
Abstract
Aim
The purpose of this systematic literature review is to assess the benefits of workplace-based occupational therapies and interventions, including acute and preventive medication, on headache intensity and frequency, related disability as well as work-related outcomes.
Methods
A search of the literature was conducted in PubMed, MEDLINE, Cochrane library, CINAHL and Embase using terms related to headache, workplace and occupational health. The Cochrane Collaboration’s risk of bias assessment tool was used on individual studies to assess internal validity and the Grading of Recommendations Assessment, Development, and Evaluation system was applied to studies by clinical outcome and used to rate quality of evidence.
Results
Fifteen articles were included in the systematic review. None of them were classified as low risk of bias according to the Cochrane Collaboration’s tool for assessing risk of bias. This systematic review found preliminary low-quality evidence suggesting that exercise and acupuncture can reduce workers’ headache pain intensity, frequency and related disability.
Conclusion
Although this systematic review provided preliminary low evidence in favour of work-based intervention, studies with more rigorous designs and methodologies are needed to provide further evidence of the effectiveness of workplace-based headache management strategies.
Introduction
Headache is considered a major health issue with a point prevalence of active headache disorders in the general population estimated at 46%. The specific prevalence of migraine is estimated at 11% (1) whereas according to the third edition of the International Classification of Headache Disorders, the lifetime prevalence of tension-type headache (TTH) in the general population ranges between 30% and 78% (2). Moreover, migraine prevalence in both sexes peaks between 25 to 55 years of age (3) whereas the peak prevalence for TTH is observed between 30 to 39 years of age (4) with those periods often regarded as the most productive years of employment (5).
Headache disorders are commonly associated with both significant direct and indirect costs; thus increasing the burden of active headaches disorders in the workplace (6,7). In fact, the economic impact of migraine among workers in the United States (US) has been estimated at over 11 billion and 12 billion US dollars in direct and indirect costs, respectively, of which 43% were accounted for by absenteeism-related expenses (8). However, those figures may represent an underestimation of the economic burden of migraine, as they do not include expenses incurred by rising presenteeism rates, defined as limitations of productivity time at work caused by health issues (9), which could account for as much as 89% of total migraine-related expenditures (5). In addition, given that TTH prevalence is considerably higher than that of migraine and often underdiagnosed (10), one may argue that the economic burden of TTH and overall primary headache disorders could be even higher.
Headache has been reported to be the most common condition leading to lost productivity hours (11) with an estimated 10.2 workdays lost per year including 7.8 of those days due to presenteeism (12). A Dutch study showed that 29% of employees from a manufacturing company still worked while experiencing headache symptoms (13). Productivity during episodes of migraine has also been reported to decrease by at least 50% in about half of those affected (3).
Due to their significant impact on productivity and workers’ well-being, coupled with their high prevalence in the working population, headache disorders should be considered a priority in occupational health. Although the subject of headaches and employee productivity is a cornerstone in terms of occupational medicine, to our knowledge there has been no published systematic review of literature reporting on the effectiveness of preventive and treatment interventions for primary headaches in the workplace. The purpose of this literature review is thus to review the effectiveness of current occupational therapies and interventions conducted in the workplace that aim to prevent or reduce headache-related symptoms and associated disability. The results of the review will guide future research and eventually the design of intervention programs to be implemented in the workplace environment.
Methods
Search strategy
A systematic search of the literature was conducted using the following online databases: PubMed, MEDLINE, Cochrane library, CINAHL and Embase. The search strategy combined controlled vocabulary specific to each database and free text words related to headache, workplace and occupational health. The following keywords were used: ‘migraine OR headache OR tension headache’ AND ‘workplace OR work environment OR worksite OR workers OR occupational health OR occupational disease’. Results were restricted to studies published from January 2000 to May 2015 with no limitation with regards to language. In addition, reference lists from previously published systematic reviews were hand-searched for any additional relevant studies. EndNote X7.4 (Thomson Reuter, PA, USA) was used to create a bibliographic database and manage the search results.
