
Abstract
This study sought to determine if Whites and African-Americans respond similarly to headache treatment administered in ‘real-world’ headache specialty treatment clinics. Using a naturalistic, longitudinal design, 284 patients receiving treatment for headache disorders completed 30–day daily diaries that assessed headache frequency and severity at pretreatment and 6–month follow-up and also provided data on their headache disability and quality of life at pretreatment and 1–, 2– and 6–month follow-up. Controlling for socioeconomic status and psychiatric comorbidity, hierarchical linear models found that African-Americans and Whites reported significant reductions in headache frequency and disability and improvements in life quality over the 6–month treatment period. African-Americans, unlike Whites, also reported significant decreases in headache severity. Nevertheless, Africans-Americans had significantly more frequent and disabling headaches and lower quality of life after treatment relative to Whites. Although Whites and African Americans responded favourably to headache treatments, more efficacious treatments are needed given the elevated level of headache frequency that remained in both racial groups following treatment.
Introduction
Headache disorders constitute serious public health and medical dilemmas in the USA. High rates of employee absenteeism, increased physical impairment and reduced quality of life are common in persons with headache disorders (1–7). Prophylactic (i.e. preventive) treatments have consistently been shown to reduce the frequency and severity of a variety of chronic headache conditions (1, 8–10). It is important to note, however, that the efficacy of these treatments has been determined largely in the context of highly controlled, randomized clinical trials. Far less research has evaluated the effectiveness of headache treatments when they are administered by diverse groups of healthcare professionals (e.g. psychiatrists, neurologists, family medicine practitioners) across a variety of ‘real-world’ treatment settings (e.g. hospitals, headache specialty clinics, primary care settings).
To our knowledge, only one published study has evaluated the effectiveness of headache treatments in ‘real-world’ clinical settings. The study found significant reductions in headache intensity and frequency in patients who met diagnostic criteria for medication overuse headaches and were being treated in a multidisciplinary treatment centre that integrated neurological, psychological and behavioural treatment (11). However, most headache treatment occurs in primary care settings and rarely includes multidisciplinary care (i.e. most care is provided almost exclusively by a single practitioner; (11)). Pharmacological treatment often serves as the ‘standard of care’, with preventive medication representing the optimal treatment approach for patients seeking treatment for chronic headaches.
A crucial goal of Healthy People 2010 is to eliminate health disparities in important demographic subgroups of the US population. This initiative is in response to research showing that people of colour experience poorer clinical health outcomes than Whites, as measured by functional status, pain relief and quality of life (12–15). In particular, studies on persons with pain disorders indicate that non-Whites in the USA are at higher risk than Whites for suffering negative treatment side-effects and complications, such as unnecessary suffering, functional disability and increased length of hospitalization (16). Although many race-related differences in headache prevalence and characteristics have been documented over the past decade, the role of race/ethnicity has received almost no attention in treatment-outcome studies. Regarding the former, African-Americans have lower prevalence rates of migraine and tension-type headache than Whites (in US and international samples), although rates of migraine may be higher in African-Americans than Whites in patients receiving headache treatment in health maintenance organizations (17). Much research also shows that African-Americans report more frequent and severe headaches than Whites (2, 18). To eliminate health disparities, it is important for researchers and practitioners to determine if contemporary treatments work equally well in Whites and African-Americans living with chronic health and pain conditions, such as headache disorder.
The current study evaluated race-related differences in headache treatment outcomes in a sample of patients seeking treatment in four headache specialty care clinics throughout Ohio. Given the extant literature indicating that African-Americans respond less favourably to treatments across a wide variety of health disorders, including pain conditions (19–21), it was hypothesized that Whites receiving treatment for their headache disorders would exhibit greater reductions in headache frequency, severity and disability and greater increases in quality of life over the course of treatment compared with African-Americans.
