
Abstract
Background
It is well recognized that underrepresented and minoritized groups do not have the same career opportunities. However, there are limited data on the range and specifics of potential barriers that withhold people in headache medicine and science from reaching their full potential. Moreover, people from different geographical regions often perceive different challenges. We aimed to identify world-wide perceived career barriers and possibilities for promoting equality amongst professionals in the headache fields.
Methods
A cross-sectional online survey was conducted among professionals in the field of headache globally. The questions of the survey were aimed at assessing perceived career barriers in four domains: professional recognition, opportunities in scientific societies, clinical practice, and salary and compensation. Perceived mentorship was also assessed.
Results
In total 580 responders completed the survey (55.3% women). Gender was the most important perceived barrier in almost all domains. Additionally, country of birth emerged as an important barrier to participation in international scientific societies. Career barriers varied across world regions.
Conclusion
It is essential that longstanding and ongoing disparities by gender and country of origin for professionals in the headache field are globally acknowledged and addressed in areas of recruitment, retention, opportunities, mentor- and sponsorships, and advancement.
Introduction
It is increasingly accepted that diversity in the workplace leads to a competitive edge (1–3), and also leads to tangible benefits including economic vibrancy (1) and innovativeness (2). This seems also true for the academic sector (3). A recent study found that research publications authored by ethnically diverse and gender-diverse groups receive significantly higher numbers of citations than papers written by researchers of a single ethnic group or the same gender (4). Unfortunately, a closer analysis of publications unveiled important inequalities. Not only are there less articles written by women as first authors and senior authors in high impact journals compared to men, but these articles also had fewer citations (5,6). While the contribution of women as first authors of original research in high impact medical journals was significantly higher than 20 years ago, it has plateaued in recent years (6).
Racial disparity is another important issue that is evident across multiple subspecialties of medicine (7). In the USA, only about 12% of the neurology workforce is made up of people from underrepresented racial and ethnic groups (Black or African American, Hispanic or Latino, American Indian or Alaska Native, Native Hawaiian and other Pacific Islanders), while women constitute about 30% of this workforce (8,9). In academics a similar gap is present (10). While efforts have been made to narrow this gap, disappointingly, over a 35-year period, women physicians in academic medical centers were less likely than men to be promoted to the rank of associate or full professor or to be appointed to department chair. Importantly, there has been no apparent narrowing of this gap over time (10). Persons of color have also been less likely than Caucasian individuals to be promoted, and women who belong to underrepresented minorities may have double barriers (10). Additionally, medical professionals in different countries perceive different challenges (11).
Participation in scientific societies and receiving grant funding are pivotal to the development, growth and success of academic careers. Historically and recently, women have been underrepresented among the American Academy of Neurology (AAN) plenary speakers (12). While the AAN has taken active steps to address equity, notable gaps remain, especially in specific prestigious plenary sessions (12). Women are also less frequently recipients of recognition awards (13,14), and women in academia are awarded less grant funding (15), which are key factors in progressing their academic careers (16). These gender gaps in grant funding are at least partially attributable to less favorable assessments of women as principal investigators, and not the quality of proposed research (17,18).
These differences can have significant repercussions for careers. Nevertheless, the global medical, scientific, and academic communities remain uninformed on the impact of barriers that prohibit full participation by women and people from underrepresented racial, ethnic, and national groups. This lack of awareness and education results in underrepresentation, under acknowledgment and failure to fully mobilize the human potential.
To promote clinical and research opportunities in the headache field based solely on abilities and to remove possible career barriers providing an unfair disadvantage, a global assessment of the problem is necessary. With this international cross-sectional survey, we aimed to define current career barriers amongst the professional headache workforce, specifically in the areas of professional recognition, opportunities in scientific societies, clinical practice, and salary and compensation. Based on the findings obtained regarding perceived barriers, we propose interventions to help strive towards equality.