Selection criteria
Studies were deemed eligible if they included 1) participants aged over 18 years old; 2) a working population; and 3) implementation of a worksite-based prevention or treatment program for any type of primary headache. Two independent reviewers (MPG, AAM) screened citation titles and abstracts for eligible studies and a third reviewer (MD) was involved in resolving any disagreement between the two independent reviewers. Letters, editorials, commentaries, unpublished manuscripts, books and book chapters, conference proceedings, cost analyses, narrative reviews, systematic reviews, clinical practice guidelines as well as experimental and laboratory studies were excluded from the study.
Data extraction
A data extraction table was developed to facilitate the identification of relevant information from eligible articles (see supplementary material for details). The following information was extracted from the original studies: first author’s last name and publication year, studied population (sample size and participants’ characteristics), study design, work environment, description of interventions (type, duration and frequency), outcomes (related to headache and work performances: type and time of measurements) and results pertaining to the research question (difference in means, standard deviation, 95% confidence interval (CI), and p value whenever available).
Risk of bias assessment
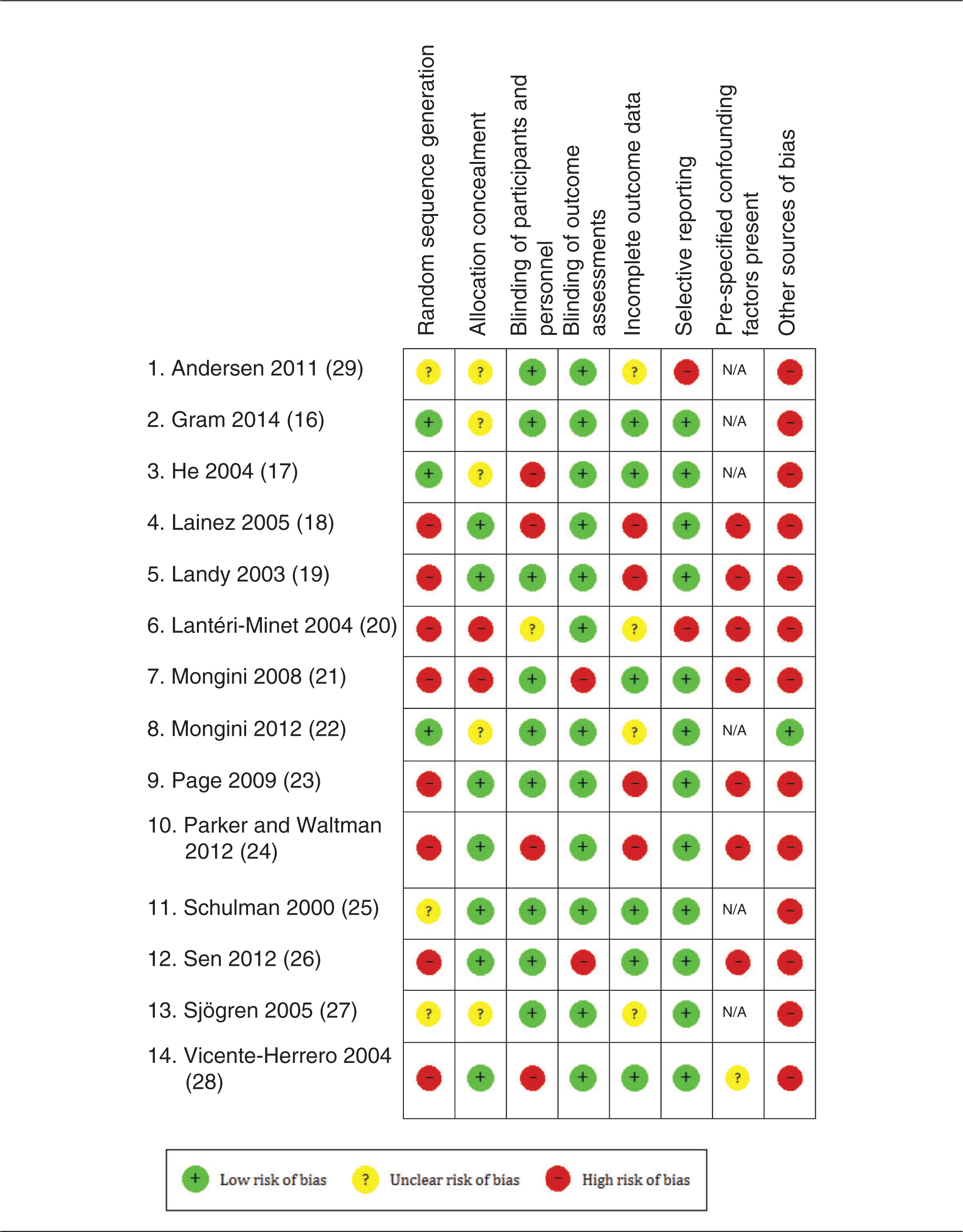
Random pairs of independent reviewers assessed the risk of bias with the Cochrane Collaboration’s tool for assessing risk of bias (version 5.1.0) in order to assess internal validity of included studies (14). The tool includes seven items divided into six domains of bias: selection, performance, detection, attrition, reporting and any other bias. For the particular case of non-randomised trials, confounding factors were pre-specified by the review team (age, gender, ethnicity and headache type). A critical assessment of the risk of bias level (high, low, unclear) was made for each item of the tool. Four key domains were identified by the research team as the most important domains: ‘Random sequence generation’, ‘allocation concealment’, ‘incomplete outcome data’ and ‘selective reporting’. Moreover, ‘Blinding of participant’ was deemed to be an additional key domain for trials including a drug therapy intervention. A summary assessment of risk of bias within a study was then made by grading a study at high risk of bias if one or more key domains is at high risk of bias, at unclear risk of bias if one or more key domains is at unclear risk of bias and at low risk of bias if all key domains were at low risk of bias.
Quality of evidence assessment