Patients and methods
Sample characteristics and study procedures
This study enrolled 311 patients seeking treatment for primary headache disorders in four out-patient headache specialty treatment clinics in Ohio's four largest cities. Of these 311 patients, 27 self-identified their race as ‘Hispanic,’ ‘Asian American/Pacific Islander,’ ‘Native American,’ or ‘Other’ and were excluded from subsequent data analyses, yielding 171 White and 113 African-American patients (see Fig. 1). Of these 284 patients, 230 received prophylactic medications at participating clinics. The 230 patients were recruited through four headache specialty treatment centres in: Columbus (n = 89), Toledo (n = 80), Cleveland (n = 50) and Cincinnati (n = 11). Study inclusion criteria were: (i) ≥ 18 years old; (ii) satisfying International Headache Society (IHS) criteria (2003) (22) for episodic migraine, chronic migraine, episodic tension-type headache (ETTH), chronic tension-type headache or medication overuse headache; (iii) the physician determined that the patient should begin new preventive medication therapy; and (iv) provision of informed consent. Because the study utilized a naturalistic design, no exclusion criteria were applied in an effort to form a sample that was representative of clinic patients.

Patient flow diagram.
Recruitment materials (i.e. brochures and posters) were distributed to participating clinics for display and distribution to patients. Although patients were recruited by site physicians and nurses during the patient's initial clinic visit, only the physician determined patient eligibility. Because persons of colour were relatively underrepresented in all four treatment centres, all racial minority patients who presented for treatment were approached for recruitment and enrolment into the study. The larger pool of White patients enabled the project to use a recruitment strategy in which only every fifth White patient was approached for recruitment and enrolment. Eligible patients who expressed interest in the study provided written informed consent in the treatment clinic. Patients were initially assessed at pretreatment and were then treated and re-assessed at 1-, 2- and 6-month follow-up. The follow-up appointment times were recommended by physicians participating in the study and represented the typical treatment schedule used by physicians to monitor treatment effectiveness, identify possible negative treatment side-effects, and the need for medication adjustments (see Fig. 2).

Study assessment and treatment schedule.
At the initial visit, and if abortive medication was indicated, patients who were not already receiving these treatments were prescribed acute medications (i.e. non-steroidal anti-inflammatory drugs, triptans, etc.). Modifications in acute treatments were implemented for those patients who were already taking abortive medications for their headache. At the second visit, which occurred 1 month after the initial visit, the need for preventive medication based on the patient's headache activity during the past month was determined. At this point, preventive medication was prescribed as clinically indicated. It is important to note that preventive medication could not be prescribed until the second visit in order to permit pretreatment assessment of headache activity and quality of life. Patients were then scheduled to attend two follow-up visits 2 and 6 months after the initial visit.
The study's naturalistic design and its assessment/treatment schedule were implemented for the following reasons. First, the time points at which the four assessments were completed by participants represent the typical timing of treatment visits that patients undergo in participating headache treatment clinics. Second, the naturalistic and observational nature of the study introduced no changes to the usual treatment provided to clinic patients. Finally, patients were followed over a period of 6 months because this period was believed to provide sufficient time for patients' headaches to respond to newly initiated treatments.
Assessment methodologies
As shown in Fig. 2, the study collected data from patients at four assessment periods. Study data were collected through three different assessment methodologies.
Headache diagnosis
During the initial patient–physician interaction, the physician diagnosed the patient's current headache disorder(s) using IHS (2003) criteria (22). The physician also documented each patient's past and current pharmacological headache treatments.
Thirty-day daily diaries
At the conclusion of the initial visit, and also after completing their 6-month visit, participants received a self-administered, paper-and-pencil daily diary they used to record the frequency and severity of each headache experienced during the next 30 days. The first 30-day period was the interval between the patient's initial visit and their second visit and the second 30-day period occurred after the patient's final treatment was administered at the 6-month follow-up (see Fig. 2). Patients received their new preventive therapy at the second visit. Headache frequency was operationally defined as the ‘number of days over the 30-day period during which patients indicated that they experienced a “mild”, “moderate” or “severe” headache’. Headache severity was assessed daily for each headache using a 4-point scale (0 =‘No pain’, 1 =‘Mild’, 2 =‘Moderate’ or 3 =‘Severe’). Average headache severity scores were calculated by summing all headache severity ratings and dividing this sum by the number of headaches experienced over the 30-day period.
Headache Disability Inventory (23)
The 25-item Headache Disability Inventory (HDI) assessed the burden of chronic headaches and measured the perceived impact of one's headaches on emotional functioning and daily activities. The HDI was completed at pretreatment and 1-, 2- and 6-month follow-up. The HDI demonstrated excellent internal consistency (α= 0.90; current study), with higher scores indicating greater headache disability.
