
Abstract
Despite an extensive body of research on the individual burden of migraine, few studies have examined its impact on the family. We aimed to assess the impact of migraine on family life both from the perspective of those with migraine and from the perspective of their partners. A validated computer-assisted telephone interview (CATI) identified 574 people with migraine from a population sample of 4007 in mainland England, and 568 from 4376 in Philadelphia County, in the USA. Migraine cases with six or more migraine attacks per year and living as married with partners were asked, along with their partners, to participate in this study. In a follow-up interview, questions were asked of the proband (i.e. subject identified with migraine in the survey) about the impact of migraine. Similar questions were also asked of the probands' partners regarding the impact of the proband's migraine on their participation in social, family and leisure activities and on family relationships. The samples from the two countries showed similar characteristics, and were combined. Of 389 people with migraine living with a household partner, 85% reported substantial reductions in their ability to do household work and chores, 45% missed family social and leisure activities, and 32% avoided making plans for fear of cancellation due to headaches. One half believed that, because of their migraine, they were more likely to argue with their partners (50%) and children (52%), while majorities (52-73%) reported other adverse consequences for their relationships with their partner and children, and at work. A third (36%) believed they would be better partners but for their headaches. Participating partners (n = 100) partly confirmed these findings: 29% felt that arguments were more common because of headaches and 20-60% reported other negative effects on relationships at home. Compared with subjects who did not have migraine regarding their work performance, a statistically significantly higher proportion of migraine partners were unsatisfied with work demands placed on them (P = 0.02), with their level or responsibilities and duties (P = 0.02), and with their ability to perform (P = 0.001). Results from this study show that the impact of migraine extends to household partners and other family members.
Introduction
Migraine is a common chronic recurrent neurological disorder characterized by attacks of pain, associated symptoms and temporary disability (1). Numerous studies have demonstrated that migraine is an important cause of absenteeism, reduced productivity while at work and diminished health-related quality of life (2–11). Some studies have shown that migraine influences health status and behaviour between as well as during attacks (2, 3).
Because migraine affects women more often than men (gender ratio 3 : 1) (12), and is most common between the ages of 25 and 55 (12), the years of child rearing, a substantial impact on family life might be expected. However, of the many studies focusing on the burdens of migraine, relatively few have examined its impact on the families of those directly affected. A Canadian study reported that 90% of people with migraine reported postponing their household work because of headaches, 30% had cancelled family and social activities during their last migraine attack, and two-thirds feared letting others down because of their headaches (13). Other studies (14–17) found that migraine attacks brought significant disruption to family life, with impact on spouses, children and friends.
In this report, we extended previous work by conducting simultaneous, methodologically similar population-based studies in the USA and the UK. We interviewed people with migraine as well as their partners to assess the impact of migraine on their family lives and relationships.
Methods
Parallel epidemiological studies were conducted in the UK and the USA using similar methods (5, 18); interviews were identical except for minor differences in word choice which took into account linguistic differences between the two countries. Each study was conducted in three phases. First, migraine cases were identified from general population samples with a validated computer-assisted telephone interview (CATI) where identification of those with migraine was based on International Headache Society (IHS) diagnostic criteria (1). In the second phase, those with six or more migraine headaches per year were interviewed further about their health care utilization and medication use. Third, those who completed the second phase and were living as married with household partners were asked, along with their partners, about the impact of the proband's (the subject who brings the family to attention) migraine on the family. The methods are described in brief below and in more detail elsewhere (5, 18), along with the results from the first two phases.
Sampling frame
A systematic sample of households from the mainland of England was obtained from the UK electoral register by Sample Answers Ltd, a UK-based geodemographic company using procedures detailed elsewhere (18). In the US survey, a sample of households in Philadelphia County, Pennsylvania was identified using random-digit dialling methods described elsewhere (5). Eligible respondents from these households conversed easily in English, ranged in age from 16 to 65 years in the UK and from 18 to 65 years in the USA, and permanently resided in the contacted household. From households with multiple eligible members, a respondent was selected at random for inclusion in the final data set.
Screening interview
The CATI has been extensively used and validated in independent studies in the UK (18) and the USA (5). Against diagnoses made by clinicians applying IHS criteria, the CATI has been shown to have high sensitivity (UK 91%, USA 85%) and specificity (UK 97%, USA 96%) for diagnosing migraine with or without aura.