In order to rate the quality of evidence, the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system was applied (15) to the studies’ clinical outcomes (pain and disability, work-related outcomes) in each category of intervention. The assessment was based on the five downgrading factors (risk of bias, inconsistency, indirectness, imprecision and publication bias) and three upgrading factors (large effect, dose response and all plausible confounding). In brief, four of the authors (AL, MPG, MD, AAM) independently assessed the quality of evidence level. Assessments were then compared during a formal meeting during which consensus with regard to the strength of evidence was reached (high, moderate, low or very low). The quality of evidence level, coupled with the global risk of bias score, was taken into consideration in the Results/Discussion section. Meta-analyses were not performed due to high heterogeneity of scientifically admissible studies with respect to patient interventions, comparators and outcomes.
Results
Flow of the studies through the review
The initial search of the literature yielded 3451 articles. Following exclusion of duplicates and unrelated records, 29 full-text articles were assessed for eligibility. Seventeen articles were included for critical appraisal (16–32) of which four were based on the same population (21,30–32) and will be considered as one for now; the reasons for exclusion of the other articles are provided in Figure 1.
PRISMA flow diagram.
Studies’ characteristics
Patient populations under study included migraine exclusively in seven studies (18,20,23–26,28), mixed headache types (including migraine, TTH, myogenous neck and shoulder pain and unspecified or unknown types of headache) in four studies (19,21,22,29), and three focused exclusively on unspecified type of headaches (16,17,27). Among the 14 selected studies, eight involved a prevention program only (16,17,19,21–23,27,29), two involved an intervention program only (20,25) and four were mixed programs combining intervention and prevention (18,24,26,28). In the prevention subgroup of trials, five assessed the effects of exercise programs with or without headache-related educational content (16,21,22,27,29), two assessed the effects of educational programs only (19,23) and one assessed acupuncture treatment effects (17). In the intervention subgroup, one study assessed the effects of drug therapy (25) and one other studied the effect of orientating patients with migraine and without treatment towards their doctor for individual management of migraine (20). Finally, in the mixed intervention subgroup, three trials involved an exercise program combined with headache-related educational interventions (18,24) and one trial assessed the effects of prophylaxis drugs (26). Among these studies, the mean sample size was 337 (median: 247; range: 24–1881) and the mean follow-up period was nine months (median: 8 months; range: 10 weeks–3 years).