Modified Migraine Specific Quality of Life Questionnaire (24)
A 14-item version of the Migraine Specific Quality of Life Questionnaire (MSQL) was used to assess the long-term impact of headache disorders on patients' quality of life. Because MSQL items refer only to migraines, the term ‘migraine’ was replaced with ‘headache’ in each relevant item. For example, the original MSQL item ‘In the past 4 weeks, how often have migraines interfered with how well you dealt with family, friends and others close to you’ was changed to ‘In the past 4 weeks, how often have your headaches interfered with how well you dealt with family, friends and others close to you’. This measure was completed at pretreatment and 1-, 2- and 6-month follow-up. The 14-item measure demonstrated excellent internal consistency (α= 0.88, current study), with higher scores indicating greater impairment.
Demographic characteristics
As part of the 30-day diary, patients indicated the racial group with which they most identified, their age, gender, number of years of education, employment status, health insurance status (Health Maintenance Organization, Preferred Provider Organization, private insurance, Supplemental Security Income) and annual income.
Socioeconomic status
To obtain a more comprehensive estimate of each patient's socioeconomic status (SES), a principal components analysis (PCA) was conducted using the variables ‘Number of Years of Education Completed’ and ‘Annual Income’. These two variables are used commonly when creating composite measure of SES (25). The PCA identified one factor in the analysis (eigenvalue = 1.35), which accounted for 67.4% of the variance in the two measures. Years of education completed and annual income loaded equally onto the factor (Factor Loading = 0.82). The PCA also calculated an SES factor score (M = 0.0,
Comorbid psychiatric conditions
Psychiatric disorders were assessed and diagnosed using the Primary Care Evaluation for Mental Disorders (PRIME MD; (26)). The PRIME-MD was administered to participants by trained research staff during a telephone interview conducted within 2 days of the pretreatment visit. The Prime-MD yields a subset of diagnoses included in the Diagnostic and Statistical Manual of Mental Disorders (DSM IV; (24)), including mood and anxiety disorders, as well as alcohol (abuse/dependence), eating disorders and somatoform disorders. In the current study, the presence of a psychiatric condition was dichotomized as 0 =‘No Psychiatric Condition Present’ or 1 =‘One or More Psychiatric Conditions Present’).
Data analytic procedures
Independent group t-tests for continuous variables and χ2 tests of association for categorical measures were calculated to test if Whites and African-Americans differed on sociodemographic variables, headache diagnoses or headache characteristics at pretreatment and to identify differences between treatment completers and treatment dropouts on demographic variables, headache diagnoses, headache characteristics, and acute and preventive headache treatments. A patient was operationally defined as a ‘drop’ if they missed one or more treatment visits and did not reschedule and attend the missed visit(s).
To test if Whites and African-Americans responded similarly to newly initiated preventive medications, outcome analyses focused on two sets of measures. Headache-specific quality of life (as assessed by the modified MSQL) and headache disability (as assessed by the HDI) were assessed at pretreatment and 1-, 2- and 6-month follow-up. Headache frequency and severity were assessed through 30-day daily diaries completed immediately after pretreatment and 6-month follow-up (these measures were not completed at 1- and 2-month follow-up). Outcome analyses were conducted using an intent-to-treat approach. The intent-to-treat analyses used data provided by patients who were enrolled in the study, received at least one type of preventive medication, and who may (or may not have) completed treatment and all assessments through 6 months.
Hierarchical linear modelling (HLM; (27)) compared Whites and African-Americans at pretreatment on headache frequency, severity, disability and quality of life and determined if Whites and African-Americans reported similar rates of change on the study's four outcome measures. All participants, including those who had missing observations at one or more assessment periods, were included in HLM analyses. HLM was chosen over traditional
Results
Race, sociodemographics and headache characteristics at pretreatment
As shown in Table 1, the average patient was 36.8 ± 10.2 years old (range 18–66 years), had completed 14.0 ± 2.2 years of education, and had a primary headache diagnosis of episodic migraine without aura (38%). Almost all participants (99%) had health insurance; most were insured through preferred provider (38%) or health maintenance organizations (31%). Thirty per cent of participants reported annual incomes of < $20 000, 39% reported incomes between $20 001 and $40 000, 19% reported incomes between $40 001 and $60 000 and 12% reported annual incomes > $60 001. At pretreatment, the average participant had experienced one or more headaches on 17.4 days during the past 30 days.
