
Abstract
We applied the recent International Headache Society (IHS) criteria for headache related to spontaneous intracranial hypotension (SIH) to 90 consecutive patients with a final diagnosis of SIH confirmed by cerebral magnetic resonance imaging with contrast. Orthostatic headache (developing within 2 h of standing or sitting up) was present in 67 patients (75%) but appeared within 15 min after standing or sitting—as required by point A of the criteria—in only 53 (59%). Forty-four (49%) patients did not satisfy point A, including 22 (24%) with non-orthostatic headache and 14 (16%) with headache developing ≥ 15 min after standing or sitting up; 80 (89%) did not satisfy point D. Only three (3%) patients had headache fully satisfying the IHS criteria. These findings indicate that the current IHS criteria do not capture most patients with SIH-associated headache. Excluding the requirement for response to epidural blood patch (criterion D) and considering headaches appearing within 2 h of sitting or standing up would capture more patients.
Keywords
Introduction
Spontaneous intracranial hypotension (SIH) has generated increasing interest over the last 15 years (1). Clinical experience and literature data indicate that orthostatic headache is the prototypic manifestation of SIH, while typical magnetic resonance imaging (MRI) findings, as proposed by Schievink (1), are: (i) subdural fluid accumulation; (ii) pachymeningeal enhancement; (iii) venous engorgement; (iv) pituitary hyperaemia; and (v) sagging of the brain (1–5). Point 4, pituitary hyperaemia, should, however, be considered as part of point 3, i.e. a local, peculiar manifestation of venous engorgement. Recent evidence suggests that SIH, once considered a very rare disorder, may have been frequently underdiagnosed or misdiagnosed in the past (6). Migraine and tension-type headache are among the most common misdiagnoses (6). A recent emergency department study estimated that SIH has an annual incidence of five per 100 000 and indicated it was an important cause of new daily persistent headaches, particularly in the young and middle-aged (1).
The International Headache Society (IHS) recently proposed diagnostic criteria for headache attributed to SIH (7) (Table 1). However, these criteria have not been tested in large series with SIH. In this study, the IHS diagnostic criteria for headache attributed to SIH were assessed in a large series of SIH patients.
International Headache Society criteria for headache attributed to spontaneous intracranial hypotension (IHS-2004: 7.2.3/ICHD-II, 2004)

CSF, cerebrospinal fluid; MRI, magnetic resonance imaging; CT, computed tomography.
Patients and methods
Ninety patients presenting consecutively at our Institute between 1993 and 2006 with a final diagnosis of SIH confirmed by cerebral MRI with contrast (Table 2) (8) were included. Thirty-five were male (39%) and 55 female (61%); mean age at first examination was 45 years (range 15–71). Median follow-up was 3 years (range 8 months to 14 years). Median time from symptom onset to diagnosis was 4 months (range 15 days to 45 months). Headache and other clinical characteristics were recorded in a semistructured interview. Seventy (78%) patients received their headache interview at initial admission. In the remaining 20 patients (22%), the interview was completed later by telephone. The IHS (2004) (7) criteria for headache attributed to SIH (Table 1) were applied.