Methods
Participants
An anonymous and voluntary web-based survey was distributed among people with a proven interest in headache research and clinical care. Members and associate members of the International Headache Society (IHS), delegates of the 2019 International Headache Conference and members of national headache societies affiliated with the IHS were invited to participate. To ensure that all persons working in the headache field had the chance to participate, we contacted the whole membership database of the International Headache Society and allowed national representatives to send out the survey to their members.
Survey instrument and administration
The survey instrument was developed using previously published surveys (19–21) and the experience of authors (IdB, AA, RBHS, BB, RHJ, PPR, GMT). Consensus was reached with several online rounds and emails. A questionnaire was constructed in English (see online Supplementary Materials). The survey included multiple choice items with some open-ended response options assessing demographics including age, sex, race/ethnicity (combined), country of birth, current country resident status, highest level of education achieved, current position and academic rank if applicable (see Supplementary Methods). Participants were asked about possible career barriers and mentorship opportunities. All responses were kept anonymous, and no personal identifying information was collected. The web-based survey was sent in September 2019 and closed in June 2020 with three reminders to encourage participation and were answered anonymously.
Data Analyses
Data from the questionnaires were analyzed using SPSS 25.0 (IBM Corporation, Armonk, NY). All surveys were examined for inconsistencies and invalid responses were treated as missing values. Questions with open-ended answer options were scanned to look for patterns or common answers, in the absence of these, these answer options were disregarded. Descriptive statistics (frequency counts, percentages) were used to capture demographic data for the study population, as well as perceptions of barriers. Logistic regression was performed to ascertain the effect of gender and workplace location on the likelihood of participants experiencing career barriers, corrected for age and race/ethnicity during all analyses. Results were considered significant if p < 0.05.
Results
Participants
In total 580 responders completed the survey. All responders indicated their gender (male, female or non-binary) and the women:men ratio was almost equal to 1, with 320 participants being women (55.3%). One participant identified as non-binary. As all data were analyzed and reported stratifying for gender, this participant was removed from subsequent analyses to ensure anonymity. The highest percentage of responders was from Europe (229, 39.6%), the second most represented region was South East Asia (126, 21.8%) followed by the North America (78, 13.5%). Only a minority, 23 (4.0%) and 19 (3.3%) were born in African and Eastern Mediterranean countries. In total 556 (96.0%) of the responders were healthcare providers and 480 (82.9%) participated in research activities. Moreover, 458 (79.1%) of responders participated in both clinical and research activities. Most responders were specialists working in academic hospitals. The majority of participants were in a relationship (82.7%), and had children (71.8%). Responders’ characteristics are displayed in Supplementary Tables 1 and 2.
Perceived barriers in the headache field
Many participants did encounter barriers affecting professional recognition (33.7–54.0% depending on subdomains), opportunities in scientific societies (47.0–60.8% depending on subdomains) or barriers affecting salary and compensation (39.3%) (Table 1 and Figures 1 –3). All barriers surveyed; age, country of birth, ethnicity and gender were reported. In domains reflective of professional recognition, gender was the most frequently reported barrier (13.5–27.8% depending on subdomains) (Table 1 and Figure 1). In most domains concerning opportunities in scientific societies, country of birth was the most frequently reported barrier in international scientific societies, with 42% indicating that country of birth or education is a barrier to obtaining positions in international scientific societies (Table 1 and Figure 2). For positions within national societies, gender was the most frequent barrier (27.3%), while age was the most frequent perceived barrier that caused participants not to be invited as a speaker or chair (21.9%) (Table 1 and Figure 2).
Perceived career barriers reported by all participants and by gender.

amissing n = 29 (15 men, 14 women).
bmissing n = 50 (33 men, 17 women).
cmissing n = 38 (13 men, 25 women).
dmissing n = 45 (20 men, 25 women).
emissing n = 29 (13 men, 16 women).
fmissing n = 39 (17 men, 22 women).
gmissing n = 28 (14 men, 14 women).
hmissing n = 57 (30 men, 27 women).
imissing n = 24 (10 men, 14 women).