Sociodemographic characteristics and headache diagnoses of White and African-American patients

χ2 tests of association and independent sample t-tests characterized associations among race, sociodemographics, headache diagnoses and headache characteristics at pre-intervention. As shown in Table 1, African-Americans (M = 13.5) had completed fewer years of education than Whites (M = 14.3) (P < 0.01). African-Americans (74%) were more likely than Whites (61%) to be diagnosed with a psychiatric comorbid condition (χ2(1) = 5.1) (P < 0.03). African-Americans (M =−0.20) also had lower SES factor scores than Whites (M = 0.12) (P < 0.02). Table 1 also shows that Whites (54%) were more likely to be diagnosed with episodic migraine headache (with or without aura) compared with African-Americans (37%) (P < 0.02). Finally, African-Americans (6%) were more likely than Whites (0%) to be diagnosed with ETTH (P < 0.01), although ETTH was reported by very few patients.
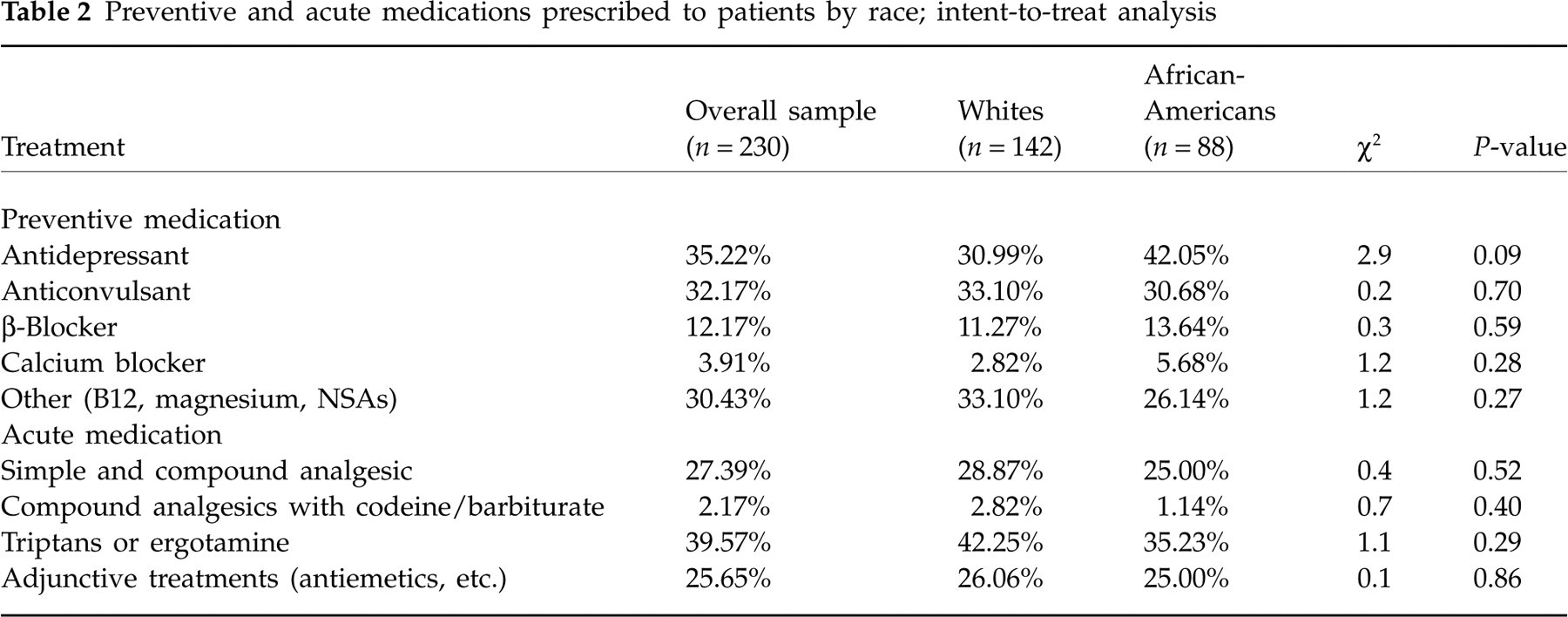
Table 2 shows preventive and acute medications prescribed to patients during the course of the study. African-Americans (42%) were marginally more likely than Whites (31%) to be prescribed antidepressant(s) as preventive medication (P = 0.09). African-American and White patients were equally likely to be prescribed adjunctive supplements, anticonvulsants, β-blockers and calcium channel blockers. The prescription of acute medications by physicians was similar across White and African-American patients.
