
Abstract
Background
There is lack of data on opioid (over)use for migraine in Europe.
Methods
We performed a cross-sectional study in a large Dutch cohort using a web-based questionnaire to assess opioid use in individuals with migraine. Primary outcome was to assess opioid use for the treatment of migraine attacks. As secondary outcomes we specified use of opioids (duration of use, type of opioids, prescriber) and compared between persons with episodic migraine versus chronic migraine. Descriptive statistics, unpaired T-tests, Chi-square and Mann-Whitney U tests were used.
Results
In total n = 3712 patients participated, 13% ever used opioids for headache. In opioid users, 27% did this for >1 month, and 11% for >1 year, and 2% without prescription. The majority of prescribing physicians were general practitioners (46%), followed by neurologists (35%), other specialists (9%), or emergency room doctors (8%). Opioids were used as acute treatment in 63%, in 16% as preventive treatment, and in 21% for both indications. Chronic migraine patients reported more opioid use compared with episodic migraine (22% versus 12%, p < 0.001), with also more prolonged use (>1 month: 34% chronic migraine versus 24% episodic migraine, p < 0.003).
Conclusion
Opioid use is more frequent and prolonged in chronic migraine patients. Further education for both doctors and migraine subjects and providing multimodal pain management strategies are needed to reduce opioid use in persons with migraine.
Introduction
Migraine attacks can be episodic (episodic migraine, EM), but when high in frequency are referred to as chronic migraine (CM). CM is described as headache occurring on ≥15 days per month for more than three months, which on ≥8 days per month has the features of migraine headache (1). Chronic migraine is a highly disabling and difficult to treat affecting nearly 2% of the general population (2). Medication overuse is a major risk factor for transformation from episodic (<15 headache days) to chronic migraine and an important factor in maintaining and aggravating chronification. The majority of individuals with chronic migraine overuses acute headache medication leading to further sensitization of the brain (3,4).
Migraine-related emergency department visits are common. In the United States alone, 1.5 million visits to emergency departments for migraines were made in 2008 (5). Emergency departments handle almost 20% of all migraine care compared to other clinical settings (6). Visiting patients are looking for an acute reduction in pain. According to (inter)national migraine treatment guidelines, effective medication should include at least non-steroidal anti-inflammatory drugs (NSAIDs), antiemetics, or triptans (7–9). Even though this wide range of effective therapeutic options are available, data suggests that doctors still tend to prescribe opioids, and in many national guidelines it is still mentioned as a possible treatment choice (10). Numbers derived from the National Hospital Ambulatory Medical Care survey showed that in almost half of acute migraine visits at emergency departments in the United States, migraine sufferers received opioids (11–13). This suggests that the debate on proper treatment for acute, severe and ongoing migraine attacks is still needed (14,15).
The high numbers of opioids prescriptions for migraine in the United States, but likely also in other countries, is cause for concern. First, because opioids for the acute treatment of migraine are less effective than specific acute migraine-specific treatments such as the triptans (16). Opioid use is associated with an increased risk of medication discontinuation compared to triptans (17). Reasons for medication discontinuation included return of migraine pain, concerns regarding drug interactions, and stomach upset, among others (18). More importantly, (excessive) use of opioids has been correlated to a dose-dependent increase in the risk of progression to chronic migraine (11,19). Since current available numbers for opioid use in migraine primarily reflect the US population and these specific statistics are not available for European migraine subjects, we aimed to set up a cross-sectional study to investigate the use of opioids among episodic (EM) and chronic migraine (CM) individuals within a large Dutch migraine cohort.
Methods
Study design and participants
We performed a cross-sectional questionnaire study among subjects with migraine. Data were collected between October and December 2021. Participants were selected from the Leiden Headache Center migraine cohort (20,21). Migraine (episodic and chronic) fulfilled the International Classification of Headache Disorders (ICHD-3) criteria (1).