Subjects were first asked if they had at least one headache not due to head injury, hangover, or an illness such as cold or flu in the past year. For affirmative answers, the number of different types of headache was ascertained. Detailed questions were asked about the most severe type of headache occurring in the previous 12 months (i.e. most interfered with work, study or chores), based on the demonstration that if the subject had migraine, the most bothersome headaches were very likely to be migraine (19). If it became clear that the interviewee did not have migraine, the interview was terminated. Specific questions were asked about age at onset, headache frequency and duration (unmedicated), pain intensity and disability (e.g. missed work, interference with daily activities and need for bed rest) and headache features (i.e. location and quality of pain, effect on headaches of physical activity, and the occurrence of nausea, vomiting, photophobia, phonophobia and visual or sensorimotor aura). Whenever a feature was reported, questions were asked about frequency (never, rarely, less than half the time, half the time or more) of occurrence with attacks. When nausea, photophobia or phonophobia were reported, follow-up questions were asked about severity (mild, moderate or severe).
Family impact interview
Eligible migraine sufferers who completed earlier phases of the study and who were living as married with a partner were also asked about the impact of their migraine on their family. Cohabiting couples not legally married were included. Single parents were excluded. In the USA, migraine sufferers and their partners were invited by telephone. In the UK, interviews were conducted in person using methods detailed elsewhere (18). The interview covered five main areas: (i) demographic characterization; (ii) impact of migraine on participation in housework and recreation; (iii) impact of migraine on relationships and communication with children; (iv) impact of headache on relationships and communication with household partner; (v) impact of migraine on work performance and satisfaction with work. In each of these domains, the impact of migraine was subjectively rated from 0 (no impact) to 10 (most severe impact). Partners answered a similar questionnaire regarding the impact of the proband's migraine on the proband participation in housework and recreation, on their relationship with their household partner, and on work or study performance.
Selection of a control group
Similar to migraine cases and their partners, a control group was invited to participant in an in-depth interview that paralleled the interviews for the migraine cases and their partners. While not a primary focus of this research, this control group was selected to compare responses regarding work performance and satisfaction with responses of migraine sufferers and partners of migraine sufferers. Subjects were eligible for the control group if they did not suffer from migraine, did not experience photophobia, phonophobia, or nausea more than rarely, and agreed to provide an address for a follow-up interview. The demographic characteristics of those who agreed to the follow-up interview (n = 376) closely resembled those subjects who refused a subsequent in-depth interview.
Statistical analysis
Analyses were performed using Stata (Intercooled Stata 6.0 for Windows, College Station, TX. USA). The χ2 test was used to determine statistical significance unless otherwise indicated.
Results
Sample characteristics and participation (Fig. 1)
In the UK, 7224 households were contacted by telephone over a 4-week period; 1569 of these households (21.7%) refused to participate before the eligibility of any member could be established. Among the remainder, 1555 (27.4%) were not eligible (1457 because of age, 26 because of language barrier, 53 who could not adequately communicate because of their mental or physical condition and 19 for other reasons). Of the 4100 eligible households, 4007 (97.7%) provided a complete interview. Assuming that 27.5% (i.e. 432) of the unwilling households were also ineligible, we estimated that the overall participation rate in this first interview was 4007/(7224 − [1555 + 432]), or 76.5%.

Sample characteristics and participation rates in the UK and USA. ∗Proportions with regard to those who agreed to participate. †Proportions with regard to eligible households. ‡Proportions with regard to those who completed interviews. §Proportions with regard to the migraine probands identified. ¶Proportions with regard to those probands who completed the family impact interview.
In the USA, 11 863 households were contacted during 2 months, of which 4205 (35.4%) refused to participate before eligibility could be established. Of those remaining, 3101 (40.5%) were not eligible (2147 because of age, 613 because of language barrier, 149 who could not adequately communicate because of their mental or physical condition and 192 for other reasons). Of 4557 eligible households identified, 4376 (96.0%) provided complete interviews. Assuming that 40.5% (i.e. 1703) of those who refused were not eligible, the overall participation rate was 4376/(11 863 − [3101 + 1703]), or 62.0%.
Totals of 568 (12.9% of 4376) and 574 (14.3% of 4007) adults with migraine were identified from the US and UK populations. Of these, 280 (49.3%) in the USA and 297 (51.7%) in the UK were living with partners. A total of 246 (43.3%) migraine sufferers in the USA and 143 (24.9%) in the UK completed the family impact interviews. In addition, 37 partners (13.2%) in the USA and 63 (44.1%) in the UK also completed interviews.