Risk of bias assessment
Risk of bias assessment.
Effects of interventions
Prevention
Education programs
Landy et al. and Page et al. (19,23) both conducted cohort studies in order to assess the effect of workplace-based education programs on headache frequency and disability. Page et al. (23) followed 247 participants for six months and reported a significant decrease in the mean number of days with headaches in the preceding three months (3.5 days). They also reported that at the end of the study the percentage of employees with minimal or infrequent disability increased while the number of employees with moderate or severe disability decreased. Landy et al. (19) followed 268 participants for three months and reported a decrease of 35.7% in the number of days with ≥ 50% disability (n = 164). Similarly to the findings of the other study (23), participants with little disability increased during the follow-up.
Page et al. (23) also explored work-related outcomes and reported significant reductions in missed work days/1000 employees with migraines for three months (−200 days) due to headache and in days worked with headaches/1000 employees for three months (−3000 days). These results are considered very low-quality evidence (downgraded for study design, risk of bias and imprecision of results).
Exercise programs
Andersen et al. (29) assessed the variation of headache frequency in 198 participants randomised into either 12- or 2-minute training groups or a control group (CG). After the 10-week intervention, the decrease in mean frequency of headache was higher in the 12-minute training group (−0.79; 95% CI: −1.2 to −0.37) than the 2-minute (−0.64; 95% CI: −1.0 to −0.23). No change was observed in the CG (0.06, 95% CI: −0.23 to 0.15).
Gram et al. (16) investigated the effects of a 20-week strength training program on headache intensity (0–10 numeric rating scale (NRS)), and frequency (days/month). Analysis of the 351 participants revealed a decrease in headache intensity for both supervised training groups (−0.4; SD = 1.8 and −0.4; SD = 1.4) whereas the CG (+0.7; SD = 2.2) did not improve. Regarding the change in headache, participants in both supervised training groups decreased their headache frequency (−0.4 days/month; SD = 3.7 and −0.7 days/month; SD = 2.6) whereas participants in the CG showed no significant change (+0.6 days/month; SD = 4.4).
Mongini et al. (21) conducted a non-randomised controlled trial (RCT) on 384 participants to assess the effects of relaxation and posture exercise on headache frequency and disability. After six months, mean number of days with headache in the intervention group (IG) decreased significantly (−2.43 days/month; 95% CI: −3.19 to −1.74) compared to the CG (0.02 days/month; 95% CI: −0.62 to 0.73). Mongini et al. (22) also conducted a large (N = 1881) cluster RCT assessing the effects of a six-month multicomponent exercise program on headache frequency. Both IG and CG experienced a reduction in mean number of days with headache, although the magnitude of the difference was higher in the IG (−2.53; 95% CI: −3.01 to −2.04) than the CG (−0.81; 95% CI: −1.29 to −0.33).
Sjögren et al. (27) in their cross-over study assessed the effects of non-supervised resistance training for upper and lower extremities on headache intensity. The 53 participants were randomised into two groups. After the 30-week trial period, the mean difference in headache intensity was lower in the intervention period (−0.64 point/10; 95% CI: −0.28 to −1.00).
Overall, all of the five articles found a beneficial effect of an exercise program on headache pain intensity and frequency, and disability outcomes. However, the quality of the evidence was rated as low (downgraded for risk of bias).
Acupuncture
He et al. (17) in an RCT followed 24 office workers for a three-year period to assess the effects of a short course of acupuncture treatment. Results showed that acupuncture can reduce neck and shoulder pain intensity (82% improvement over 10 treatments) and headache frequency (70% improvement over six treatments – no raw data provided). Improvements observed in favour of the intervention group were maintained at the three-year follow-up. The quality of evidence was rated as low (downgraded for risk of bias and imprecision of results).