Patterns of treatment attrition
At the 6-month follow-up, 95 of 142 Caucasian patients (67%) and 42 of 88 African American patients (48%) had attended all scheduled treatment sessions. Patterns of treatment attrition (by race) are shown in Fig. 1. Independent sample t-tests and χ2 tests of association compared completer (n = 137) to non-completer patients (n = 93). Sixty-nine per cent of participants who completed the study were Caucasian, while only 51% of participants who dropped from the study were Caucasian (P = 0.004), indicating that African Americans were more likely to prematurely terminate their headache treatments.
As shown in Table 3, non-completers (Non) were significantly younger than completers (Com) (MNon = 34.8, MCom = 37.9, P < 0.03), had significantly fewer years of education (MNon = 13.6, MCom = 14.2, P < 0.05) and had lower SES scores (MNon =−0.18, MCom = 0.11, P < 0.04). Non-completers were more likely to be diagnosed with chronic tension-type headache than completers (22.6%Non, 10.3%Com, P < 0.02) and medication overuse headache (10.8%Non, 2.9%Com, P < 0.02). Completers were more likely than non-completers to be diagnosed with one type of headache (66.9%Com, 51.6%Non, P < 0.02).
Preventive and acute medications prescribed to patients by race; intent-to-treat analysis
Demographic and behavioural differences between treatment completers and dropouts
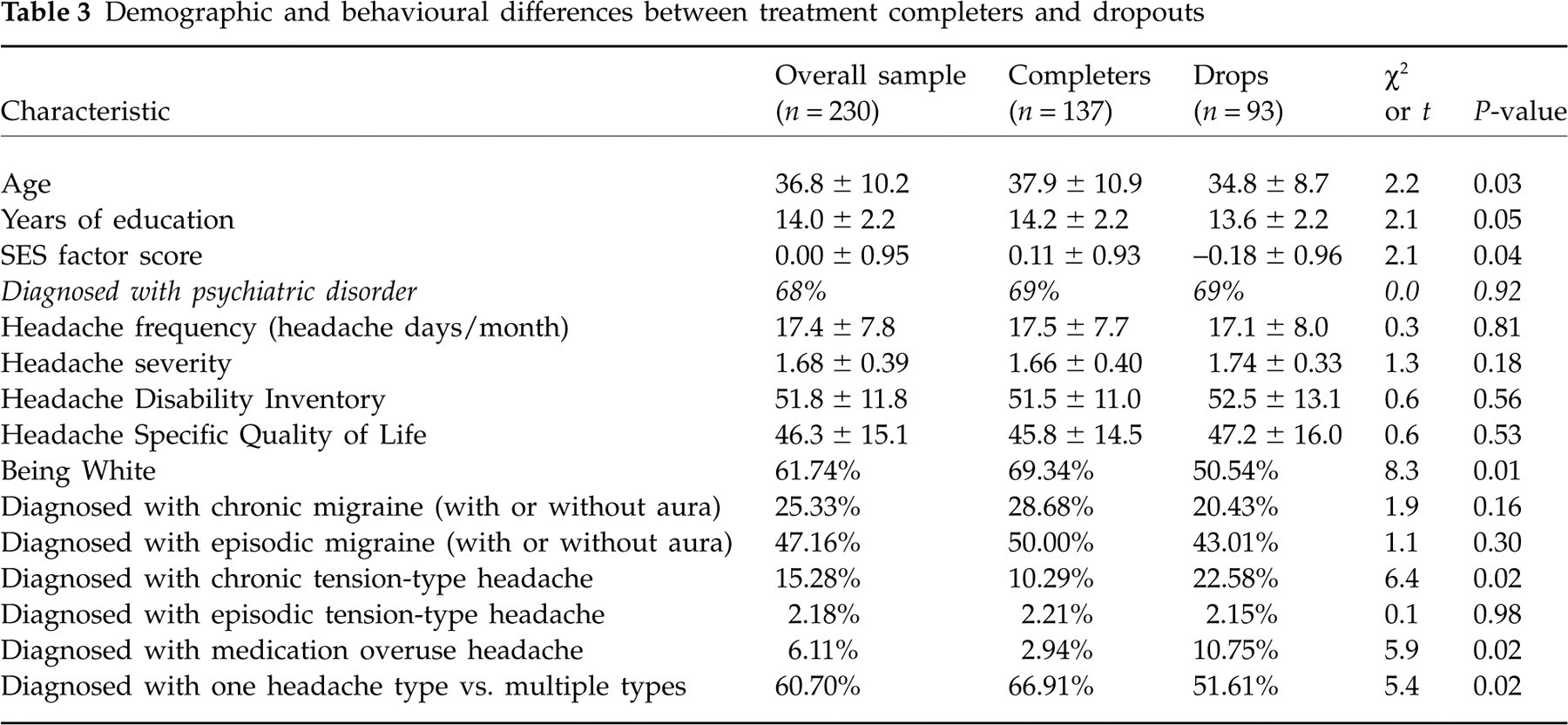
With respect to acute and prophylactic medications, significant differences were observed only on prescription of adjunctive supplements; non-completers (30.1%) were more likely to be prescribed adjunctive supplements than completers (14.5%). Importantly, completers and non-completers did not differ at pretreatment in headache frequency, severity, disability or quality of life (all P > 0.10).
Treatment outcome analyses by race
The observed means tested in treatment outcome analyses conducted using HLM are shown in Table 4. Treatment outcome analyses conducted using HLM are shown in Table 4. As shown in Table 4, African-Americans had significantly poorer headache-specific quality of life and more frequent and severe headaches at pretreatment compared with Whites (all P < 0.05). Both Whites and African-Americans reported significant reductions in headache frequency, headache disability and impairments in quality of life; however, only African-Americans reported significant reductions in headache severity. In terms of reduction in headache frequency, both Whites and African-Americans experienced approximately one less headache per month (or five fewer headaches over the entire follow-up period). Table 4 also shows that, even after reporting significant improvements on all four outcome