Representativeness of the sample
For both the US sample (Table 1) and the UK sample (Table 2), sociodemographic characteristics of migraine cases who participated in the second interview were generally similar to those of the larger population (i.e. all migraine cases) from which they were selected. Those with partners were slightly older, had higher incomes, and larger households. Participants in the second interview resembled the entire migraine sample with regard to gender, age, and race.
Sociodemographic characteristics of migraine probands and migraine probands with partners in the US sample

Sociodemographic characteristics of migraine probands and migraine probands with partners in the UK sample
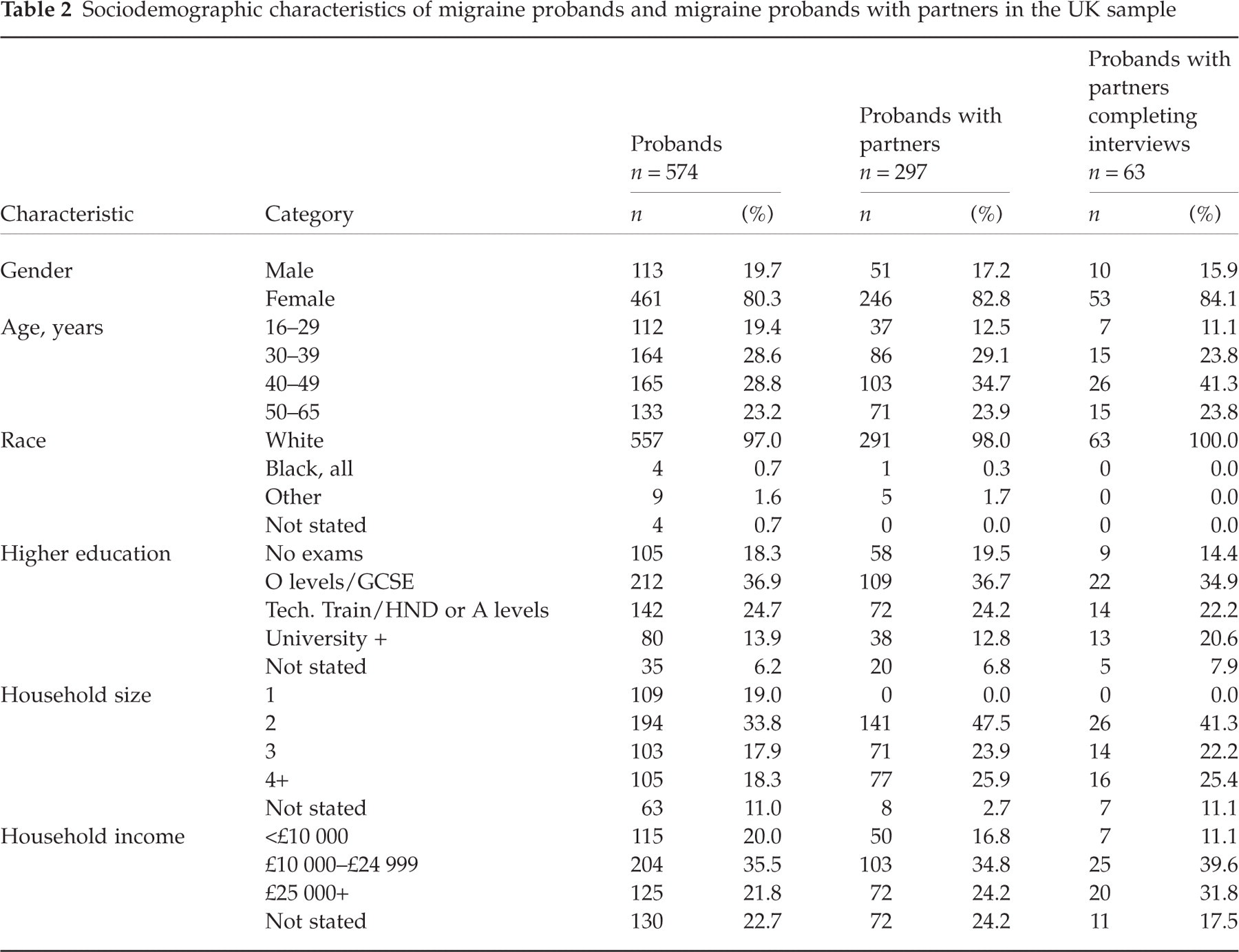
To assess representativeness of the subsets of probands whose partners completed interviews, we compared the demographic characteristics of all probands with those for whom an interview was completed with the partner (see Tables 1 and 2). The two groups were generally similar, both in the USA and in the UK.