Leiden Headache cohort
Migraine subjects (aged 18–80 years) were previously recruited via nationwide public announcement, advertising in lay press and our research website. They were considered eligible after a two-step inclusion process using validated questionnaires. Additionally, persons attending the Leiden Headache Clinic were invited to participate. All participants were first asked to fill out our validated web-based screening E-questionnaire (sensitivity of 0.93 and specificity of 0.36 for migraine) (22,23). Subjects who fulfilled the screening criteria for migraine received a validated web-based extended migraine e-questionnaire, based on the International Classification of Headache Disorders criteria (ICHD-3 version) (1). The specificity of the extended migraine E-questionnaire was 0.95 and sensitivity was 0.45 (20). These E-questionnaires are described in detail elsewhere (20).
We consider the cohort a well-defined web-based cohort, as only between 4–20% of migraine individuals are included from our Leiden Headache Clinic, and 87% of the participants are previously diagnosed with migraine by a physician. In addition to questions that are necessary to diagnose migraine accurately, the extended E-questionnaires also includes items on demographic factors, aura and headache characteristics, and acute and prophylactic headache medication use. Participants unable to use the web-based E-questionnaires were allowed to complete the questionnaires on paper.
E-questionnaire
All subjects of our Leiden Migraine cohort were invited to complete an online E-questionnaire with general additional questions on current migraine characteristics and medication, and questions to assess current and past opioid use. The following opioids and the corresponding dosages were specified: buprenorphine (5–15 microg/h), fentanyl (25–50 microg/h or 50–400 microg), hydromorphone (1.3 mg), morphine (5 mg/ml or 10–200 mg), oxycodone (5–120 mg), tapentadol (50–100 mg), tramadol (50–300 mg), and an option for non-specified subcutaneous injection in case the patient did not know the name of the opioid. Codeine was not included in this list, since this therapeutic agent is not prescribed for migraine in the Netherlands. The time period for the use of an opioid was categorized into the answer options; once, shorter than one week, between one week and one month, more than one month, more than six months or more than one year. Further questions were included to assess who prescribed the opioid (emergency department, local health center, general practitioner, neurologist, other specialist or self-acquired) as well as the therapeutic indication of treatment (for an acute attack, as preventive treatment or combination of both).
Statistical analyses
Unpaired T-test for quantitative variables, Chi-square for categorical variables, and Mann-Whitney U test for ranked variables, were used to analyse the opioid use among migraine participants. Primarily, the percentage of subjects who used an opioid in the past, present and ever were calculated and further specified per opioid as the percentage of individuals who used an opioid at some point in time.
Additionally, analyses were performed for episodic (EM) versus chronic migraine (CM), separately. Chronic migraine was defined as an average of ≥15 headache days per month during the past three months, from which ≥8 days fulfil criteria for a migraine attack according to ICHD-3 (1). Furthermore, we looked at monthly acute medication use days (MAMD). We defined medication overuse headache (MOH) according to the ICHD-3 as the regular use of acute headache medication on at least 15 days per month in the case of simple analgesics or at least 10 days per month in the case of triptans, ergotamine, combination analgesics, opioids, or a combination of medication classes for >3 months (1).
We assessed factors associated with opioid use and conducted a logistic regression analysis. Our predictors included age, sex, current triptan use, chronic migraine, health care provider visited for migraine (i.e., none or general practitioner versus one or multiple neurologist(s)).
Two-sided p-values <0.05 were considered statistically significant. Due to a clear distinction between primary and secondary analyses, no corrections for multiple testing were made (24). All analyses were performed in R version 3.6.1.