Cerebral MRI findings in 90 SIH patients
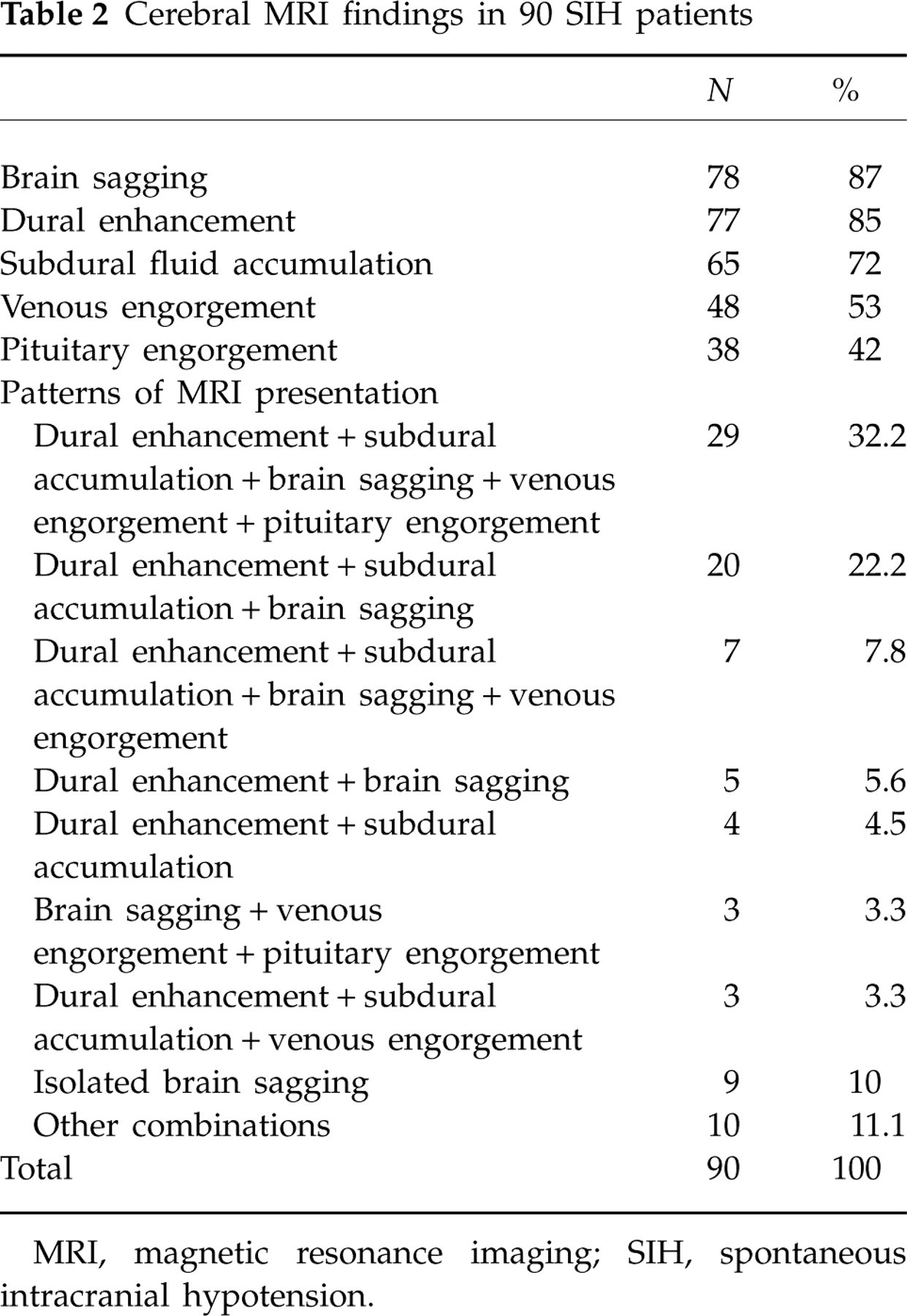
MRI, magnetic resonance imaging; SIH, spontaneous intracranial hypotension.
Headache was considered improved when frequency or intensity were reduced ≥ 50% and patients returned to daily activities.
The MRI studies were considered to confirm the SIH diagnosis when the ‘typical’ findings described by Schievink (1) were present (Table 2). The neuroradiologists were not blinded to the clinical presentation. In the search for cerebrospinal fluid leakage (CSF), additional imaging studies were performed: MRI of the spine with or without myelographic effect (n = 64), myelo-computed tomography (n = 23), and radionuclide myelocisternography (n = 26).
Clinical history and evolution, imaging studies and results of treatments all contributed to the final diagnosis of SIH and excluded other diagnoses, such as meningitis or dural sinus thrombosis, that were sometimes initially entertained.
Two patients with symptoms compatible with SIH and with normal MRI were lost to follow-up and therefore excluded from the study.
Patients were treated for SIH with bed rest, oral hydration and steroids (1–4). If there was no improvement after a month, epidural blood patch (EBP) was given (9–11).
Results
No differences in clinical or general characteristics were found between patients interviewed on admission (N = 70) and those (N = 20) whose interview was completed later by telephone (data not shown). All patients satisfied points B and C of the IHS diagnostic criteria for headache attributed to SIH. Specifically, all patients had typical neuroimaging signs of SIH (1), which appeared in different combinations (Table 2). The only finding that although isolated was considered sufficient to diagnose SIH was brain sagging (12).