Comparison of US and UK samples and subsets
We compared the US and UK samples of probands, probands with partners and those with partners who completed interviews. Because of the similarity of the USA and UK data, and our limited power for assessing differences, we elected to pool results. Pooling the samples, there were 330 females and 59 males with migraine who completed the family impact interviews.
Impact on social and leisure activities and family relationships
Table 3 displays the impact of migraine on the ability of the migraine sufferer to participate in housework and recreation, as reported by the proband. The vast majority (84.6%) of those directly affected by migraine reported a moderate or greater reduction in ability to do housework or chores (≥4 on a 0–10 scale) due to migraine; results were similar for women (84.8%) and men (83%). Three or more days of family or social activities had been missed in the past 3 months by 19.3% of migraine sufferers, and 32.4% had avoided making plans for family or social activities.
Impact of migraine on the headache sufferer's participation in housework and recreation by people with migraine, overall and by gender

∗Reduction rated on a scale of 0 = not reduced at all, to 10 = unable to do housework or chore.
Table 4 presents the results of partner interviews regarding the impact of the proband's migraine on the partner's participation in housework and recreation. Although one-third did not respond to the question, many partners (39.0%) had significant reduction in their ability to do housework or chores which they attributed to the proband's migraine. Three or more days of family or social activities were missed by 11.0%; 12.0% had avoided making plans for the family because of their partner's migraine.
Impact of migraine on the partner's participation in housework and recreation, overall and by gender
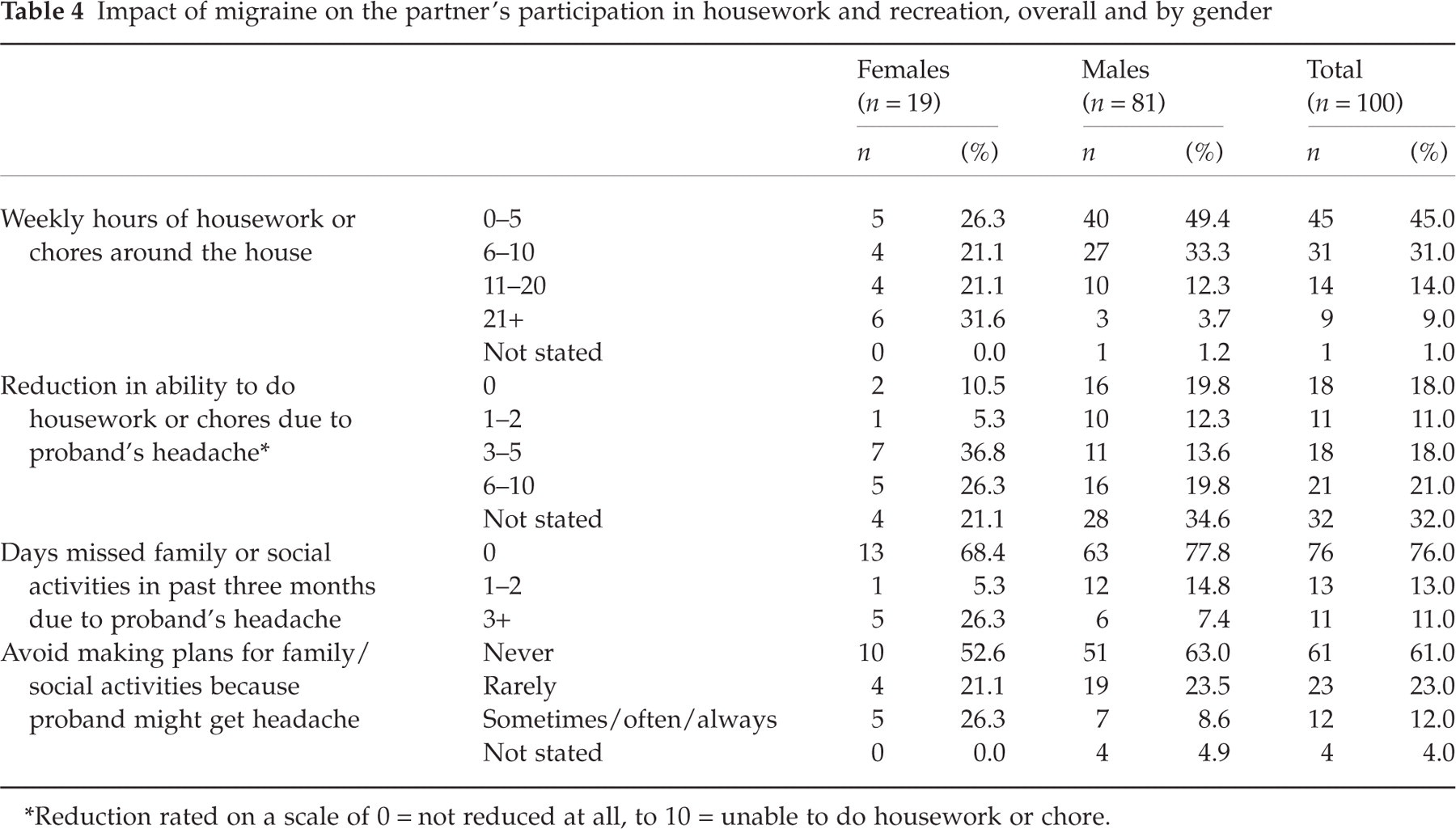
∗Reduction rated on a scale of 0 = not reduced at all, to 10 = unable to do housework or chore.
Migraine probands also reported a negative impact on their relationships with their children (Table 5). This impact was moderate or severe in 62.7% of cases (score 4–10). Many felt less able to relate to their children and 43.2% thought they would be better parents but for their headaches. Results for men and women were similar. Migraine in a parent adversely influenced their children's school attendance: 9.5% of the children had missed school in the past year because of their parents’ migraine (10.2% for female parents vs. 3.8% for male parents), and 10.8% of children had been late for school or left early (11.6% for female parents vs. 3.8% for male parents).
