
Abstract
Background
The International Burden of Migraine Study (IBMS) showed chronic migraine (CM) was associated with a higher disease burden than episodic migraine (EM). However, in this study Asians with CM were underrepresented.
Objectives
We investigated if CM and EM differed in headache-related disability, health-related quality of life (HRQoL) and health care resource utilization in Taiwan.
Methods
This study recruited patients with EM and CM from two headache clinics in Taiwan. Diagnosis was made by physicians based on Silberstein-Lipton criteria. Participants completed a questionnaire including sociodemographics, Migraine Disability Assessment (MIDAS), EuroQol five-dimensions (EQ-5D), Migraine-Specific Quality of Life v2.1 (MSQ), Patient Health Questionnaire-4 (PHQ-4), productivity and health care resource utilization.
Results
A total of 331 patients (EM, n = 164 (49.5%); CM, n = 167 (50.5%)) completed the study. CM patients reported a significantly higher MIDAS score, lower generic (EQ-5D visual analogue scale score and EQ-5D index score) and migraine-specific (all three domains of MSQ) HRQoL, higher levels of anxiety and depression (PHQ-4 ≥ 6) and greater health care resource utilization and productivity loss than those with EM. Positive correlations were found between these instruments and levels of anxiety and depression.
Conclusion
Compared to EM, CM was significantly associated with higher disability, lower HRQoL and greater health care resource utilization and productivity loss.
Introduction
Migraine is a common and disabling neurological disorder (1) with one-year prevalence ranging from 4.5% to 8% for men and from 8% to 16% for women (2–9). The prevalence of migraine is 4.5% for men and 14.4% for women in Taiwan (10); however, a meta-analysis showed Asians have a lower prevalence than Caucasians (11). Patients with migraine can be classified into two subgroups based on headache frequency: episodic migraine (EM; <15 headache days per month) and chronic migraine (CM; ≥15 headache days per month) (12). In the second edition of the International Classification of Headache Disorders (ICHD-II), CM is listed as a complication of migraine (12). Debates on the specific criteria for CM remain; however, a headache frequency of ≥15 days per month is generally accepted for CM (13,14). The prevalence of CM in the general population is estimated as 1.4%–2.2% (15); however, more than half of the patients in the headache clinics had CM (16,17).
Migraine attacks usually cause major disability in occupational and school performance, household work function, and social and leisure activities (18,19). Migraine is ranked 19th of the disabling disorders among all single causes by the World Health Organization (WHO) (2). The disability of severe migraine attack is comparable to dementia, quadriplegia, or acute psychosis (20,21). Patients with migraine also had lower health-related quality of life (HRQoL) (18,22,23).
In addition, migraine prevalence was the highest during the peak productive years – between the ages of 20 and 45 (24). Therefore, the consequent impact of migraine in society would be substantial. In the American Migraine Prevalence and Prevention (AMPP) study, 655 CM patients, compared with 11,249 EM patients, were associated with approximately two times higher levels in prevalence of depression, anxiety and chronic pain (25). Respiratory disorders were also more likely to be reported by those with CM (25). In addition, in patients with CM, health care costs and reduction in productivity at work were more severe compared to those with EM (26,27).
Recently, a worldwide Web-based study, the International Burden of Migraine Study (IBMS), collected data from several countries in Western Europe, North America and Asia/Pacific. In the IBMS study, 5.7% of the respondents were diagnosed with CM and 94.3% with EM. CM patients, compared to EM patients, were more likely to be disabled, had lower HRQoL, higher levels of anxiety and depression, and greater health care resource utilization (28,29). Of note, the ethnic composition differed between CM and EM groups. There were more Caucasian and Hispanic participants in the CM group, but fewer Asian participants (28,29). In the only Asian country that participated in the IBMS study, Taiwan, a very small number of CM patients (n = 8) were recruited. The low recruitment of CM patients might be explained by the fact that participants in Taiwan were contacted from a general pool of survey participants rather than a headache or migraine prescreened population like the other participating countries.