No patient had a history of dural puncture or CSF fistula (7).
Headache characteristics and associated phenomena pertinent to the IHS classification are shown in Table 3. Orthostatic headache was present in 67 (75%), but only in 53 (59%) of these did it appear within 15 min of standing; the headache was non-orthostatic in 22 (24%). Thus, 44 (49%) patients did not satisfy point A of the IHS criteria (8), either because their headache was not orthostatic (24%) or because their orthostatic headache began > 15 min (but within 2 h) of sitting or standing (16%) (Table 4 and Fig. 1). EBP was administered to 28 (32%) patients. A marked reduction in headache occurred in all of these, but only in 10 (11%) did the improvement occur within 72 h (Table 5). Eighty (89%) patients did not satisfy point D of the criteria (Table 5 and Fig. 1) (7); of these, 37 did not satisfy point A as well (Fig. 1). Only three (3%) patients had a headache satisfying the IHS criteria for headache attributed to SIH (Fig. 1).
Clinical manifestations and headache characteristics in 90 patients with spontaneous intracranial hypotension
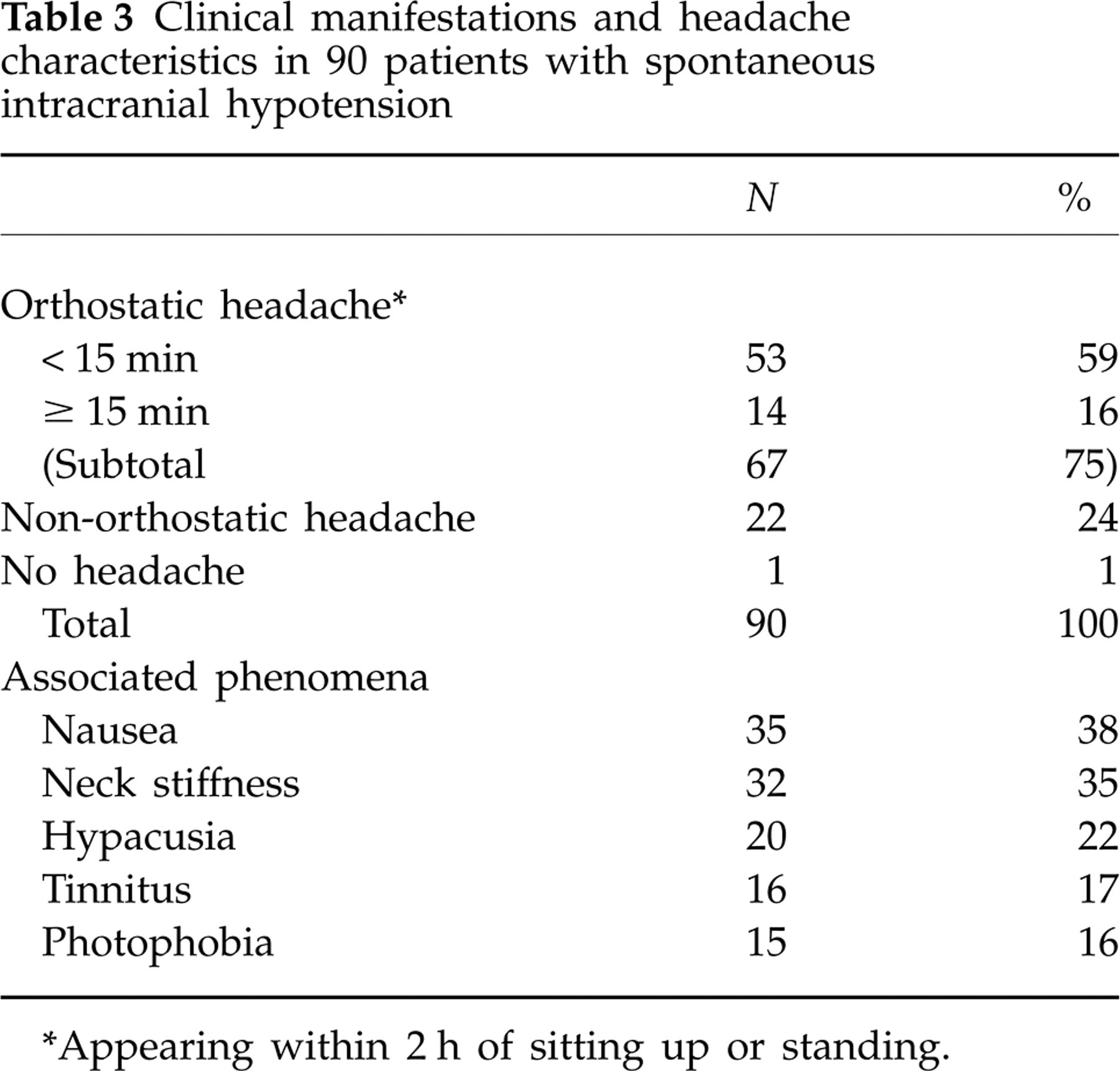
∗Appearing within 2 h of sitting up or standing.