Impact of migraine on relationships with children of those with migraine, overall and by gender

The sample size presented regards migraine sufferers with children that completed the interview.
∗Rated from 0 = no impact to 10 = most severe impact.
The impact of migraine on relationships with household partners is presented based on interviews with the probands (Table 6) and with their partners (Table 7). Both groups reported that migraine adversely interfered with communication, reduced the time they spent together, and increased the number of arguments. Interestingly, a higher number of those with migraine reported these presumably shared problems than did their partners. Half (49.6%) of the probands agreed with the assertion ‘If I didn’t have a headache I would be a better spouse’, whereas only 12.3% of partners agreed that ‘if my partner did not have headaches, he/she would be a better spouse’.
Impact of migraine on relationships with household partner of those with migraine, overall and by gender, as reported by probands

Impact of migraine on relationships with household partner of those with migraine, overall and by gender, as reported by partners

∗May report more than one response.
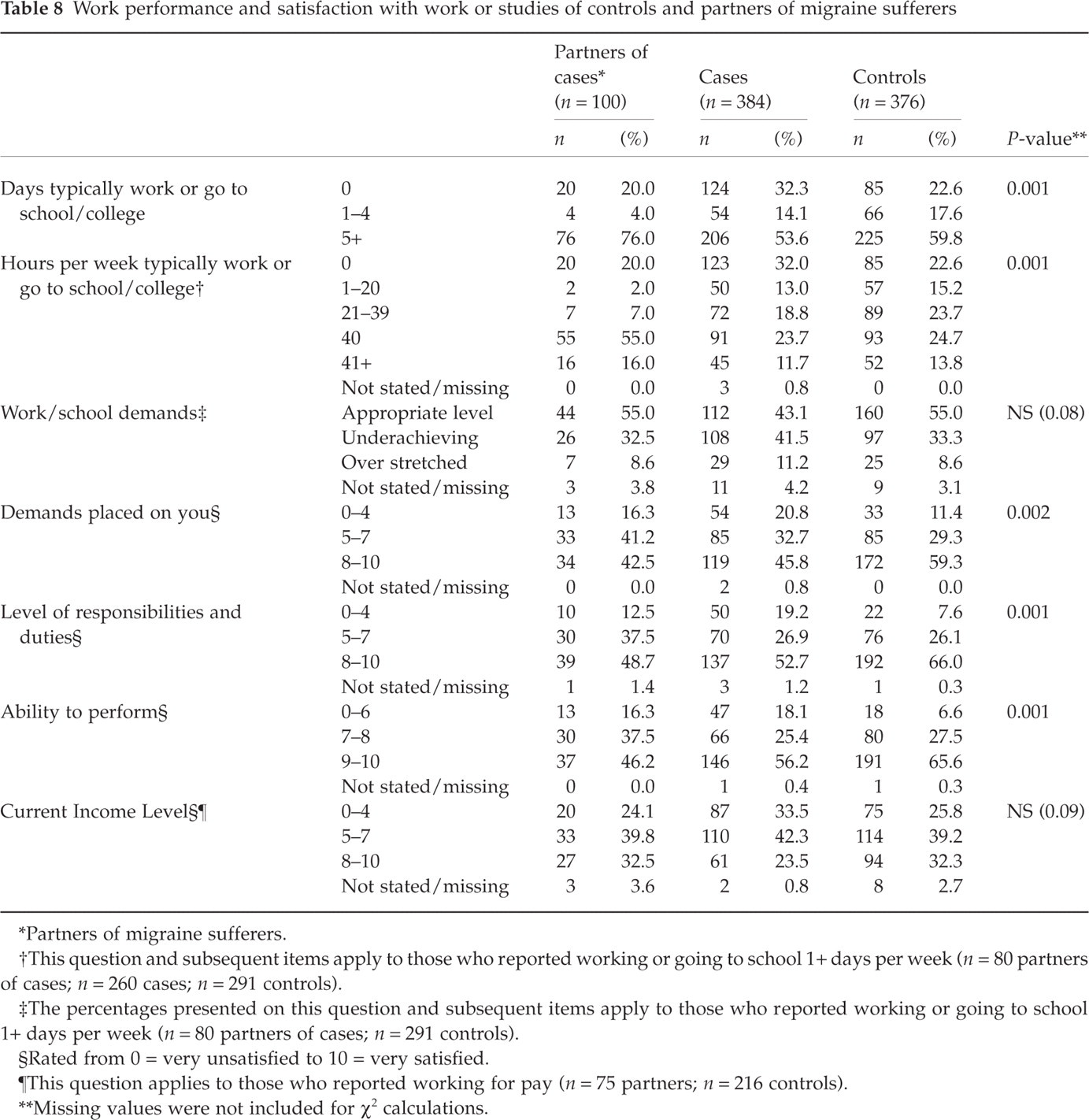
The partners of migraine sufferers were compared with migraine sufferers and with subjects who did not have migraine (controls as described in Methods) regarding their work performance and satisfaction with work (Table 8). A significantly higher proportion of migraine partners were dissatisfied with the demands placed on them (P = 0.002), with their level or responsibilities and duties (P < 0.001), and with their ability to perform (P = 0.001) compared with the control group. Migraine sufferers and their partners tended to be similar with regard to their perceptions of work perfromance and satisfaction.
Work performance and satisfaction with work or studies of controls and partners of migraine sufferers
∗Partners of migraine sufferers.
†This question and subsequent items apply to those who reported working or going to school 1+ days per week (n = 80 partners of cases; n = 260 cases; n = 291 controls).