measures, African-Americans still differed from their White counterparts in headache quality of life (P < 0.01) and reported marginally greater headache frequency and disability than Whites (P < 0.10). The outcome analyses, conducted using the intent-to-treat approach, were re-conducted using a completers-only approach. The completers-only approach used only data provided by participants who completed all four study assessments and received preventive treatment. The results of the completers-only analyses were identical to those found in the intent-to-treat approach. Accordingly, only results from the intent-to-treat approach are reported.
Changes in headache characteristics following new preventive treatments in Whites and African-Americans; no covariates

∗ P < 0.01;
∗∗ P < 0.05;
∗∗∗ P < 0.10.
Mean and standard error (shown in parentheses)
The roles of SES and psychiatric comorbidity in treatment outcome analyses
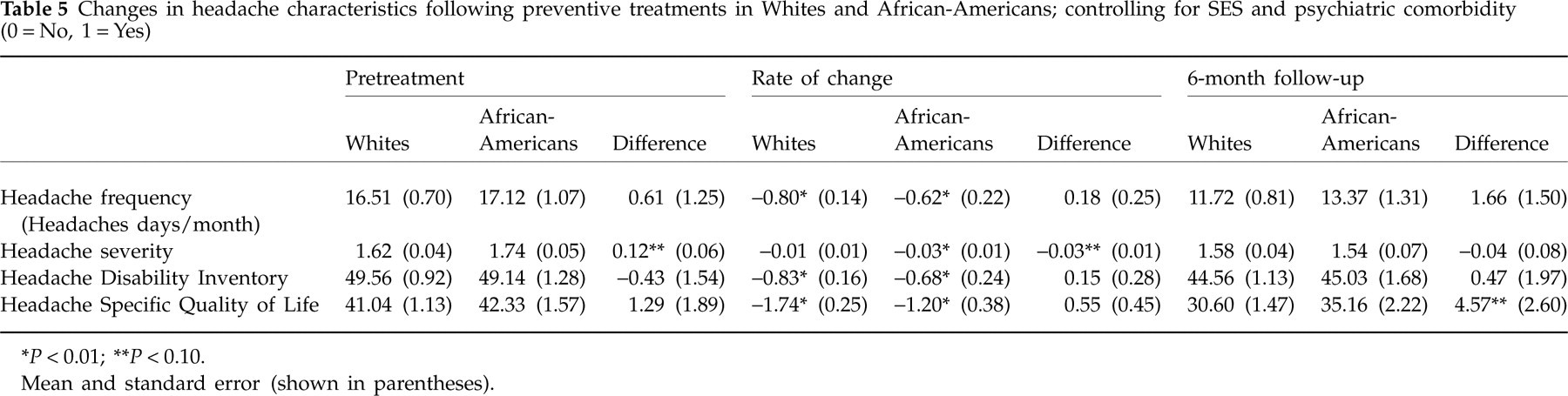
Race-related differences in health and treatment outcomes decrease considerably (and sometimes entirely) when controlling for SES (28). Furthermore, the presence of a psychiatric condition reduces the effectiveness of various treatments for pain and headache (29). Accordingly, the outcome analyses presented in Table 4 were reconducted using SES and psychiatric comorbidity as statistical covariates. As shown in Table 5, when controlling for SES and psychiatric comorbidity in intent-to-treat outcome analyses, the significant differences at pretreatment between Whites and African-Americans in headache frequency and quality of life were no longer significant, and the significant pretreatment difference in headache severity was reduced to a marginally significant difference (P < 0.10). All rates of change associated with treatment in Whites and African-Americans from pretreatment through 6-month follow-up were unchanged and remained significant (all P < 0.01). At 6-month follow-up, African-Americans and Whites reported similar levels of headache frequency, severity and disability (all P > 0.10), although African-Americans reported marginally lower headache-specific quality of life (P < 0.10). These patterns of findings suggest that, although SES and psychiatric comorbidity play significant roles in race differences on headache characteristics at pretreatment and 6-month follow-up, they are unrelated to rates of change in response to headache treatment in Whites and African-Americans.
Changes in headache characteristics following preventive treatments in Whites and African-Americans; controlling for SES and psychiatric comorbidity (0 = No, 1 = Yes)
∗ P < 0.01;
∗∗ P < 0.10.
Mean and standard error (shown in parentheses).
Discussion
