
Abstract
Background
Matters of workplace harassment are an important issue. This issue needs to be recognized and studied to prevent occurrences. These important sensitive areas of effective workplace management are increasingly gaining more interest. We aimed to identify the prevalence of workplace sexual, verbal and physical harassment among headache professionals.
Methods
We adopted a cross‑sectional exploratory survey approach with quantitative design. The survey was distributed electronically among headache healthcare and research professionals globally through the International Headache Society (IHS).
Results
Data were obtained from 579 respondents (55.3%; 320/579 women). A large percentage of respondents (46.6%; 270/579) had experienced harassment; specifically, 16.1% (93/578) reported sexual harassment, 40.4% (234/579) verbal harassment and 5.5% (32/579) physical harassment. Women were almost seven times more likely to experience sexual harassment compared to men (odds ratio = 6.8; 95% confidence interval = 3.5–13.2). Although women did also more frequently report other types of harassment, this was not statistically significant (odds ratio = 1.4; 95% confidence interval = 1.0–2.0).
Conclusions
Lifetime exposure to workplace harassment is prevalent among headache professionals, especially in women. The present study uncovers a widespread issue and calls for strategies to be implemented for building a healthy and safe workplace environment.
Introduction
Although not always recognized, healthcare as an industry is predisposed to harassment (1–4). In some cases, this may be related to differences in economic status, prestige and power (5–7). Not only can this problematic behavior affect victims severely (8,9), but it may influence patient outcomes. A consistently positive association has indeed been found between a positive workplace environment and positive patient outcome across multiple studies (10,11).
Harassment in the workplace can take many forms, including behaviors that affect an individual's employment, cause employee discomfort, impact work environment or interfere with work performance. Verbal harassment in the workplace includes insults, disrespectful or unpleasant jokes, name calling and unjustified and/or public criticism. Physical harassment encompasses behavior such as damaging property, threats and assaults. Sexual harassment includes requests for sexual favors and other undesired or unsolicited verbal or physical behavior of a sexual nature.
Excluding quid pro quo cases of sexual coercion and other behavior with obviously bad intent, to a certain degree, the problem of harassment can result from differences in perception. In a proportion of cases, the perpetrator has different beliefs on the offensiveness of their behavior. What is considered innocuous by one individual is not perceived that way by another. This difference in threshold concerning acceptable behavior inevitably leads to disputes. To be deemed unlawful, harassing conduct must objectively be viewed as creating a hostile work environment; however, the perspectives of the person being harassed are still very important and should always be considered. In the American court system, often the “reasonable person” standard is used. With this standard, in addition to the behavior being unwelcome and affecting the work environment of the victim, an objective reasonable person’s perspective would also view the behavior as harassment (12). Of course, this remains a subjective matter, which is greatly influenced by who this reasonable person is (12,13).
Harassment is prevalent in the medical profession (5,14–17). In academic and workplace environments in medical institutions and practices, harassment can, for instance, occur both in teacher–student relationships and in manager–employee relationships, involving students and trainees, medical personnel, managers and academic faculty. Shockingly, a meta-analysis of 51 studies demonstrated that almost 60% of medical students and trainees had experienced harassment or discrimination during their training, with female students and trainees being targeted more often than men (16). In an academic sample of clinician-researchers, one-third of women reported sexual harassment compared to 4% of men (17).
Being subjected to workplace harassment has been associated with many negative effects, such as increase of depressive symptoms, lower levels of vitality, employee discomfort, lower levels of job satisfaction and sense of safety at work, higher ethical or moral distress, increased turnover intentions, and suicidal behavior (8,9,18–20).
Efforts to curtail this type of behavior are particularly challenging. Perpetrators often hold senior leadership and supervisory positions. This contributes towards the fact that people who experience work-based sexual harassment seldom file complaints or report their experiences (21). Moreover, other factors such as stigma, fear of consequences and difficulties in proving allegations all play important roles in this (22,23).
Discussing these behaviors in our own field is often uncomfortable. Nonetheless understanding what happens, where, when and to whom is essential for efforts to transform culture and to eradicate problematic behaviors. We therefore aimed to determine the prevalence and potential risk factors of workplace sexual, verbal and physical harassment among headache professionals.