‡The percentages presented on this question and subsequent items apply to those who reported working or going to school 1+ days per week (n = 80 partners of cases; n = 291 controls).
§Rated from 0 = very unsatisfied to 10 = very satisfied.
¶This question applies to those who reported working for pay (n = 75 partners; n = 216 controls).
∗∗Missing values were not included for χ2 calculations.
Discussion
The present study shows that, in population samples of people with migraine from the USA and UK, migraine sufferers report a substantial negative impact on participation in family life, family relationships and satisfaction with work. Many respondents reported that they were less able to communicate and more likely to argue with their children, felt less involved with home and school and spent less time with the children. Almost half felt they could be better parents if they did not have migraine. These feelings were more common among women than among men with migraine. Many also felt less able to communicate and more likely to argue with their partners, and that they could be a better partner if they did not have headaches.
Our results highlight the impact of migraine on the family lives of those with the disorder and, crucially, its spread to other family members. Though the effect of pain on family life has been extensively examined (19, 20), few studies have dealt specifically with migraine. Smith (15) interviewed migraine sufferers about their family lives, reporting that 60% believed their families were significantly affected, and 36% took a negative attitude (isolation or sense of guilt) towards their partners. People with migraine not infrequently cancel family or social activities (13, 15, 21), thereby generating guilt toward their spouses and children (22). In Smith's study (15), frequency and quality of sexual relationships were decreased, and divorce occurred in some cases. Another study (22) evaluating the marital relationships of 117 people with headache and their spouses, compared with couples without migraine, found that couples with headache had greater problems with cohesion. Families including a migraine sufferer showed less openness in expressing their feelings compared with both families with chronic back pain sufferers and families without chronic pain (23). These studies suggest that ‘family disharmony, instability and conflict may be caused by migraine’ (15).