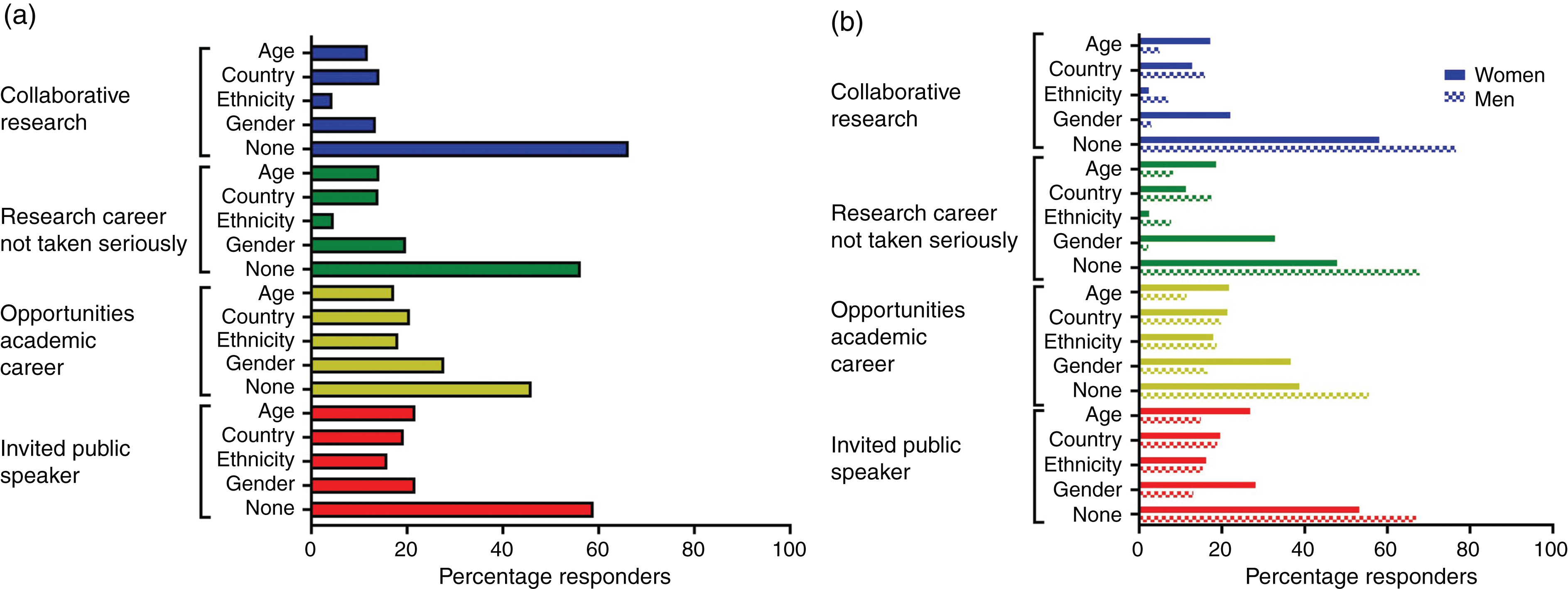
Barriers to a career in headache affecting professional recognition. Results from all participants (a) and stratified by gender (b). Country is used to indicate country of birth and/or education.

Barriers to a career in headache affecting opportunities in scientific societies. Results from all participants (a) and stratified by gender (b). Country is used to indicate country of birth and/or education.

Barriers to a career in headache affecting salary and compensation. Results from all participants (a) and stratified by gender (b). Country is used to indicate country of birth and/or education.
Perceived barriers stratified by gender
In the gender stratified analyses, it became clear that women more frequently experienced gender as a barrier (Table 2). In fact, when age, ethnicity and workplace were corrected for, women were two to three times more likely to experience barriers to professional recognition. For instance, women were three times more likely to experience barriers to collaborative research efforts (OR 3.1, 95% confidence interval (95%CI) 1.9–5.0, p < 0.001) (Table 2). While they did not indicate a different rate of participation in international conferences, women were two times more likely to experience barriers to holding a position in both national and international scientific societies (respectively OR 2.3, CI 1.5–3.5, p < 0.001 and OR 2.0, 95%CI 1.3–3.0, p = 0.002). Women in clinical practice also more frequently indicated barriers negatively influencing their interaction with patients (OR 2.8, 95%CI 1.8–4.6, p < 0.001). The perceived negative effect of gender on salary and/or grants received, as well as on compensation for work in private practices was almost exclusively reported by women (Table 1 and Figure 3). Moreover, men sometimes reported a perceived positive effect of age on salary and/or grants, this was much less often the case for women.