Methods
Design and setting
Using a non-experimental cross-sectional exploratory survey approach with a quantitative design, we conducted a global-wide survey aimed at headache professionals, including medical doctors, other healthcare providers and all those that are involved in the field of headache research. This study was part of a previously published effort to determine relevant career barriers for headache professionals (24). In short, (associate) members of the International Headache Society (IHS), and delegates of the 2019 International Headache Congress (IHC) were sent the web-based survey by email. Additionally, associate national headache societies affiliated with the IHS were requested to send out the survey to their members. The survey was conducted anonymously and voluntary.
Survey development
The survey was developed in English and used previously published surveys (25,26), and the experience of authors (IdB, AA, RHS, BB, RHJ, PPR and GMT). Consensus on the content of the questionnaire was reached by online discussion and email communication. The survey collected basic demographic information including country of birth, in addition to information on whether respondents had experienced harassment, the severity and perpetrator of harassment, and on if/how they responded, as well as other information that has been analyzed and reported separately (24). Finally, participants were asked how they responded to witnessing sexual harassment/being a bystander to sexual harassment. The web-based survey was first sent in September 2019 and closed in June 2020 after three reminders were sent to motivate partaking.
Data analysis
Data were analyzed using SPSS, version 25.0 (IBM Corp., Armonk, NY, USA). All questionnaires were examined for invalid responses as well as inconsistencies, which then were considered missing values. Descriptive statistics were used to capture demographic data. Primary outcomes were reported as percentages. To identify risk factors for experiencing sexual harassment and other types of harassment, we conducted logistic regression analyses on the following demographic characteristics as independent variables: age at time of survey completion, gender, race/ethnicity, region of employment and marital status. Risk factors are reported as the odds ratio (OR) with associated 95% confidence interval (CI). p < 0.05 was considered statistically significant.
Results
Participant demographics
In total, 580 participants completed the survey. One respondent identified with the non-binary gender identity. To ensure anonymity, this participant was removed from subsequent analyses. Just over half of participants were women (55.3%; 320/579). The highest percentage of responders was from Europe (39.6%; 229/579), the second most represented region was South East Asia (21.8%; 126/579) followed by North America (13.5%; 78/579). Only a minority, 4.0% (23/579) and 3.3% (19/579) were born in African and Eastern Mediterranean countries, respectively. In total, 556 (96.0%) of the respondents were healthcare providers and 480/579 (82.9%) participated in research. Moreover, the majority of respondents participated in both clinical and research activities (79.1%; 458/579). The majority of respondents have or had an academic career path (78,5%; 455/579). The majority of participants were in a relationship (82.7%; 479/579), and had children (71.8%; 416/579). Additional respondents’ characteristics can be found in Table 1 (24). Almost half of respondents indicated that they had experienced harrasment in the workplace (46.6%; 270/579). For participants who considered themselves healthcare providers, this was 46.6% (259/556), whereas, for those participating in research or academics, it was 41.0% (197/480) and 46.8% (213/455) respectively.
Demographics respondents.

1Three participants preferred not to disclose their age. 2One participant reported a non-binary gender identity. Because the results are separately reported based on gender, we had to exclude this participant to ensure anonymity. 3Participants with a difference in location birth and workplace: n = 38 (6.6%).
Prevalence, severity and perpetrators of sexual harassment
Overall, the prevalence of sexual harassment was 16.1% (93/578) (Figure 1A). In women, the prevalence of sexual harassment was 25.6% (82/320) compared to 4.3% (11/258) in men. For participants working in healthcare, research and academics, the prevalence of sexual harassment was similar, at 15.9% (88/555), 14.8% (71/479), and 15.6% (71/454), respectively. Most frequently, harassment was subjectively characterized as mild (62.4%; 58/93). Nevertheless, 8.6% (8/93) of respondents indicated the harassment as severe. Of note, 18.2% (2/11) of men reported sexual harassment that they were subjected to as severe (Figure 1B). The most frequent reported perpetrator was a boss, supervisor, attending or another senior employer (68.8%; 64/93), followed by patients (39.8%; 37/93) and colleagues (29.0%; 27/93). Respondents indicated sexual harassment by subordinates for 8.6% (8/93) of the time and for 2.2% (2/93) the victim did not know the harasser.