Treatment interventions
Medication
Schulman et al. (25) in an RCT followed 206 migraine patients during nine months to determine the effects of sumatriptan on migraine-related workplace productivity loss. Results showed that sumatriptan when compared with a placebo leads to decreased productivity loss (36.8 vs 72.6 minutes), shorter return to normal work performance at two hours (70% vs 30%) and across the work shift (84% vs 58%), and a shorter median time to returned to normal work performance (54 vs 209 minutes). The quality of evidence was rated as very low (downgraded for risk of bias, inconsistency of result and imprecision of results).
Other interventions
Lantéri-Minet et al. (20) followed 575 participants with migraine over 18 months in order to assess the effects of referring patients to their physician (IG) compared to a group of participants already medically followed for migraine management (CG). The mean duration of crisis was significantly shorter in the IG (29.5% vs 24.8% <4 hours crisis). When comparing the three-month period before inclusion to the one after the intervention, there was a reduction of 12.4% in participants stopping their work due to migraine in the CG compared to 10.9% in the IG. Quality of evidence was rated as very low (downgraded for risk of bias, indirectness of evidence and imprecision of results).
Mixed programs (prevention and treatment)
Education and symptomatic medication
Parker and Waltman (24) followed 28 participants during 12 months to explore the combined effects of education and medication on headache frequency, severity and associated disability in a pilot study. Results showed that for 76.1% of participants, the frequency of headaches over time decreased by at least 50%, the severity of headaches by 50% in 31.3% of them, and a reduction of disability scores was observed by 50% in 66.5% of them.
Vicente-Herrero et al. (28) followed 406 employees for seven months to evaluate the effect of medication on workplace and non-workplace consequences of migraine headache. Results showed decreased interference of headache with daily (−70.4% of patients reporting interference) and social activities (−72% of patients reporting interference). Two studies assessed the effects of medication (rizatriptan) and education on work-related outcomes (18,28). Lainez et al. (18) followed 259 participants for three months and reported significant reduction of absenteeism (−1.25 days/3 months) and increased productivity (−3.65 days/3 months). Vicente-Herrero et al. (28) provided data from 436 participants and reported a significant reduction of absenteeism (odds ratio (OR) = 0.5, 95% CI: 0.32–0.82), and that the percentage productivity at work with migraine increased from 59% at baseline assessment to 94.8% seven months later.
Evidence was deemed to be of very low quality for these three studies (downgraded for study design, risk of bias and imprecision of results).
Preventive and symptomatic medication