The objectives of this study are to characterize EM and CM from a clinic sample in Taiwan in order to better understand the sociodemographic features and to determine the impact on HRQoL, health care resource utilization and productivity. We employed most of the instruments used in the Web-based IBMS study. The results can be utilized to complement these data of patients with CM in Asians.
Methods
This was a cross-sectional, clinic-based observational survey with participants from two headache clinics in Taiwan from February to April 2011.
Clinic settings
Taipei Veterans General Hospital (VGH) is a 2918-bed national medical center that serves veterans as well as nonveteran citizens. The hospital is located in Taipei, which is the capital of Taiwan and a major urban center with a population of approximately 2.64 million. Most of the patients of Taipei VGH come from northern Taiwan. The headache clinic of Taipei VGH has been operating since 1996. Living Water Neurological Clinic is located in the city of Tainan, and a headache clinic has been operating since 2004. Despite a population of 740,000, Tainan is not as developed as Taipei in terms of infrastructure and facilities. In Taiwan, the referral system has not been utilized efficiently; therefore, almost all patients at these two headache clinics were self-referred.
Study subjects
During the study period, patients with migraine in these two outpatient headache clinics were invited to participate in the survey. All male and female potential participants in these two headache clinics were eligible for inclusion in the survey if they (1) were ≥20 and ≤65 years of age and were able to read and understand the survey questionnaire; (2) had migraine diagnosed by neurologists, not excluding those fulfilling criteria for medication-overuse headache based on the ICHD-II criteria; (3) had a headache for at least three months and had a headache for at least one day in the past month; and (4) were willing to join the study. This study was approved by the Institutional Review Boards at Taipei VGH hospital for the Taipei VGH headache clinic and Chi-Mei hospital for Living Water Neurological Clinic. All the participants provided their informed consent before joining the study.
Migraine diagnosis and categorization
The neurologists filled out the headache profiles and made the headache diagnoses by using a structured interview and performed neurological examinations of all participants. In addition, the participants were also asked to report, in the past three months, the average number of days per month with a headache of any intensity and also the average number of days with a headache of at least four hours. For comparison with IBMS results, eligible participants were categorized as either EM (<15 headache days per month) or CM (≥15 headache days per month) (13), i.e. Silberstein-Lipton criteria, by the neurologist.
This study aimed to recruit 330 patients with migraine with about an equal number of patients with EM and CM. In patients with CM, medication overuse (MO) was also surveyed according to the ICHD-2 revised criteria (13). Of note, presence of MO did not contradict the diagnosis of CM in this study. In addition, in patients with EM, a prior history of CM was also surveyed.
Data collection
Sociodemographics and comorbidities
Participants reported their age, gender, race, marital status, employment status, education, household income and height and weight. Body mass index (BMI) was calculated as body weight divided by body height squared (kg/m2) for each subject. In addition, comorbid conditions were defined as self-report of a physician diagnosis. Comorbid conditions were further divided into five categories (psychiatric, pain, vascular disease risk factors, vascular disease events and others), which were modified from the Web-based study of IBMS (28,29) for comparisons.
Migraine Disability Assessment Questionnaire (MIDAS)
The five-item MIDAS questionnaire, used to assess headache-related disability in the past three months, is the most frequently used instrument to measure disability in migraine research and clinical practice (30–32). The scores range from 0 to 270 and a four-grade grading system is used to measure headache-related disability: grade I, little or no disability (score of 0–5); grade II, mild disability (score of 6–10); grade III, moderate disability (score of 11–20); and grade IV, severe disability (score of ≥21). Of note, in a five-grade grading system, the highest category is subdivided into grade IV-A, severe disability (scores of 21–40) and grade IV-B, very severe (scores of 41–270) (28). The introduction of this new scoring method allows for a higher sensitivity to highlight the higher disability experienced by CM patients compared to EM patients (29).