This is the first prospective study designed specifically to examine race-related differences in patients receiving contemporary preventive treatments for headache disorders. Major study findings were: (i) both African-Americans and Whites reported significant improvements in headache frequency, disability and quality of life over the course of treatment, but only African-Americans evidenced reductions in headache severity; and (ii) African-Americans reported significantly more frequent and severe headaches and poorer life quality compared with Whites prior to treatment, and racial differences in frequency, disability and quality of life remained at post treatment. It is important to note, however, that many of the race differences observed at pretreatment and 6-month follow-up were no longer significant when controlling for SES and psychiatric comorbidity.
A major finding of this research was that White and African-American patients responded similarly to their headache treatments; both groups reported significant reductions in headache frequency and disability and improvements in quality of life over the 6-month follow-up period. African-Americans, unlike their White counterparts, also reported significant reductions in headache severity. These findings did not support the study's main hypothesis that Whites would respond more favourably to treatment than would African-Americans—a pattern observed across a variety of chronic health (e.g. AIDS, cancer, diabetes) and pain conditions (30). One interpretation of this finding is that if African-Americans and Whites have similar access to specialty care, both groups will respond equally well to headache treatments. The lack of race-related treatment differences may be because many factors associated with race-related treatment outcome differences in past research, such as financial barriers and delayed access to care (31), less trust in one's healthcare provider (32) and poor patient–physician communication (32–34), were less relevant for the treatments administered to patients in the current study. Specifically, all patients in the current study had severe headaches and had been referred to the specialty clinics for their headache disorders. All patients had comparable levels of access to care and health insurance and received similar types of preventive headache treatments. Finally, a very small number of physicians (n = 4) provided treatment to patients, minimizing the variability in treatment response due to different physicians. Unless there are physiological or biological reasons for Whites and African-Americans to respond differently to preventive headache treatments, the similar patterns of treatment outcomes in White and African-American patients in this study may not be surprising.