Standard protocol approvals, registration and patient consents
This study was approved by the medical research ethics committee of Leiden University Medical Center. All subjects provided written informed consent.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Results
We sent an invitation to participate in this specific study to n = 6577 migraine patients, of whom n = 4047 responded and n = 3712 completed the questionnaire (response rate 56.4%) (Flow Chart, Figure 1). Subjects of this study were previously identified via our website (79.4%) and via the Leiden Headache Clinic (20.6%). Baseline characteristics are shown in Table 1. The responder group contained more men compared with the non-responder group (16.0% vs. 13.8%, p = 0.014) and the responders were older than the non-responders (mean age 52 vs. 48 years, p < 0.001). Participants with episodic migraine (EM) and those with chronic migraine (CM) were comparable regarding age and sex (p = 0.83 and p = 0.26). The subtype migraine with aura occurred more among participants with EM than those with CM (27.2% vs. 36.5%; p < 0.001). As expected, subjects with Chronic Migraine (CM) were more likely to suffer from Medication Overuse Headache (MOH) than subjects with EM (58.7% vs. 15.9%; p < 0.001). The mean number (±SD) of Monthly Migraine Days (MMD) was higher in CM 15.4 ± 5.6 versus 4.0 ± 3.2 for EM (p < 0.001), as was the mean number (±SD) of Monthly Acute Medication Days (MAMD) in CM 8.2 ± 8.1 versus 3.5 ± 5.0 EM (p < 0.001).
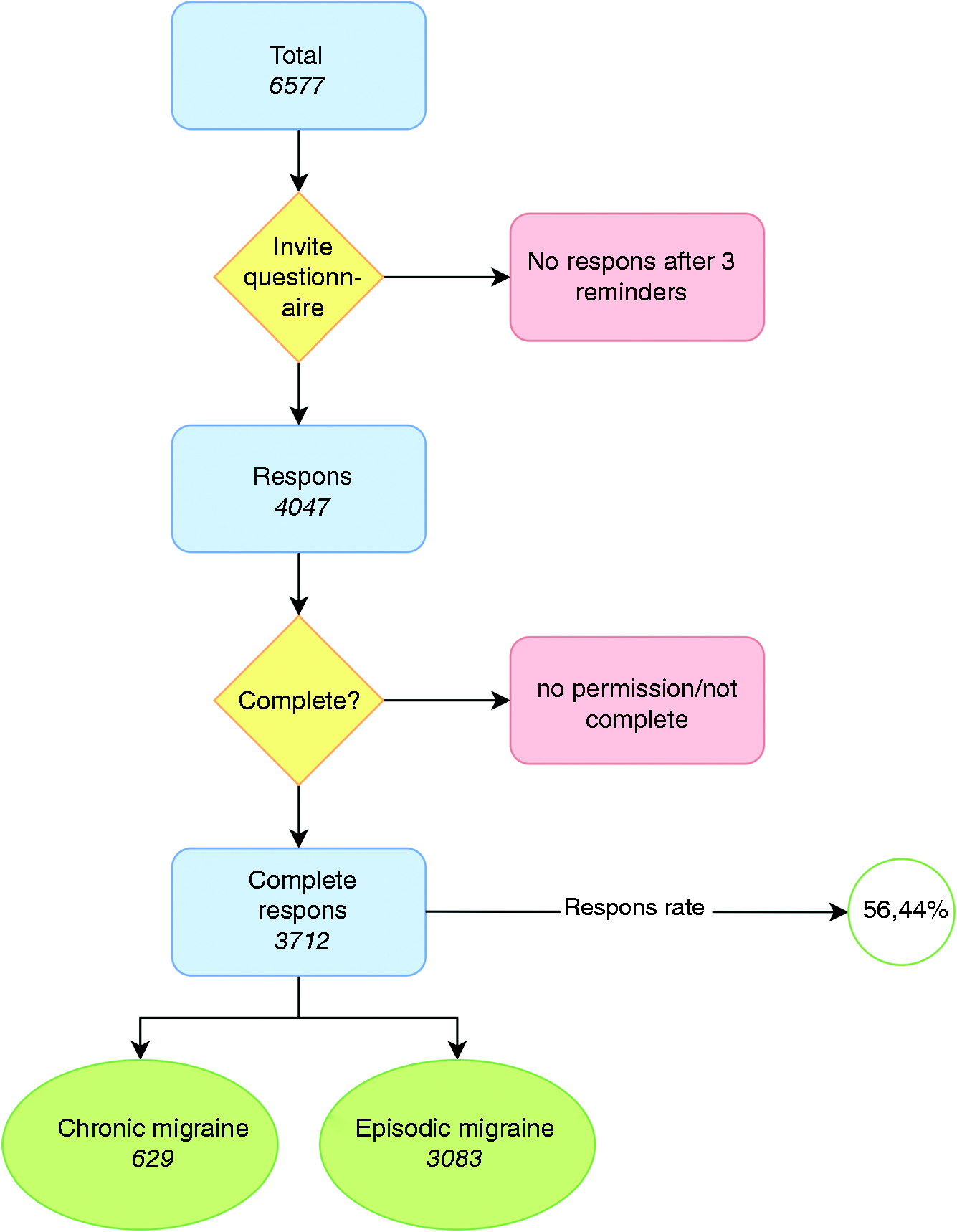
Flow chart of the study.