Reported sexual harassment in a work-based setting. In all questions, multiple responses were allowed. (A) Proportion of respondents reporting at least one experience of work-based sexual harassment. (B) Severity of the reported sexual harassment defined as mild, moderate or severe. (C) Individuals’ reaction to the occurrence of the sexual harassment affecting them in a work-based setting and (D) reaction to witnessing sexual harassment in a work-based setting.
Reporting of sexual harassment and bystander behavior
After incidences of sexual harassment, 51.6% (48/93) of respondents did not report or share information about the incident and only 7.5% (7/93) reported the harassment to human resources or management (Figure 1C). Of all respondents, 18.1% (105/579) indicated that they witnessed sexual harassment in the workplace. Interestingly, when sexual harassment was witnessed, 16.2% (17/105) of respondents indicated that they reported this to human resources, whereas 36.2% (38/105) kept quiet (Figure 1D). Victims reported more frequently that they confronted the harasser compared with what bystanders reported, 30.1% (28/93) versus 22.9% (24/105) (Figure 1C and 1D).
Risk factors for sexual harassment
Women were more likely than men to have experienced sexual harassment (OR = 6.8; 95% CI = 3.5–13.2) (Table 2). Being Caucasian was also associated with an increased risk of experiencing sexual harassment (OR = 2.8; 95% CI = 1.4–5.6). Additionally, respondents that were single were more likely to experience sexual harassment (OR = 2.3; 95% CI = 1.2–4.7).
Multiple logistic regression analysis of risk factors for sexual harassment.

OR, odds ratio; CI, confidence interval.
Prevalence and severity of other verbal and physical harassment
Among all headache professionals, the prevalence of verbal harassment was 40.4% (234/579). The prevalence of physical harassment was 5.5% (32/579) (Figure 2A). Although harassment was mostly indicated by the respondent to be mild (40.1%; 95/237) or moderate (33.3%; 79/237), almost one out of ten reports indicated it as severe (9.7%; 23/237) (Figure 2B).