Migraine-Specific Quality of Life Questionnaire, version 2.1 (MSQ)
The MSQ (33) is a 14-item questionnaire designed to measure migraine-specific HRQoL by assessing the limitation of daily performance. MSQ is composed of three domains: role function-restrictive, role function-preventive, and emotional function. The first two domains assess the reduction and prevention of daily social- and work-related activities, whereas the last assesses the emotion related to migraine. In each of the three domains, a sum of the item responses is computed and rescaled to a 0–100 scale. Higher scores indicate better HRQoL.
EuroQol five-dimensions (EQ-5D)
The EQ-5D is a self-reported health status with coverage of five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and general health status. The health states from each of the five dimensions are converted into a weighted health state index by applying scores from the EQ-5D preference weights elicited from general population samples. These weights lie on a scale on which full health has a value of 1 and death a value of 0. The instrument also includes a 20 cm vertical visual analogue scale (VAS) to capture health self-ratings, with 100 at the top representing best imaginable health, and 0 at the bottom representing worst imaginable health (34).
Patient Health Questionnaire-4 Items (PHQ-4)
PHQ-4 consists of two core anxiety items and two core depression items and is an ultra-brief screening tool for anxiety and depression (37). A four-point Likert-type scale (0–3) is used for each of the four items, resulting in a total score of 0 to 12. The severity of anxiety and depression was graded according to the total score: normal (0–2), mild (3–5), moderate (6–8) and severe (9–12). In this study, a PHQ-4 score of ≥6 was calculated to indicate moderate to severe anxiety and depression, whereas the total score of PHQ-4 indicates the level of anxiety and depression.
Except for the PHQ-4, all the above instruments for disability and health-related quality of life, including MIDAS, MSQ and EQ-5D, have been validated in Chinese.
Health care resource utilization
Information on health care professional visits, use of the emergency department, overnight hospital stay, diagnostic tests, and headache treatments including pharmacologic (migraine preventive medications, acute abortive medications, botulinum toxin injection and alternative treatment) and non-pharmacologic (transcutaneous nerve stimulator procedures, occipital nerve block procedures, acupuncture and change in diet, sleep, or day-to-day behavior) treatments over the last three months were obtained from the participants. This part was modified from the Web-based study of IBMS (28,29) for comparisons.
Statistical analysis
Descriptive statistics were expressed as mean ± standard deviation (SD) for continuous variables. The Student t test was used to compare the continuous EM and CM data. The Chi square or Fisher’s exact tests were used for categorical data. A general linear model (GLM) was used to evaluate differences between EM and CM, controlling for covariates of age, gender, and comorbidities, expressed as linear squares (LS) mean ± standard error (SE). The clinical correlates of MIDAS, MSQ and EQ-5D index score and VAS score were also analyzed by GLM. A p value <0.01 was regarded as statically significant, balancing the risk of type I and II errors for multiple comparisons.
Results
Sample characteristics
Sociodemographic characteristics by migraine subgroup.

NT: New Taiwan dollars. The current exchange rate (August 2012) was about one US dollar to 30 NT dollars; BMI: body mass index.
Clinical characteristics of participants
Summary of migraine features and diagnoses by migraine subgroup.

The significant variables (p < 0.01) are highlighted in bold; ICHD-2: Second edition, International Classification of Headache Disorders.
Comorbidities with CM and EM
Comorbidity by migraine subgroup.

The five comorbidity (self-report of a physician’s diagnosis) groups are defined as follows:
Pain: Chronic pain (excluding headache or migraine), rheumatoid arthritis/osteoarthritis, fibromyalgia; Vascular disease risk factors: high blood pressure, high cholesterol; Vascular disease events: heart attack (myocardial infarction), stroke, transient ischemic attack, heart disease/angina (chest pain); Psychiatric disorders: depression, anxiety, nervous or excessive worry; and Other conditions: Irregular heart rhythms (palpitations or arrhythmias), premenstrual syndrome/menstrual problems, epilepsy/seizures/convulsions or “fits,” sinusitis or sinus infection, ulcers of the stomach or intestines, other (excluding headache or migraine).