Results by intervention programs.
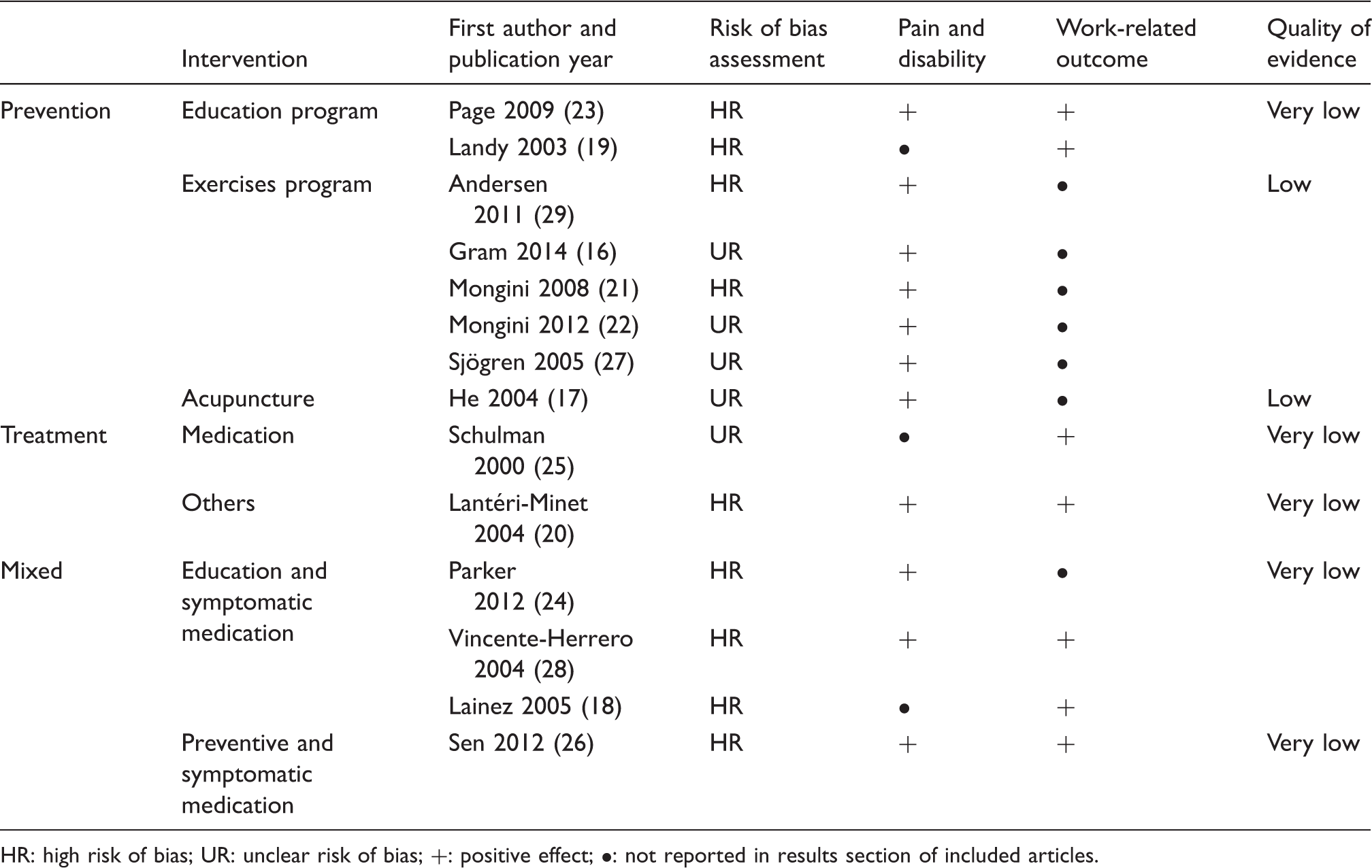
HR: high risk of bias; UR: unclear risk of bias; +: positive effect; •: not reported in results section of included articles.
Discussion
Altogether, the results showed that several types of intervention aiming at the prevention and treatment of primary headaches in the workplace have been assessed. Exercise programs, medication and education were the most frequently reviewed intervention whereas three studies included mixed interventions combining education and medication. The systematic review found preliminary low-quality evidence suggesting that exercise program (strength, stretch, resistance, relaxation and postural training) and acupuncture can prevent high pain intensity and frequency as well as disability in workers with headaches. For all other prevention and intervention programs, the overall quality of evidence was too low to draw any conclusions with regard to efficacy in reducing headache pain intensity, frequency, and disability or improving work-related outcomes. The risk of bias assessment indicated that a majority of studies were classified as studies with high risk of bias (9/14) or unclear risk of bias (5/14), none of the included studies were classified as having low risk of bias and many of them showed issues with confounding factors, random sequence generation and incomplete outcome data reporting.
Two previously published systematic reviews (33,34) have assessed the effects of medication on headache. Banzi et al. (33) reported no effect of selective serotonin reuptake inhibitors and serotonin norepinephrine reuptake inhibitors on duration and intensity of TTH. However, this review included but was not specific to working populations and focused only on TTH. Burton et al. (34) focused on the effects of migraine medication treatment on workplace productivity. Amongst the studies assessing absenteeism and productivity, all studies related to triptan therapy were associated with a significant improvement of worker productivity and a reduction of absenteeism. These results are similar to those reported in the present systematic review. However, the quality of this evidence was not assessed in the Burton study (34) and classified as very low in ours. Overall, the systematic review process yielded only five medication studies investigating primary headache medication interventions conducted in the workplace. Subsequently, the breadth of medication interventions explored is limited and the results presented in this systematic review (in the working environment context) should under no circumstances be considered as evidence-based recommendations for practice in the working environment due to the limited and preliminary nature of the evidence. In fact, under such circumstances where most of the evidence is rated very low, further research is very likely to have an important impact on our confidence in the estimate of treatment effects.