In this study, interviews with partners support the views of those with migraine and suggest that migraine disrupts family life (14–16, 19–23). Partners reported that, from their viewpoint, headaches negatively influenced their relationships (Tables 3, 4, 6 and 7). Problems in relationships might be expected to be shared, and perceived, equally. Perhaps the migraine sufferers’ sense of isolation and guilt toward their partners accentuates perception of disease impact. Perhaps their partners underestimate the burden.
Partners of people with migraine reported decreased work performance and dissatisfaction with their work demands, responsibilities and duties, compared with a control group (Table 8). While several studies have demonstrated the substantial indirect costs of migraine (8–11, 24), these results suggest that migraine in the family may also reduce the productivity of persons other than the migraine sufferer. Our results are consistent with those of Stang et al. (24), who reported that the employed partner in the family of migraineurs loses, on average, 4 additional days due to diseases, 5 additional days due to short-term disability and 3 additional days due to worker's compensation, compared with controls in non-migraine families. Considering that migraine sufferers tend to have lower incomes than other workers (25), an additional economic impact on their partners can only supplement family economic problems, being another possible cause of disaggregation within the family.
Several cautions are recommended in interpreting these results. The migraine group was defined using a CATI based on IHS criteria, not a clinical assessment. The CATI has been well validated, both in the UK and the USA (5, 18) and has excellent operating characteristics; nonetheless, some degree of classification errors are likely. Diagnostic errors also occur during in-person assessments by a clinician (26, 27). The follow-up survey was limited to migraine sufferers who reported six or more headaches per year. These results may not apply to those with less frequent attacks, and therefore should not be extrapolated according to estimated prevalence of all migraine. Data from the American Migraine Study II (10) showed that 10% of the American migraineurs assessed in that survey had no headache in the previous 3 months (projecting less than six headaches per year), while 48% had from one to four (which projects 4–16 attacks per year, assuming the same headache frequency). Based on these data, we can estimate that we excluded 20–25% of migraine sufferers, with relatively low headache frequency.
Apart from this, the UK study was conducted in a population sample of mainland England we believe to be representative of the country. The US study was conducted in a geographically focused regional population sample. Prior studies in the USA demonstrate that migraine is relatively uniformly distributed in the USA; region and degree of urbanization have minimal influences on migraine prevalence and characteristics (5, 28). We therefore expect this regional population sample to provide a fair snap-shot of migraine in the USA, and a similar study in a nationally representative population sample generated similar results (5).
Perhaps more serious limitations arise from response rates, always a problem in research of this nature. The overall participation rates were higher in the UK than in the USA. This may be explained by the method of interview. In the USA, family members were interviewed by telephone. In the UK, follow-up interviews were conducted in person. In the USA, just 13% of the partners completed the family impact interview, which can create participation bias, perhaps by selecting proportionally more partners of severely disabled migraineurs. If this is true, we may underestimate the frequency but overestimate the severity of migraine. Alternatively, the low participation rate may have affected the representativeness of the partners’ sample, eventually biasing in the other direction, overestimating the results. Also, this is a limitation where the ‘non-stated’ answer was predominant (Question 2, Table 4). Finally, a last issue concerns the potential influence of co-morbidity. Because depression and other co-morbidities were not measured, we cannot investigate their influence on the present results. This issue does not challenge our findings, but rather their causal attribution. In addition, this survey reports the perception of migraine sufferers and their partners and does not rely on direct observation. Further, we did not have a control group for many of our observations.
In conclusion, our study shows that both people with migraine and their partners are significantly and adversely impacted by their headaches. Migraine imposes a heavy burden on the family beyond those borne directly by the affected person. In a context in which migraine remains under-recognized, under-diagnosed and under-treated (3, 29–32) despite numerous studies demonstrating effective migraine therapies that relieve pain and restore ability to function (27), this is yet more evidence of need for better medical care for migraine and access to it. Our data suggest that not only those with migraine but also their partners and their children would benefit.
Footnotes
Acknowledgements
The authors thank Pfizer Inc. for funding this research.