Likelihood of women reporting perceived barriers opposed to men.
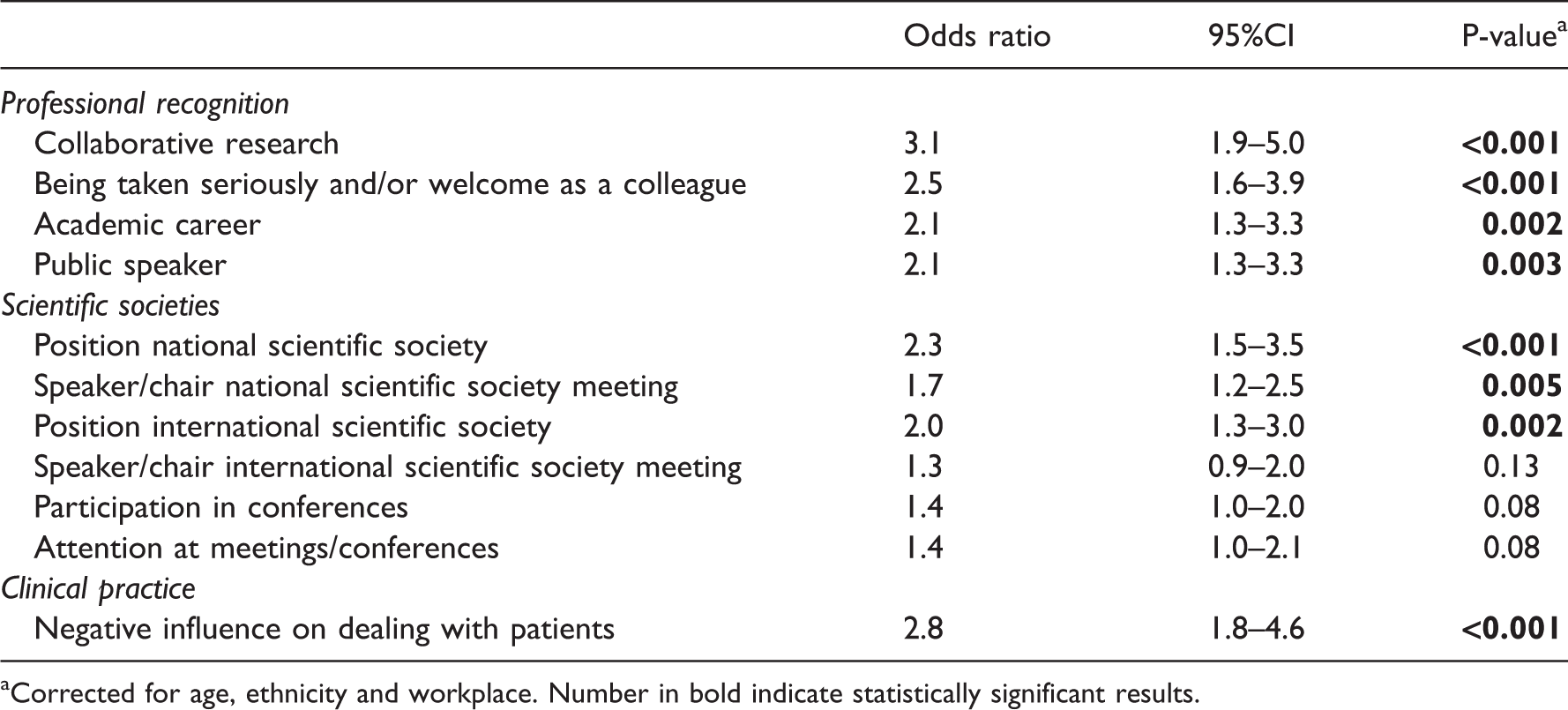
aCorrected for age, ethnicity and workplace. Number in bold indicate statistically significant results.
