, or with symptoms that only evolve over the course of the day after several hours of being upright. Future studies should be performed to evaluate whether the current patient group, with refractory SIH and treated surgically, constitutes only a specific subgroup of all patients with SIH.
Comparison with published studies on optic nerve sheath diameter
Comparison of ONSD in literature patients with non-elevated ICP.

The two associated parameters of the ONSD in the gravitational challenge reflect an independent parameter of low intracranial pressure with an increased compliance of the CSF system.
Diagnosis of SIH
Patients with SIH are often difficult to diagnose and treat. All patients in our current series fulfilled the criteria for SIH set by the International Headache Society (26). Defining a stepwise protocol with a meticulous workup and a classification system (12) helped to gain more insight, especially in patients with long-standing symptoms.
Despite useful imaging criteria (i.e. presence of extrathecal contrast in the spinal MRI or cranial imaging with presence of subdural fluid collections, a sagging of the brain or enhancement of the pachymeninges), cranial and spinal MRI of some patients may reveal only minor changes, and diagnosis remains challenging (4). Other diagnostic criteria, notably the lumbar opening pressure (measured as a single value in lumbar puncture) are not as reliable and would not suffice as the sole parameter for diagnosis of SIH (19). In a recently published study, we have found in eight of 14 patients (57.1%) a higher cutoff than the suggested (<60 mmH2O; 4.4 mmHg) (19). Only 30% of all patients in the present analysis showed a lumbar opening pressure of less than 60 mmH2O, as stipulated by IHS criteria (10). Thus, the sensitivity/specificity of the lumbar opening pressure is rather low.
Study limitations
Limitations of this study are that the ONSD can be user- and machine dependent, with a range of non-pathological values in literature. Moreover, this was a single-centre study with a small number of patients, and the findings need to be verified by a larger prospective trial.
Conclusion
Transorbital sonography of the ONS during gravitational challenge offers a diagnostic tool to differentiate between an open and a closed spinal dural CSF leak. After treatment of SIH, it can be useful during follow-up. The findings correlate with the clinical resolution of symptoms and give insights into the pathophysiology of CSF dynamics.
Footnotes
Clinical implications
Transorbital ultrasound of the optic nerve sheath diameter shows a significant decrease (collapse) when moving from the supine to the upright position (“gravitational challenge”) in patients with an open spinal CSF fistula. After successful microsurgical closure of the spinal CSF fistula, this difference ceases and ONSD remains stable. In addition, the diameter of the optic nerve sheath measured in the supine position alone increased after successful treatment. Transorbital ultrasound of the optic nerve sheath diameter may be utilized for the follow up in the treatment of patients with SIH and intractable orthostatic headaches.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.