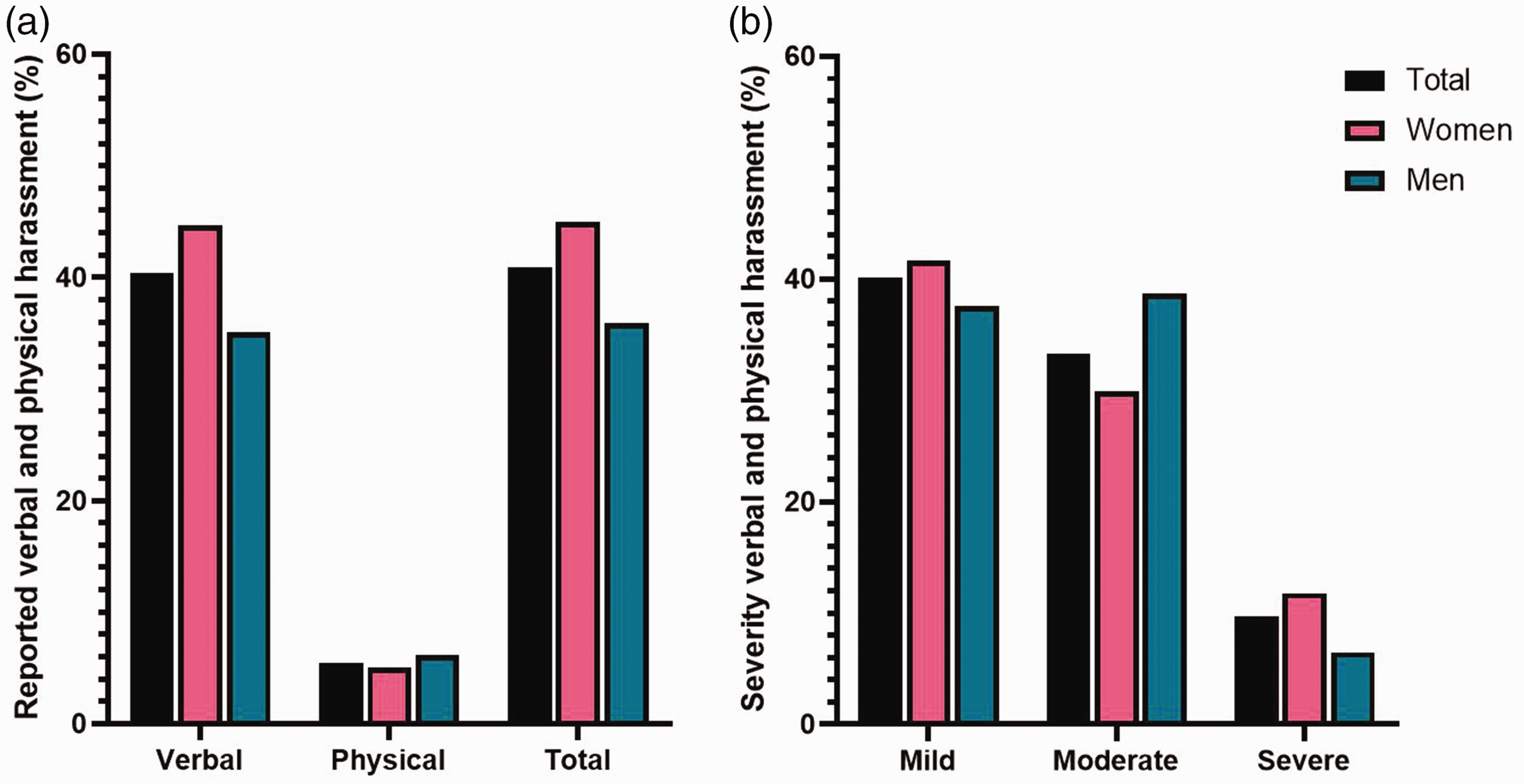
Reported verbal and physical harassment in a work-based setting. In all questions, multiple responses were allowed. (A) Proportion of respondents reporting at least one experience of work-based harassment that was not sexual in nature and (B) severity of the reported harassment defined as mild, moderate or severe.
Risk factors for other verbal and physical harassment
Although women appeared to experience also other verbal and physical harassment more frequently compared with men, this was not statistically significant (OR = 1.4; 95% CI = 1.0–2.0) (Table 3). Moreover, no other significant risk factors were identified.
Multiple logistic regression analysis of risk factors for verbal or physical harassment that was not sexual in nature.

OR, odds ratio; CI, confidence interval.
Discussion
In this survey, workplace harassment emerges as a common incident in the headache field, with almost half of respondents experiencing one or more type of harassment. Weak governance, as well as an underappreciation of the impact of the misconduct, can all contribute towards an environment in which conductors are not held accountable. As the global demand for equity within the workplace intensifies, it is also crucial to explore the possibility of sexual harassment as a contributor to enduring inequities, as well as its impact on career progression. We need to understand its occurrence to be able to enact advantageous interventions. We found a high prevalence (16.1%) of sexual harassment in the global headache field. Women were seven times more likely than men to experience sexual harassment. Sexual harassment is a deprivation of fundamental rights, as well as unprofessional and illegal, and should be treated as such. We also found a high prevalence of other types of harassment (40.9%). We could not identify specific risk factors for this type of harassment.