Perceived barriers by geographical workplace location
Unfortunately, there were not sufficient responders working in the African (3.1%) and Eastern Mediterranean (3.1%) regions to be able to evaluate specific perceived barriers among individuals from these regions. Responders’ characteristics by geographic workplace location are displayed in Supplementary Table 2. Supplementary Figures 1–3 illustrate perceived barriers to a career in headache affecting professional recognition, opportunities in scientific societies, salary and compensation by geographic workplace, respectively. These illustrate a certain degree of variability by geographical region in regard to perceived barriers assessed.
As Europe was the most common geographical work region, we examined the likelihood of non-European participants reporting perceived barriers compared to European participants. There were large differences in whether and to what extent barriers are perceived by geographical work location. For instance, North American participants had higher odds of reporting issues of colleagues not taking them seriously or being welcomed by them compared with their European counterparts (OR 2.1, 95%CI 1.0–4.1, p = 0.037) (Table 3). The opposite effect was seen in the Western Pacific region where they had lower odds of perceiving these barriers than their European counterparts (OR 0.3, 95%CI 0.1–1.0, p = 0.041) (Table 3). North Americans and persons from South America had higher odds of reporting barriers preventing participation in international scientific societies (OR 2.3, 95%CI 1.2–4.4, p < 0.015 and OR 3.1, 95%CI 1.3–7.3, p < 0.008) compared to persons from Europe (Table 3).
Likelihood of non-European participants experiencing barriers opposed to participants based in Europe.
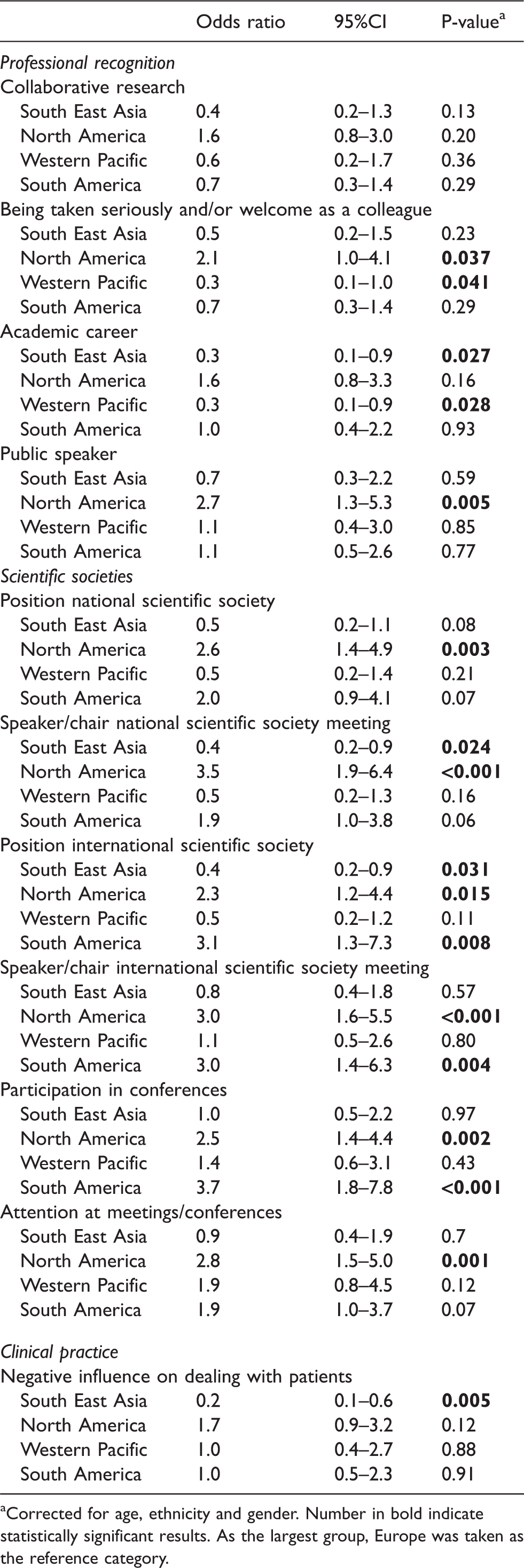
aCorrected for age, ethnicity and gender. Number in bold indicate statistically significant results. As the largest group, Europe was taken as the reference category.