Baseline characteristic of the included subjects.

CM, Chronic Migraine; EM, Episodic Migraine; MOH, Medication Overuse Headache; MAMD, Monthly Acute Medication Days; MMD, Monthly Migraine Days.
Monthly Acute Medication Days are self-reported, and self-reported Analgesic/Triptan/Ergotamine days.
For our MOH definition we took the overall MAMD instead of the separate reported acute-medication days. Some patients may have unreported the total number of MAMD compared to the separate days.
Primary analysis
In total 497 (13.4%) participants reported ever having used an opioid for their headaches (Table 2). The reported current use of an opioid for headache among all participants was 65 (1.8%) and previous use of an opioid for their headache 463 (12.5%). In addition, 953 (25.7%) participants reported to have (ever) used an opioid for a therapeutic indication other than headache (Table 2).
a. Opioid use present and past for migraine. b. Opioid used, but not for headache.
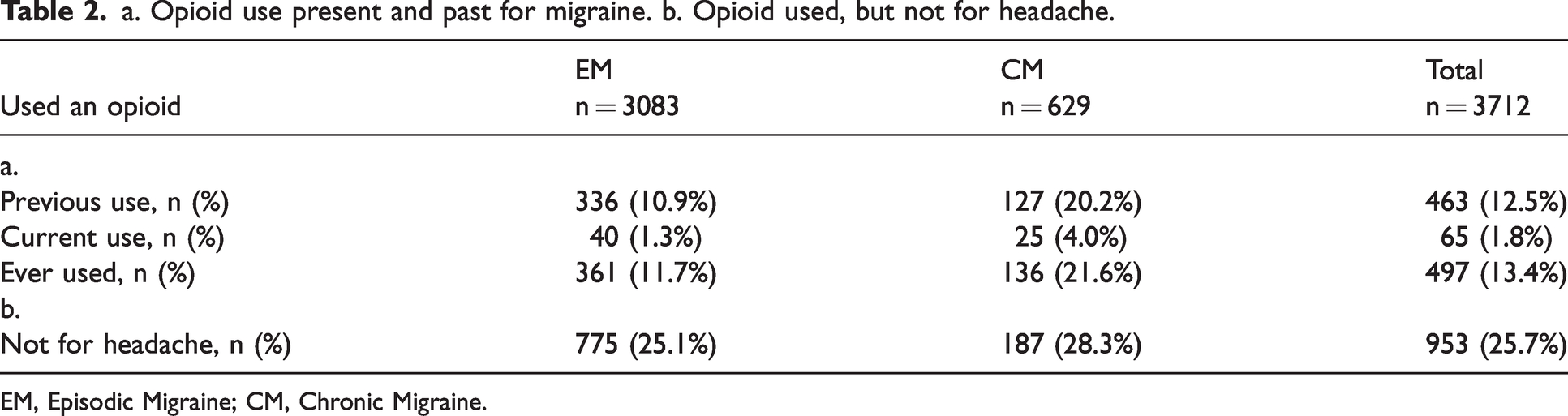
EM, Episodic Migraine; CM, Chronic Migraine.