Adherence to criterion A of International Headache Society criteria for headache attributed to SIH in 90 patients with SIH

All patients met criteria B and C (see Results section).
SIH, spontaneous intracranial hypotension.
Adherence to criterion D of International Headache Society criteria for headache attributed to SIH in 90 patients with SIH
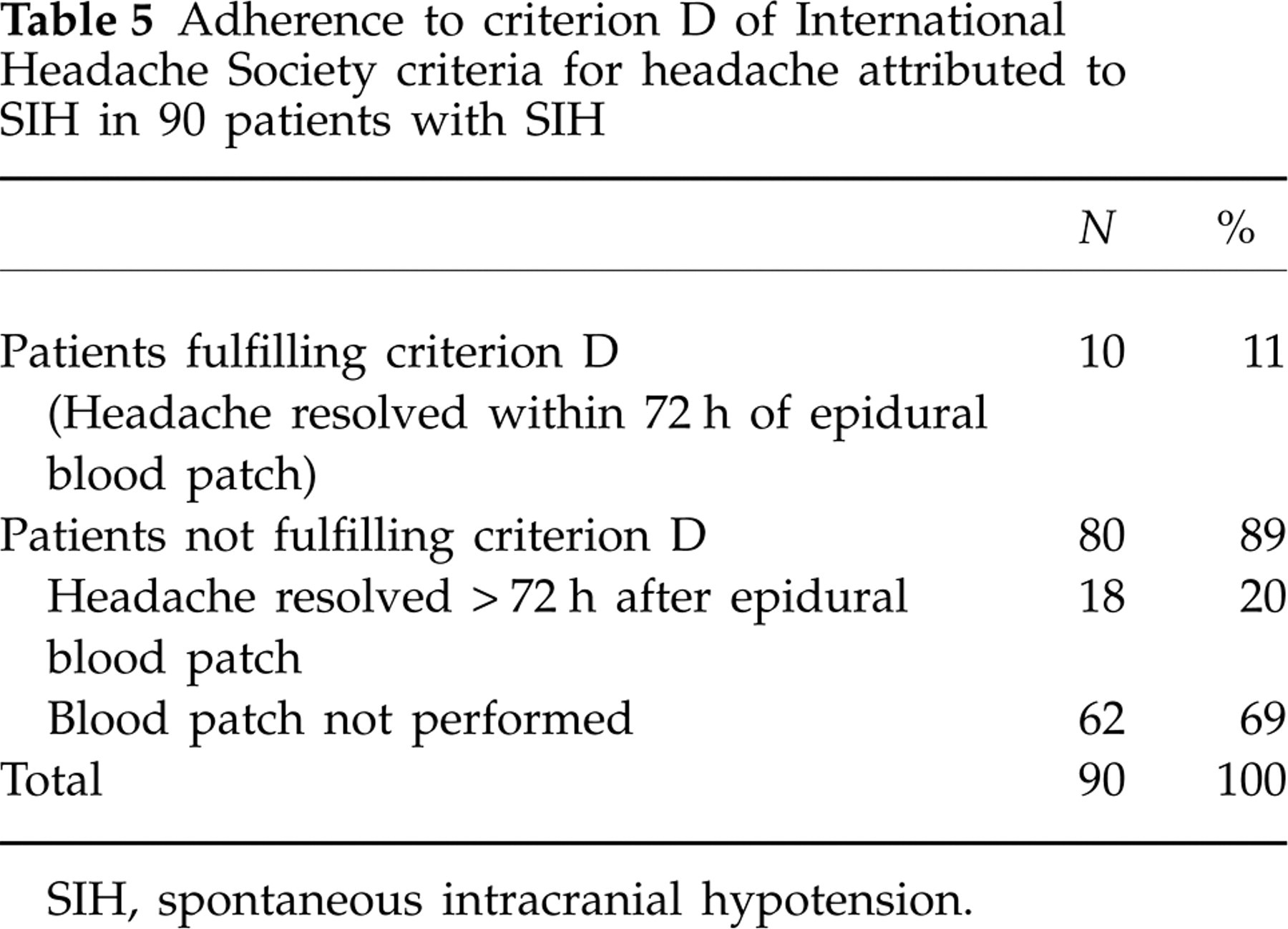
SIH, spontaneous intracranial hypotension.