MIDAS classification (headache-related disability)
CM participants had significantly higher mean MIDAS scores (CM: 46.1 ± 49.2 (grade IV-B) vs. EM: 14.4 ± 23.4 (grade III), p < 0.001), indicating more severe disability compared to EM participants. After controlling for age, gender, and number of comorbid disorders, CM participants still had more severe disability compared to EM participants (CM 45.2 ± 3.3 vs. EM 17.2 ± 3.3, p < 0.001). The proportions of participants (adjusted for covariates) with MIDAS score ≥21 (grade IV severe disability) and ≥41 (grade IV-B very severe disability) were 59.3% and 41.3% for CM, compared to 21.9% and 7.9% for EM respectively (both p < 0.001) (Figure 1).
Migraine Disability Assessment (MIDAS) score grading by migraine subgroup.
Migraine-specific quality of life (disease-specific HRQoL)
CM was associated with lower MSQ scores in three domains: role function-restrictive (56.4 ± 17.3 vs. 70.8 ± 13.8, p < 0.001), role function-preventive (70.0 ± 18.2 vs. 81.4 ± 16.2, p < 0.001), and emotional function scores (62.0 ± 23.0 vs. 78.1 ± 16.8, p < 0.001) (Figure 2). These differences remained statistically significant after adjustment for other covariates (p < 0.001). All else being equal, the average MSQ scores in CM patients compared with EM patients were 9.2 points lower on the Function-Restrictive subscale (minimal important differences (MID) 3.2), 6.8 points lower on the function-preventive subscale (MID 4.6), and 8.0 points lower on the emotional function subscale (MID 7.5). Such differences are considered clinically significant (35).
Migraine-Specific Quality of Life Questionnaire (MSQ) three subscales by migraine subgroup.
PHQ-4 (anxiety and depression)
A higher level of anxiety and depression, measured by PHQ-4, was reported by CM patients compared to EM patients (CM: 4.7 ± 0.2 vs. EM: 2.3 ± 0.2, p < 0.001). The differences remained significant after adjustment for other covariates (p < 0.001). Moderate to severe anxiety and depression (PHQ-4 scores ≥6) was more common for CM patients than EM patients (33.5% vs.7.9%, p < 0.001) (Figure 3).
Patient Health Questionnaire-4 Items (PHQ-4) to measure the severity of depression and anxiety by migraine subgroup.
EuroQoL five-dimensions (generic HRQoL)
Compared with the EM group, the CM group had a lower EQ-5D VAS (67.4 ± 18.7 vs. 82.3 ± , p < 0.001) and a lower EQ-5D index score (0.73 ± 0.27 vs. 0.91 ± 0.15, p < 0.001).
Health resource utilization
Use of medical resources due to headache during past three months by migraine subgroup.

Past four weeks instead of past three months.
Among the participants with EM (n = 164), 38 (23.2%) had a past history of CM. At the time of enrollment in the current study, these 38 patients no longer fulfilled the diagnosis of CM and were grouped into the EM group. Regarding the proportion of usage of preventive medications, patients with EM with a prior CM history were similar to those in the CM subgroup (57.9% vs. 48.5%, p = 0.30). The comparisons between EM participants with and without a prior history of CM showed no difference in age, gender, employment status, disability, HRQoL, psychiatric comorbidity, and medical resource utilization (data not shown).
Comparison between CM participants with and without MO
Among the 167 participants with CM, 48 (28.7%) had medication overuse (MO). The demographics, including age, gender, marital status, employment status, education level, and annual household income between those with and without MO were not different (data not shown). However, CM patients with MO, compared to CM patients without MO, had more headache days per month (24.1 vs. 21.1, p = 0.004), but the comparisons of the MIDAS, PHQ-4, MSQ, and ED-5D scores were not different.
Clinical correlates of disabilities or impairment of HRQoL
Results of general linear regression model to test for predictors of MIDAS, EQ-5D, and MSQ subscales.