Secondary analyses
The four most frequently used types of opioids that were reported by the participants were (see Table 3 for all); tramadol (58.0%), oxycodone (20.5%), morphine (19.5%), fentanyl (17.3%). A large group of migraine participants (46.3%) only used an opioid occasionally (one time), but in 27.0% of cases this was for longer than one month, and for 11.3% of subjects longer than one year (Table 4 and Figure 2).
Opioid use specified for the opioid types, use at any point in time, number of patients.

EM, Episodic Migraine; CM, Chronic Migraine.
Notably, participants could indicatie use of more than one opioid.
Duration of opioid use.

EM, Episodic Migraine; CM, Chronic Migraine.
Notably, time periods are shown as exclusive groups.

Duration of opioid use presented as percentage for all opioid use.
The reported prescriber and reason for opioid use is shown in Table 5 and Figure 3. Opioids were mostly prescribed by physicians, but 2.4% of opioid-users indicated that they used an opioid without a prescription. The major group of prescribing physicians were general practitioners (45.8%), followed by neurologists (34.7%), other specialists (9.4%), and a physician at first aid (local health center or emergency department) (7.6%). Opioids were reported to be prescribed as acute treatment in 62.7% of cases, in 15.9% as preventive treatment and in 21.5% as both acute and preventive medication.
Prescription of opioid(s), by prescriber type (a) and indication (acute, preventive, both) (b).

EM, Episodic Migraine; CM, Chronic Migraine.

Prescription of opioid(s), by (a) prescriber type, and (b) indication (acute, preventive, both).
For tramadol, oxycodon, morphine a total of ≥45% responders could indicate which dosage was provided. For the other opioids the response rate of participants who knew the dosage of the medication was too low to further analyse the data. For tramadol the majority (87.1%) used 50–100 mg, for oxycodon the majority (82.5%) used 5–20 mg, and for morphine 89.8% used 5–50 mg.
Chronic migraine versus episodic migraine
Opioid use was more frequent in individuals with CM compared with EM (21.6% vs. 11.7%, p < 0.001) (Table 2). The reported types of opioid use were different between EM and CM tramadol, morphine, oxycodone and non-specified opioids (all p-values <0.05). Especially tramadol was used more often among participants with CM than those with EM (64.0% vs. 24.1%, p < 0.001). The duration of opioid use was more often prolonged in those with CM versus EM (>1 month: 33.6% vs. 24.4%, p < 0.003; >1 year: 17.7% vs. 8.7%, p < 0.001). Subjects with CM reported more self-required use of opioids compared with EM (4.8% vs. 1.2%, p = 0.015). CM participants more often received opioids at a local health center (3.0% vs. 7.1%, p = 0.035). CM received less prescriptions by general practitioners than EM (35.7% vs. 50.9%, p = 0.035).
Triptan users versus non-triptan users
We performed a simple analysis of the current use of opioids in patients currently taking triptans (38/2396, 1.59%) versus those without current use of triptans (27/1316, 2.05%) and found no significant difference (Chi-square p = 0.60).
Logistic regression analysis
Logistic regression analysis showed that male sex (β = 0.30, p < 0.02), chronic migraine (β = 0.68, p < 0.0001) and consultation of neurologist(s) (β = 0.83, p < 0.0001) were associated with opioid use, whereas age and current triptan use were not.
Discussion
In this large cross-sectional study, 13% of participants with migraine reported to ever have used opioids for headache. In 27% of opioid users this was for more than one month, and 11% reported use for more than one year. Remarkably, 2.4% had used opioids without a prescription. Opioid use was more frequent and more prolonged in those with chronic migraine (CM) compared with episodic migraine (EM). Our study shows that patients with migraine receive opioids by physicians although opioids are shown to be ineffective in this primary headache disorder.