For instance, the Canadian Headache Society Guideline: Acute Drug Therapy for Migraine Headache (35) concluded that there was strong evidence supporting the use of the following medication in acute migraine therapy: almotriptan, eletriptan, frovatriptan, naratriptan, rizatriptan, sumatriptan, zolmitriptan, acetylsalicylic acid (ASA), ibuprofen, naproxen sodium, diclofenac potassium, and acetaminophen whereas the American Academy of Neurology and the American Headache Society (36) concluded that Divalproex sodium, sodium valproate, topiramate, metoprolol, propranolol and timolol can be recommended for the prevention of migraine. The most recent TTH headache treatment recommendations (e.g. European Federation of Neurological Societies guideline on the treatment of TTH (37), National Institute for Health and Care Excellence (NICE) headaches in over 12 s: Diagnosis and management (38) suggest simple analgesics and non-steroidal anti-inflammatory drugs for the treatment of episodic TTH while carefully balancing risk-benefits considerations and patients’ preferences.
Study limitations
Although every attempt was made to include all relevant studies, as in all systematic reviews it is possible that other relevant literature was missed. The current systematic review used strict criteria for the selection of studies conducted in the working environment in order to specifically tease out the efficacy of such approaches on work-related outcomes. However, there is a wide body of evidence assessing the comparative efficacy of several prevention strategies and interventions programs and there is little doubt that the related results should also be carefully considered in the development of headache treatment and prevention programs in the workplace. Additional relevant information regarding preventive and acute interventions for primary headaches can be found in recently published systematic reviews and clinical guidelines (35–37,39,40). Furthermore, an inherent limitation to the included studies lies in the use of mixed populations which hinder to discover the true effect of the intervention. Specific headache types are likely to respond differently from one another and should therefore be studied in subgroups. Finally, due to the overall heterogeneity of admissible studies as well as the high risk of bias and imprecision of results reported in the original studies, it was not possible to conduct a meta-analysis on any of the pre-specified clinical outcomes.
Consideration for future research
Future studies should be carefully designed and include proper control intervention and randomisation strategies. Selection of participants should be based on the International Classification of Headache Disorders to ensure proper comparability of population across studies. Intention-to-treat analyses should be considered and strategies for the management of missing data should be described. Precision of results was also an important issue in the current review, as several studies did not provide proper mean results with CIs. Proper reporting of trial results is essential in the development of recommendations and should be considered in future studies. Occupational cohort studies comparing interventions were considered in these systematic reviews, since, when properly conducted, they provide relevant and valuable information with respect to the applicability of the proposed interventions. Working environment is often concerned with the productivity and stability of their working processes. Therefore, non-randomised studies comparing interventions in two similar working environments usually yield better acceptability by the employer and increased employees participation (41). However, as elegantly stated by Kristensen (2005), ‘there may be many good reasons for not performing a randomised controlled trial in an occupational setting. But there are no good reasons for ignoring the problems created by not applying such a design’. Therefore, occupational intervention studies should always be conducted in light of the methodological considerations of the respective study designs, while also taking into account the ecological value of the study.
Conclusion
Consequences of headache represent a major burden in the workplace with significant costs. Few studies have assessed secondary prevention or therapeutic interventions conducted at work. This systematic review suggests that exercises and acupuncture can reduce future pain episodes and related disability in workers with headaches. Studies with more rigorous designs are needed to provide further evidence for workplace-based intervention effectiveness aimed at secondary prevention and treatment of primary headaches.
Clinical implications
Point prevalence is very high in the general population and has been reported as the most common condition leading to lost productivity hours. Overall the reviewed studies were classified as high risk or unknown risk of bias. There is low-quality evidence that exercise and acupuncture were beneficial therapeutic modalities for secondary prevention of pain and disability in workers with headaches. Overall design and methodology should be improved in future studies while also considering work environment specifics.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.