Academic mentorship
The majority of participants was or had past experience as a mentee (85.1%) (Supplementary Table 4). For both men and women, most mentors were men. Many positive effects were described, such as fostering a career (85.2%) and promoting participation in external professional activities (79.3%) (Supplementary Table 4). Remarkably, around one third of participants indicated that their mentors used the mentee’s work to advance their own career (31.1%).
Discussion
Our results underline that in the field of headache care and research, women more often experience career barriers as opposed to men. Moreover, gender appears to be one of the most important barriers to a successful career in the headache field. Importantly, country of birth is also an important perceived barrier for active participation in international scientific societies. Lastly, career barriers are perceived differently across world regions. These ongoing disparities need to be acknowledged and addressed in areas of recruitment, retention, and advancement to improve the yield of the headache research field.
Gender bias (unconscious and conscious) and its associated inequity with respect to payment, leadership opportunities, promotion, and retention are universal and permeate nearly all professional and social domains. While women have closed the sex gap with respect to medical school admission in some regions, women remain underrepresented in upper faculty ranks of medical schools (10). Factors contributing to the sex gap in promotion include a persisting mentality and climate, lack of sex parity in leadership, lack of gender equity in compensation, lack of retention of women (the “leaky pipeline”), and a disproportionate burden of family responsibilities and associated difficulties in achieving work–life balance (22). However, advising women to better organize their home-responsibilities will not solve the problem of gender inequality. Importantly, perceived barriers most likely lead to fewer women entering and staying in science and medicine, despite their valuable contributions.
UNESCO Institute for Statistics fact sheet released in June 2020 showed that women in research and development represent only 23.1% of the total workforce for South and West Asia, 25% for East Asia and the Pacific region, 31.1% for Sub-Saharan Africa, 32.9% for North America and Western Europe and 39.0% for Central and Eastern Europe (23). These region-specific differences in the percentage of research scientists who are women are especially interesting considering that perceived barriers varied across regions in this study. While this could be due to local social norms and cultural influences, it might also be in part due to differences in response rate per region or potential response biases. Nonetheless, it is fair to postulate that depending on the region, different barriers to career progression might be more pressing and might require different interventions.
This study has some limitations. Firstly, given that this was a survey study, there is potential for responder bias. As we wanted to give all individuals working in the headache field the chance to participate, we contacted the whole IHS membership database and also allowed national representatives to send survey links to their members and responders to be anonymous. We contacted all IHS affiliated national societies (the full list can be accessed from the IHS website https://ihs-headache.org/en/about-ihs/affiliate-member-societies/), but we cannot know for sure which representatives actually circulated the survey, as this was voluntary. This meant that we were unable to determine the response rate. While unfortunate, we considered the need for all voices to be potentially heard more pressing. Nonetheless, a possible language barrier could have prevented some headache professionals from responding. Additionally, only 2.4% of respondents were Black or African American and 4.0% were Hispanic or Latino, which may make the results of this study less generalizable to these groups. This leads to the discussion regarding underrepresentation of some races and ethnicities in the headache field. Moreover, as very few responders were located in African and Eastern Mediterranean countries, we also had an underrepresentation of individuals from those regions. Underrepresentation based on ethnicity or geographical location led to lack of diversity in the sample. In addition, race and ethnicity were collected together rather than as separate variables, so some specificity may have been lost. We were unable to include all characteristics that could be the base of discrimination in our survey; for instance, we did not study the effect of sexual orientation and disability. Finally, it is a self-report survey of perceived barriers to career achievement. There were no outside supporting data used to substantiate respondent reports; however, the subjective nature of the data are useful to report on the perception and beliefs of the respondents.