Almost 40% of respondents that experienced harassment indicated to have been harassed by patients. Harassment perpetrated by a patient or their family is a serious problem that the healthcare system has been experiencing for quite some time (27–30). Physicians report inadequate training in dealing with sexual harassment by patients and there are barriers for reporting incidents or even discussing these with colleagues or supervisors. We need ways to better address patients’ inappropriate behaviors towards healthcare providers (27). Employees should be attended to institutional policies and patients should be educated on behavioral standards. An overview of suggested recommendations to prevent and address harassment is provided in Table 4. Suggested recommendations could help foster a culture in which headache professionals feel more prepared to address harassment and where they are prepared to prioritize their own safety and wellbeing. However, and importantly, the majority of perpetrators were not patients. More than two-third of the respondents that experienced sexual harassment indicated to have been harassed by their boss or superior. This is especially shocking as we know that perpetrators accused of sexual harassment are rarely held to account. A US-based study of 125 faculty members in biomedical sciences and medicine who had been accused of sexual misconduct and received media attention (affecting at least 1668 individuals) showed that as many as 50 remained in academia, of whom 40% held positions at a different institution (27). Because these are cases in which victims reported behavior and there was media attention, this is likely the tip of the iceberg. We need to consider that several factors might impact an employers’ response to complaints of sexual harassment. Fear of defamation claims is one of those. Academic employers might find it easier to let harassers leave, resign or limit their contact with specific groups, in the hope of limiting public scrutiny and reputational damage. In this we need to recognize that human resource departments and other individuals involved often represent the institution and not the individual reporting the harassment. As such, they have other incentives influencing how they respond to the report. This of course only becomes an issue when harassment is reported.
Recommendations for preventing and/or dealing with incidents of harassment.

We need to recognize that reporting workplace harassment is not only incredibly important, but also exceedingly difficult. Often extreme power asymmetries are at work. This means that speaking out and trying to enact change within the profession is extremely hard. Frequently reported reasons for under-reporting also include belief that no action will be undertaken, fear of consequences and negative impact on own career, stigma, fear of worsening the situation, and not knowing how to report (22,23,28). Another contributing factor is the lack of a clear definition. Although some behaviors are obviously harassment (e.g. inappropriate unwanted physical contact), many behaviors are more subtle. This lack of a clear definition has been a barrier for reporting by individuals experiencing sexual harassment (29). It is important to realize that some of these unwanted behaviors have been “normalized”. Women in particular may not only downplay harassment, but may feel shame, guilt or stigma themselves, as well as second guess their own feelings and actions (29). Moreover, the lack of “evidence” or witnesses may stop victims from reporting harassment because they might fear a “their word against mine” situation. In our cohort, more than half of respondents kept quiet after harassment, whereas more than one-third of witnesses/bystanders did the same. Shockingly, 7.5% of victims felt compelled to leave their workplace. Less than 10% sought assistance from institutional resources to address the harassment. The low utilization rate is very worrisome. It is vital that we create an environment in which victims feel safe and empowered to report harassment. Healthcare and research institutions need policies clearly underlining the unacceptability of these behaviors. They also need to facilitate an appropriate investigation and protection for those who report harassment. They need to ensure accountability and transparent responses to unprofessional behaviors, including sexual harassment. They should work on fostering a safe and supportive environment that can encourage witnesses to come forward and victims to report incidents of harassment. The bare minimum that all organizations and societies can do is to ask potential hires or committee candidates whether they have violated harassment or any ethics policies or whether they left during active investigations. They should demand permission to gather information about such behaviors, investigations, warnings or suspensions from previous employers (30).
In addition to the high prevalence of sexual harassment, our data demonstrate that almost half of headache professionals experience harassment that was not of a sexual nature. Unfortunately, a hostile work environment is frequently reported across different medical and healthcare disciplines (16,23,26,31). Nonetheless, these data come at a crucial timepoint, as harassment and the “toxic hierarchical” culture in medicine are being openly challenged. Our findings indicate the need for a culture change and raise a call to action. A complicating factor is that what may work in one country and culture may not be relevant elsewhere. The effectiveness of proposed strategies needs to be meticulously evaluated in each environment and results should be communicated (32).