In spite of significant improvements observed in Whites and African-Americans (i.e. patients reported a reduction of approximately five headaches over the course of treatment), many participants continued to experience frequent headaches, even when controlling for SES and psychiatric comorbidity. Whites reported approximately 12 headache days per month (even after a 29% reduction from pretreatment levels), and African-Americans experienced approximately 13 headache days per month (following a 22% reduction from pretreatment levels) at the 6-month follow-up assessment. These mean values are essentially equal to the 15 headache days per month criterion used to make a diagnosis of chronic headache disorder. The reductions in headache days per month in both African-American (22%) and White (29%) patients are comparable to, albeit slightly lower than, those observed in randomized clinical and open label trials of Topiramate and Venlafaxine treatments for patients with chronic migraine and chronic tension-type headache. In these studies, patients reported headache frequency reduction rates between 30 and 50% from pre- to post-treatment (1, 5, 10, 35–39).
The differences observed in reductions in headache frequency in this study and those cited above may be explained by several factors. Clinical trials of new or modified preventive headache treatments often occur in highly controlled and ‘ideal’ treatment conditions. In such randomized controlled trials (RCTs), stringent inclusion and exclusion criteria greatly shape the nature of the sample, generous incentive payments are provided, and protocol is employed to maximize participant adherence and minimize study attrition. Very few of these practices can (or should) be implemented when evaluating headache care provided in ‘real-world’ treatment centres. For example, patients with comorbid psychological and/or substance use disorders were not excluded from the current study. Therefore, one might conclude that treatment outcomes observed in the current study are representative of headache treatments administered in real-world settings as opposed to treatment response rates that might be related to strict procedural protocols implemented in RCTs. It is important to note that many patients at the end of the 6-month follow-up period (which should have provided sufficient time for patients' headaches to respond to treatment) continued to report frequent and severe headaches, underscoring the need for even more effective treatments than those currently administered in headache specialty treatment centres.
Many significant race-related differences observed in headache characteristics at pretreatment and 6 months' follow-up diminished, or were eliminated entirely, when controlling for SES and psychiatric comorbidity. However, controlling for these two factors did not change the rates at which patients improved on key outcome measures. The tendency for SES to mitigate race-related differences in headache characteristics at these two time points was not surprising given the strong link between race and SES in the USA; race-related differences in morbidity and mortality across many health conditions often disappear when SES is used as a covariate (28). However, from a clinical perspective, it is important to acknowledge that practitioners cannot control for a patient's SES and that, at the completion of treatment, African-Americans reported lower headache-specific quality of life and slightly more frequent and disabling headaches than Whites. Accordingly, more effective preventive treatments are needed for African-American headache patients, and future research should examine why African-Americans tend to report poorer quality of life than Whites after receiving treatment and identify intervention strategies to improve life quality in this group. In terms of psychiatric comorbidity, persons with psychiatric conditions tend to report more severe and disabling headaches (29). The fact that African-Americans were more likely to be diagnosed with psychiatric conditions may explain, in part, the race-related differences in headache characteristics observed at pretreatment and 6-month follow-up and the tendency for these differences to mitigate when controlling for psychiatric comorbidity.
The current study has several limitations. All participating medical centres were located in relatively large cities in Ohio; the extent to which study findings generalize to other states and geographical areas (e.g. rural areas) is unclear. All study data (with the exception of physicians' diagnoses) were self-report in nature and susceptible to social desirability and demand characteristics. Some patients may have been managing their headaches during the study through activities such as relaxation, meditation, biofeedback and herbal therapies. These practices were not controlled for in study analyses and may have produced some of the improvements observed in key outcome measures. Approximately 40% of patients in the current study did not complete their treatments. Patients who did not complete treatment were younger, less educated, of lower SES and more likely to be African-American, reducing the generalizability of study findings to these groups. Finally, the sample was a non-probability (i.e. convenience) sample and relatively small. The extent to which this sample is representative of the population of persons seeking treatment in headache specialty treatment centres throughout the USA is unknown.
In spite of these limitations, the current study is perhaps the first investigation to test if Whites and African-Americans in headache specialty treatment clinics respond similarly to contemporary preventive headache treatments. The primary study finding was that Whites and African-Americans recorded reductions in headache frequency and reported improvements in disability and increases in quality of life after receiving preventive headache therapy, although many participants still reported > 15 headache days per month even after responding to treatment. Future research should identify more efficacious preventive treatments when administered in real-world treatment centres given the modest rates of improvements in both Whites and African-Americans. Finally, because African-Americans appear to respond favourably to preventive headache treatments, interventions are needed to better engage and retain African-Americans in treatment at headache specialty treatment centres.