While our findings may not be surprising regarding perceived barriers by women and people from specific global regions, it is the first time that these barriers are being surveyed in the professional field of headache care and research to our knowledge. From our findings we can conclude that there is a continuing need to monitor if enough progress is made for women and people from underrepresented global regions in (academic) headache medicine and healthcare and to improve upon the current gains in equity.
Factors contributing to these career barriers are often multidimensional with potential problems with individual, interpersonal and societal–institutional aspects. Moreover, there are often different nuances at different stages of the career path (16). There is a need for targeted interventions to counteract social stereotypes, transform “masculine” workplace cultures, end discriminatory behaviors, and promote processes to include women and other underrepresented minorities in a transparent format. The critical question is why there is a lack of retention of women and how the culture at the working place can be changed to promote women to leading positions, hence creating equal opportunities.
Climate and culture must be addressed together. Efforts to build a good climate will be unsuccessful if the policies conflict with the values of an organization (24). Thus, addressing and improving organizational culture and climate is essential to make underrepresented groups feel welcome, supported, and respected. Non-surprisingly, many advocates are tired of initiatives that focus on the actions of individuals from underrepresented groups as being the problem, and making changes to their actions being the solution. These initiatives may presume a masculine heteronormative and Caucasian homogeneous view of the world and thus automatically require underrepresented individuals to change to fit into the existing dominant system, rather than the system changing to accommodate and nurture the needs of its members. The responsibility of making a cultural shift cannot be made by the underrepresented individuals themselves as in many cases they do not have the power to affect change. Change must occur at the level of the institution, larger systems and broad shifts in cultural norms and attitudes. To achieve real inclusivity, we propose several approaches on individual, local, and (inter-) national levels (Figure 4).

Approaches to help promote inclusivity and diversity in the headache field. *Both mentors and sponsors can be crucial. Where mentors serve as guides, help solve potential issues and tell mentees that they can do the job, sponsors serve as cheerleaders and speak out about a sponsee publicly and tell others that the sponsee can do the job.
Providing a safe space for conversations about inclusivity and diversity must be a goal to improve cultures and a responsibility of leadership. Therefore, leaders at all levels should sent clear messages about the value of women and individuals from underrepresented races, ethnicity, religions, sexual orientation, gender identity and countries (25,26). Successful programs aimed at changing culture and climate require committed resources, for instance sensitivity training of hiring staff, and formal recognition that striving towards diversity is part of the goal and responsibility of leaders. There is also an important role the scientific societies should play in advocating and modeling equality. Explicit statements can change opinions and clear actions can make an even bigger impact. In addition, scientific societies should be committed to organizing inclusive conferences, not only in attendees, but also in terms of speakers, panels and organizing committees (27,28). The presenting faculty at a meeting should include individuals from underrepresented races, ethnicity, religions, sexual orientation, gender identity and countries, and be a representation of the people working in the field and members of the organization. This should also be the case for society-endorsed conferences. Hybrid conferences and scholarships with both in-person and virtual participants can be helpful to increase participation rates throughout the world, overcoming financial and geographic barriers for participation. Besides voluntary tools for organizational change, legislated approaches such as the use of quotas may also be considered. Quotas are an instrument aimed to accelerate the achievement of diversity by establishing a defined percentage of positions, which are allocated to specific groups of individuals. The concept of quotas often elicits a strong and adverse response, with claims that quality of work will be affected. While there is limited research on the usefulness of quotas, there are indications that they can have positive effects (29). While they are not the only answer, they are a tool that should be considered.
Another approach to combat career barriers is adequate mentorship. Mentoring is associated with objective and subjective measures of career success (30). Many participants already indicated that they had mentors, however women less frequently acted as mentors compared to men. Finding a mentor should not solely be the responsibility of underrepresented individuals. There also lies a responsibility for providing adequate mentors within centers and scientific societies. Our data show that in one third of cases the mentor has a mutual interest, (e.g. doing scientific or clinical work together). Another useful concept that everyone can imply is allyship or sponsorship. In allyship members of organization in a position of privilege or power seek to operate in solidarity with underrepresented groups. As an example, it could involve speaking up and supporting women and calling out discrimination. Some actual instances of sexism experienced by headache healthcare professionals and effective strategies and actions to take to support women were already suggested (31). Effective allyship requires self-awareness, commitment, respect and hard work (32,33). However, to inspire cultural change a combination of interventions will likely be necessary (26,34).