The limitations of the present study include the absence of a response rate. We prioritized giving all headache professionals the chance to participate over calculating a response rate. We therefore allowed national societies and representatives to send out the survey and could as such not calculate a response rate. Additionally, it is important to acknowledge that, as a result of limitations in our outreach efforts, we were only able to reach out to IHS (associate) members, IHC delegates and affiliated headache societies. Therefore, we recognize that not all headache professionals may have had the opportunity to participate. Moreover, a possible language barrier, outdated contact information or institutional blockage of emails may have potentially prevented part of the headache professionals from responding. Finally, although we contacted all IHS affiliated national societies (full list to be accessed from the IHS website: https://ihs-headache.org/en/about-ihs/affiliate-member-societies), we were unable to determine which representatives actually circulated the survey because this was on a voluntary basis. Although unfortunate, we still consider this an adequate first approach for this sensitive topic. To prevent responder bias, we strongly emphasized in our correspondence with prospective respondents that the survey was aimed at all headache professionals. Nonetheless, we cannot exclude that those respondents who strongly emphasized with this topic or the topic of our first manuscript (gender bias and challenges in career achievement) or who had experienced harassment were more likely to participate. Although an important result on its own, several ethnic groups were under-represented, which made it impossible to evaluate to which extent different ethnicities are a risk factor for sexual harassment. As such, although our finding of a reduced risk of experiencing sexual harassment for non-Caucasian respondents is interesting, this should be interpreted with caution. Moreover, we had an under-representation of individuals from African and Eastern Mediterranean countries. In addition, we did not collect data on age, job position, years of experience and workplace culture at the time of harassment incident(s). These may be important predictor variables if we had those data and should be included in future research projects. Furthermore, delving deeper into the circumstances surrounding incidents of harassment is likely to yield crucial insights into this challenging matter. To further investigate this issue, it is important to conduct a more comprehensive analysis aiming to determine the specific types of harassment that occur (such as verbal harassment encompassing bullying, name-calling, criticism). Additionally, it is important to examine the severity and duration of the harassment (whether it is a single occurrence, repetitive behavior by one individual, or involves multiple perpetrators) and its impact (such as increased employee absenteeism, heightened anxiety, diminished self-confidence). Also, determining the role of workplace culture, the organizational culture and leadership, both on the occurrence and attitude towards harassment, is likewise important. Finally, we need to consider that recall bias and social desirability bias might have prevented victims from reporting harassment in our survey. By ensuring anonymity, we hoped to prevent the second. If these biases occurred, this likely led to an underestimation of the prevalence of harassment. Likewise, individuals who experience severe or traumatic incidents might have been less likely to participate, ensuring a further underestimation of the issue. Another important matter that should be recognized is that we determined how many professionals had dealt with harassment. We did not examine how often victims were harassed. This likely leads to a further underestimation of the problem.
The following approaches, several which were previously discussed in more detail, might significantly reduce (sexual) harassment in the workplace (2). Professionals and organizations should strive towards creating a diverse, inclusive and respectful environment. Institutions should focus on diffusing the power structure, on reducing isolation, on improving transparency and accountability and on having working available supportive structures. If no working supportive structures are available, a system should be developed and, afterwards, its effectiveness should be evaluated. Furthermore, they should ensure diverse and accountable leadership that is clear about its dedication to reducing and eliminating all harassment. Institutions and leaders should clearly convey that reporting (sexual) harassment is honorable and courageous. Finally, effective sexual harassment training should be given. Harassment training should not be given out of “symbolic compliance”, as too often its primary aim is to protect from liability.
The effectiveness of training aimed at preventing sexual harassment is often not evaluated. Many training programs are aimed at providing information (e.g. about anti-harassment policies) and on changing attitudes (2,33). Research, however sparsely, has often demonstrated that a person’s believes and attitude are very resistant to change. It is important to realize that thoughts are in the end not harmful. The actions and behaviors of a person lead to harm of the victim. Given this, targeting behavior (even amongst those with sexist attitudes and those that do not see the harmful nature of their actions) appears to be better justified (2). Another important type of training is bystander intervention training (2,33). Bystander intervention training has long been used, especially in colleges and high schools. It focuses on creating awareness (recognizing problematic behavior), creating a sense of collective responsibility, providing bystanders with the skills and confidence needed to intervene (direct or indirect), and educating where available resources can be found. Simply put, bystander education equips bystanders with the skills necessary to recognize and take actions when problematic behavior occurs (33). Evaluating the effectiveness of these trainings is important and one should realize that what is helpful in one setting might not necessarily be part of the solution in another setting.