In addition, our study shows that opioids are prescribed mostly as treatment for acute migraine attacks, by a variety of physicians and also in an emergency setting where migraine subjects seek acute help for their headaches. Previous studies have concluded that prescribing opioids for migraine attacks in an emergency setting in the United States is common (25). While a cross-sectional study in the US showed that opioid use decreased from 2007 to 2018 among headache-related ER visits, it is still high (up to 28%) (25). The frequency of opioid prescription for nontraumatic headache in the emergency department and at hospital discharge varies internationally, but there are hardly any data on the situation in Europe (26,27) Severe headache, prehospital opioid use, and long-term opioid use predicts opioid administration at the emergency department. Opioid administration at the emergency department is also a strong predictor of opioid prescription at discharge (26). There is still major concern towards an underutilization of triptans and overutilization of opioids, and there is still a non-adherence to hospital or evidence-based established international guidelines (28).
The American CaMEO study reported 36.3% opioid use among people with migraine treated with acute prescription medications (29). In our study only 1.8% of all migraine participants reported current use of an opioid for headache. A direct comparison with the CaMEO study is not possible as the CaMEO has a different methodology for collection of the data and a different cohort. The CaMEO study defined current opioid users as individuals who use opioid or keep opioids on hand to treat headache. Also, the CaMEO study did not report the past use of opioid use. Additionally, the results are not directly comparable because the CaMEO study population consisted of current users of prescription medication for migraine whereas our study population consist of patients with a current or past migraine diagnosis. Similar to the CaMEO study, we assessed factors associated with opioid use and showed that male sex and chronic migraine were associated with opioid use, whereas age and current triptan use were not. Although our descriptive analysis showed that GPs are more likely to prescribe opioids, our regression model demonstrated that patients who consulted one or more neurologists used opioids more often. A possible explanation for this finding is that more severely affected patients (for example patients with chronic migraine) are more likely to have been prescribed opioids before being referred to a specialist.
A possible reason for the difference in current opioid use between an US population and a European population can be found in the guidelines for treating migraine. The guidelines in Europe for migraine treatment according the Consensus Statement endorsed by the European Headache Federation (EHF) and the European Academy of Neurology (EAN) warn that opioids as a medication should be avoided (28). This is because the efficacy of opioids is questionable and associated with adverse effects and risk of dependency (28). The guidelines in the US for migraine treatment regarding opioids according to the American Academy of Neurology (AAN) state that opioid treatment can be used as a rescue therapy when migraine-specific treatments fail (11). The AAN guideline recommends that opioid use should be limited to ≤9 days per month to avoid medication overuse headache (MOH) with long-term follow-up to prevent treatment complications (11).
Our study evaluated the usage of different types of opioids among migraine individuals. The most common method to compare the pharmacological potencies among different opioid types is by comparing them to morphine as standard. Tramadol and tapentadol have a lower potency than morphine (respectively 1/10 and 1/3) (30,31). The other opioid types have a relative higher potency comparted to morphine; oxycodone (1.5), hydromorphone (4–5), buprenorphine (80–100), and fentanyl (100) (31). The most commonly used opioid among the participants was the relatively weak potent opioid tramadol (58.0%). Low-potency opioids have been associated with a lower overdose risk compared to high potency synthetic opioids (32). However, pharmacological potency alone does not entail more effective analgesia or higher risk of abuse, but it also depends on the administered dosage and subject characteristics (33).
A major cause for concern is the relatively large group of patients who use opioids on more than one occasion, at times for over a year. Our study shows that opioids are not only used by migraine sufferers as treatment for acute migraine attacks, but additionally or even exclusively as prophylaxis. Use of opioids increases the risk of MOH and CM (11,19,27,34). Epidemiological data suggest that overuse of analgesics and other pain medication is common, as approximately 1–2% of the general population suffers from MOH (4). Medication overuse is a major risk factor for transformation from EM to CM (35–37). In our study, opioids were prescribed as acute treatment in the majority of cases, but 37% of those who used opioids indicated it was also, or even strictly, used as preventive treatment. This seems to show that at least these subjects were not (fully) aware of the risk for chronification of migraine and this deserves further study.