Striving towards an inclusive climate should be a continuous process, not a final destination. Setting and measuring predetermined milestones is important, but any organization should strive to always be diverse and inclusive. Now that we know which barriers are being perceived by healthcare professionals, academics and scientists in the headache field, we can start working together towards establishing an ever more inclusive, nurturing and welcoming domain.
Article highlights
Gender is an important barrier to career achievements in the headache field. Specific perceived career barriers are different across world regions. Country of birth is a barrier for participation in international scientific societies. (Inter-)national headache organizations should be aware of these barriers and ensure an equal position for all members independent of gender, ethnicity, geographical location or other personal characteristics.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024221123081 - Supplemental material for Perceived barriers to career progression in the headache field: A global web-based cross-sectional survey
Supplemental material, sj-pdf-1-cep-10.1177_03331024221123081 for Perceived barriers to career progression in the headache field: A global web-based cross-sectional survey by Irene de Boer, Anna Ambrosini, Rashmi B Halker Singh, Betül Baykan, Dawn C Buse, Cristina Tassoreli, Rigmor H Jensen, Patricia Pozo-Rosich and Gisela M Terwindt in Cephalalgia
Footnotes
Acknowledgements
We kindly thank Carol Taylor for her assistance in distributing the survey.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
IdB reports independent support from the International Retinal Research Foundation and Dutch Heart Foundation. AA reports consultancy or industry support from Novartis, Eli-Lilly and Teva. RBHS reports a research grant from Amgen. BB has nothing to disclose. DCB has received research funding from the US Food and Drug Administration, the National Headache Foundation and Amgen. She has also received consulting fees from Amgen, Allergan/Abbvie, Lilly, Lundbeck and Teva. CT has received honoraria as a consultant and speaker for Amgen, Allergan/AbbVie, Almirall, Biohaven, Eli Lilly, Lundbeck, Medscape, Novartis and Teva Pharmaceuticals. Her research group has received research grants from Allergan/AbbVie, EraNet Neuron, Italia Ministry of Health. Her Institution has received payment for clinical trials from AbbVie, Eli Lilly, Lundbeck, Novartis and Teva Pharmaceuticals. RHJ has given lectures for Pfizer, Eli-Lilly, Merck, TEVA, Novartis, Lundbeck and Allergan, is investigator in clinical trials with Eli-Lilly, Novartis and Lundbeck, is director of Danish Headache Center, Lifting The Global Burden of Headache and Founder of Master of Headache Disorders at University of Copenhagen and has received research funding from University of Copenhagen, Rigshospitalet, Lundbeck Foundation, The Medical Society in Copenhagen, NovoNordisk Foundation and Tryg Foundation. PPR has received honoraria as a consultant and speaker for Amgen, Allergan/AbbVie, Almirall, Biohaven, Chiesi, Eli Lilly, Lundbeck, Medscape, Neurodiem, Novartis and Teva Pharmaceuticals. Her research group has received research grants from Allergan/AbbVie, AGAUR, la Caixa foundation, EraNet Neuron, Instituto Investigación Carlos III, MICINN, Novartis, PERIS, RIS3CAT, Teva Pharmaceuticals; and has received funding for clinical trials from AbbVie, Biohaven, Electrocore, Eli Lilly, Lundbeck, Novartis and Teva Pharmaceuticals. GMT reports independent support from the Dutch Research Council, and the Dutch Hearth and Brain Foundations, Dioraphte and IRRF, she reports consultancy or industry support from Novartis, Lilly and Teva, Allergan (Abbvie), Lundbeck.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a granted project proposal by the International Headache Society.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.