We are not the only medical field facing these challenges. Among emergency medicine residents, mistreatment was reported to occur in 29.9% of individuals a few times per year (34). However, in the vascular workplace, with a vast majority working in vascular surgery, 43% of responders indicated bullying, undermining behavior or harassment to have occurred in the last 12 months (35). Another example comes from the field of cardiology. Here, 44% of responders indicated that the worked in a hostile work environment (31). Although these types of studies are difficult to compare as a result of different endpoints and differences in the study populations, they do indicate that this issue is widespread in the medical community and that we might learn from one another when facing these challenges.
The prevalence of sexual harassment and other harassment is high in the headache field and women are more likely to experience sexual harassment than men. Understanding mistreatment within our professional field is an important first step in creating and maintaining a safe work environment. Our leadership can help create a culture in which everyone can speak out when perceiving or experiencing harassment. Our efforts might provoke other specialties and societies to also put this issue on their agendas. Moreover, our results may provide the impetus for headache societies, headache research groups and hospitals to develop action plans and re-examine and enforce policies addressing these damaging behaviors. We owe it to our (future) colleagues, ourselves and our patients to strive towards implementing such policies.
Key findings
Workplace harassment is common in the headache field, with almost half of respondents experiencing some type of harassment. Sexual harassment was reported by 16% of respondents, and women are seven times more likely to experience this. The Women’s Leadership Forum of the IHS recommends anti-sexual harassment training programs that focus on changing behavior, not on changing beliefs.
Footnotes
Acknowledgements
We kindly thank Carol Taylor for her assistance in distributing the survey.
Declaration of conflicting interests
I. de Boer reports independent support from the International Retinal Research Foundation and Dutch Heart Foundation. A. Ambrosini has received honoraria as a consultant and/or speaker for Novartis, Eli-Lilly and Teva. R. B. Halker Singh reports a research grant from Amgen. B. Baykan has nothing to disclose. D. C. Buse, PhD has received research funding from the US Food and Drug Administration, the National Headache Foundation and Amgen and received consulting fees from Amgen, Allergan/Abbvie, Lilly, Lundbeck and Teva. C. Tassorelli has received honoraria as a consultant and speaker for Amgen, Allergan/AbbVie, Biohaven, Eli Lilly, Dompé, Lundbeck, Medscape, Novartis and Teva Pharmaceuticals. Her research group has received research grants from Allergan/AbbVie, EraNet Neuron, Italian Ministry of Health. Her Institution has received payment for clinical trials from AbbVie, Eli Lilly, Lundbeck, Novartis and Teva Pharmaceuticals. R.H. Jensen has given lectures for Pfizer, Eli-Lilly, Merck, TEVA, Novartis, Lundbeck and Allergan, is investigator in clinical trials with Eli-Lilly, Novartis and Lundbeck and is director of Danish Headache Center, Lifting The Global Burden of Headache and Founder of Master of Headache Disorders at University of Copenhagen and has received research funding from University of Copenhagen, Rigshospitalet, Lundbeck Foundation, The Medical Society in Copenhagen, NovoNordisk Foundation and Tryg Foundation. P. Pozo-Rosich has received honoraria as a consultant and speaker for Amgen, AbbVie, Almirall, Biohaven, Chiesi, Eli Lilly, Lundbeck, Medscape, Pfizer, Novartis and Teva Pharmaceuticals. Her research group has received research grants from AbbVie, AGAUR, la Caixa foundation, EraNet Neuron, Instituto Investigación Carlos III, MICINN, Novartis, PERIS, RIS3CAT, Teva Pharmaceuticals; and has received funding for clinical trials from AbbVie, Amgen, Biohaven, Electrocore, Eli Lilly, Lundbeck, Novartis and Teva Pharmaceuticals. G. M. Terwindt reports independent support from the Dutch Research Council, and the Dutch Hearth and Brain Foundations, Dioraphte and IRRF, she reports consultancy or industry support from Novartis, Lilly and Teva, Allergan (Abbvie), Lundbeck.
Ethical statement
All responses were kept anonymous and no personal identifying information was collected. No ethical approval was required.
Funding
This work was supported by a granted project proposal by the International Headache Society.