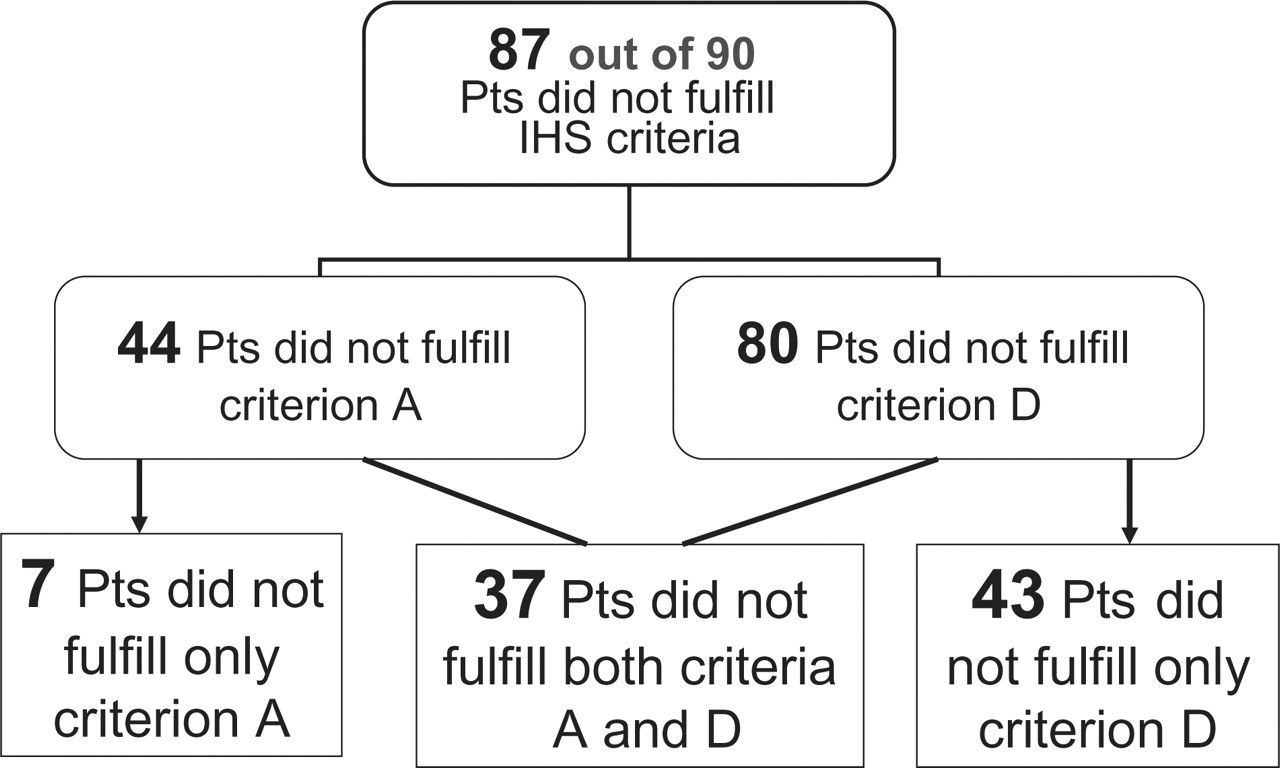
Application of the International Headache Society criteria for headache attributed to spontaneous intracranial hypotension (SIH) in 90 consecutive patients diagnosed with SIH. Only three patients fulfilled criteria for headache attributed to SIH. Note that 62 of the 80 patients not fulfilling criterion D did so simply because they did not receive epidural blood patch to treat the condition.