Patients with CM with MOH in whom preventive treatment is not effective, are recommended to start drug withdrawal (38). Drug intake can be abruptly terminated or restricted in patients overusing analgesics or triptans. In patients with long-lasting abuse of opioids, barbiturates or tranquilizers, slow tapering of these drugs is recommended (4). Currently, there is debate whether adding novel preventive medication such as calcitonin gene-related peptide (CGRP)-blockers might be useful to ensure that patients are successful at drug withdrawal (39). Behavioural intervention by a headache nurse during withdrawal therapy for MOH has been demonstrated to be beneficial in a recent concealed double-blind randomized controlled trial (37).
Although MOH is well-described as a clinical condition and the link between frequent acute medication intake and increasing headache frequency is well established, its pathophysiology is not completely understood (4,40,41). The potential pathophysiological mechanisms of MOH involve potential genetic factors, peripheral and central mechanisms, and altered descending pain modulation. Overuse of acute headache medication alters the function of the central 5-HT dependent descending modulating system (42–45). This can result in an increase in neuronal excitability in peripheral and central nervous system structures resulting in headache, hyperalgesia, and allodynia. Increased cortical excitability lowers the threshold for the development of cortical spreading depolarization (46). Upregulation of CGRP involved pathways may contribute to the chronicity of headache. Pretreatment with fremanezumab, a monoclonal anti-CGRP antibody, blocked pain-like behaviors in opioid sensitized rats (47).
The strength of our current study is that we examined self-reported opioid use with an E-questionnaire sent to a well-defined migraine cohort. Although there is some risk of recall bias, as participants were also asked about past use of opioids, this will likely lead to an underreporting. Effectively, the proportion of opioid users among migraine patients might be higher. A weakness of the study may be that not all participants were able to report on the dosages of the opioids. However, for tramadol, oxycodon, and morphine the dosages were reported by a large group of participants and the vast majority used a recommended acute treatment dose or daily dose. So, dosage overuse does not seem to be a major issue. Participants also reported on the therapeutic indication: for acute treatment, for prevention of attacks, or for combination of both. Although this use might not reflect the intention of the prescriber, it does reflect how the participants used the medication in practice. It is known that patients do not always adhere to instructions that are provided by the prescriber. Moreover, our study also showed that 2.4% used opioids without prescription. Furthermore, when patients indicate using opioids as preventive medication they may use it similar to preventive medications such as beta-blockers, or patients may take opioids anticipating upcoming attacks. The latter may be indicative for (future) dependence of opioids.
Conclusion
Despite the fact that opioids are considered not effective and are not recommended in our national treatment guideline, these medications are still prescribed, up to 11% for more than one year, and up to 22% in those who suffer from chronic migraine. Remarkably, 2.4% of opioid-users did so without a doctor’s prescription. Of all users 37% used opioids (also) for preventive reasons. Further education for both doctors and migraine subjects as well as providing multimodal pain management strategies are needed to reduce opioid use in persons with migraine.
Clinical implications
Despite the fact that opioids are considered not effective and not recommended in our national treatment guideline these medications are still prescribed, even up to 22% in those who suffer from chronic migraine, and up to 11% for more than one year. Of all opioid-users 2.4% did so without prescription. Of all users 37% used opioids (also) for preventive reasons. There is a non-adherence to evidence-based established international guidelines. Further education for both doctors and migraine patients as well as providing multimodal pain management strategies are needed to reduce opioid use in persons with migraine.
Footnotes
Authors’ contributions
RFvW: Design and conceptualized study; major role in the acquisition of data; analysed the data; interpreted the data; drafted the manuscript for intellectual content.
FcvW: Design and conceptualized study; major role in the acquisition of data; analysed the data; interpreted the data; drafted the manuscript for intellectual content.
SdVL: Design and conceptualized study; major role in the acquisition of data; interpreted the data; revised the manuscript for intellectual content.
AD: Revised the manuscript for intellectual content.
MvV: Design and conceptualized study; interpreted the data; revised the manuscript for intellectual content.
GMT: Design and conceptualized study; interpreted the data; revised the manuscript for intellectual content.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GMT reports consultancy support from Novartis, Allergan, Lilly, and Teva, and independent support from Dutch Organization for Scientific Research, the Dutch Heart & Brain Foundations, IRRF and Dioraphte.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.