Discussion
This appears to be the first study to apply the IHS criteria for SIH-associated headache systematically to a large series of patients with a MRI-confirmed SIH. The criteria proved unable to diagnose SIH-associated headache in the overwhelming majority (97%) of cases. One possible reason for this surprising result could be that the population studied was unrepresentative: our patients were seen at a tertiary referral centre, and a more representative population would be one presenting at an emergency room (9, 13). Most of our patients (78%) received their headache interview at initial admission (5). In the remainder, the interview was completed later by telephone. We found no differences between these two groups of patients.
In our series, no patients had normal brain MRI findings. Certainly such patients exist and have occasionally been reported (1). However, the fact that in our series all the patients had abnormal MRI findings reinforces, rather than limiting, the value of our data by excluding possible clinical misdiagnoses not supported by imaging studies.
Apart from the possible sample and recall biases, it is clear that an important reason for the very low proportion diagnosed with SIH-associated headache in our series was that EBP was not performed in most cases: 62 (69%) patients did not satisfy point D of the criteria simply because they did not receive EBP, because the headache improved or was not debilitating enough to require the procedure. It is impossible to establish how many of these 62 patients, who were not treated with EBP, would have responded to the procedure. Similarly, in the study of Kong et al. (14), only five (38%) of 13 patients received EBP, and not all benefited from the procedure. Furthermore, although all of the 28 (31%) patients in our series who received EBP had headache improvement, only 10 (11%) improved within 72 h, and hence only these 10 fulfilled point D (Table 5).
We are aware of no controlled studies that demonstrate the benefit of EBP in SIH (9–13). Such studies would anyway be rendered difficult by the fact that SIH resolves spontaneously in the majority of cases (1, 2). It seems reasonable to propose, therefore, that EBP should be given when patients do not improve after at least a month of commonly reported conservative treatment (bed rest, oral hydration, caffeine, theofillin and steroids) (1, 2, 4, 14) or when the headache or other symptoms are highly disabling—the policy at our centre. However, no controlled studies demonstrating the efficacy of these conservative treatments, particularly steroids, are available. In the light of these considerations we propose that a response to EBP should not be necessary in order to diagnose SIH-associated headache.
According to the IHS criteria, fulfilment of point A requires fulfilment of point D (Table 1). In our study we did not consider fulfilment of point D necessary for fulfilment of point A. Nevertheless, point A (plus points B and C of the IHS classification) was satisfied in only 51% of our patients. One reason for this was that nearly a quarter had non-orthostatic headache (Table 4). The other main reasons were orthostatic headache developing ≥ 15 min after sitting or standing (16%) and orthostatic headache developing within 15 min but without associated phenomena (8%). If the time limit were changed to 2 h, 61% would satisfy point A (plus points B and C of the IHS classification) (Table 6). Furthermore, if the time limit were changed to 2 h after sitting or standing, and the presence of associated phenomena were no longer required, 75% of patients would satisfy criterion A (Table 6).
Proposal of modification of current International Headache Society criteria for diagnosis of headache attributed to SIH

SIH, spontaneous intracranial hypotension; CSF, cerebrospinal fluid.
Until the role of EBP is clarified by appropriate clinical studies, we propose that point D be removed from the diagnostic criteria, and specifically that EBP response should no longer be necessary for the diagnosis of headache attributed to SIH. Two other possible suggestions for revision are illustrated in Table 6. The first is that, for criterion A, the headache should appear within 2 h of sitting or standing and should be associated with at least one of the associated phenomena. If this were adopted, 61% of our SIH patients would have had SIH-associated headache. The second possibility is that orthostatic headache should appear within 2 h of sitting or standing but need not be associated with any of the listed phenomena. In this case, 75% of our SIH patients would satisfy criterion A (again plus points B and C of the IHS classification) (Table 6).
In patients with non-orthostatic headache or with headache beginning > 2 h after sitting or standing, headache improvement after EBP should be considered a useful adjunctive diagnostic criterion of SIH-associated headache (Table 6, proposal 3). We believe these proposals represent a useful and constructive basis for future studies on diagnostic criteria for SIH-associated headache in a large cohort of patients diagnosed with SIH in various clinical contexts, in order to avoid the possible selection and recall biases of the present study.