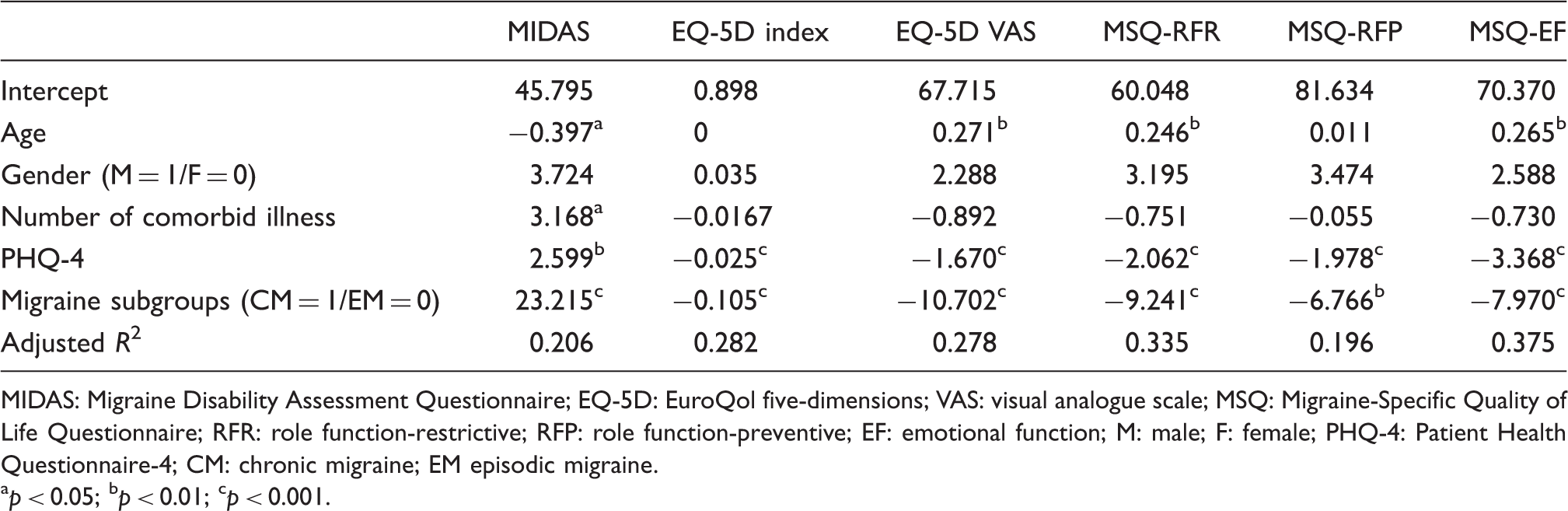
MIDAS: Migraine Disability Assessment Questionnaire; EQ-5D: EuroQol five-dimensions; VAS: visual analogue scale; MSQ: Migraine-Specific Quality of Life Questionnaire; RFR: role function-restrictive; RFP: role function-preventive; EF: emotional function; M: male; F: female; PHQ-4: Patient Health Questionnaire-4; CM: chronic migraine; EM episodic migraine. ap < 0.05; bp < 0.01; cp < 0.001.
Discussion
This study has shown that the disease burden of both EM and CM are high in Taiwan using a similar survey questionnaire as the international Website survey, IBMS (28,29). Compared to EM patients, CM patients were more likely to be associated with psychiatric and chronic pain disorders. Our study also confirms CM is associated with high levels of migraine-related disability. In addition, CM patients also had a poorer HRQoL and imposed a greater burden on the health care system. This study provides additional data to highlight the significant disease burden of CM in Asians despite the under-representation of Asians with CM in the IBMS study (28,29).
Our study demonstrated that the level of anxiety and depression, i.e. the total score of PHQ-4, was one major determinant of poorer HRQoL and higher disability of migraine patients. Consistent with our previous study conducted on a clinic-based sample (36), HRQoL measured by the Short Form Health Survey (SF-36) among patients with different headache diagnoses was determined greatly by the psychological distress and pain profile. Therefore, an improvement in the pain profile or psychological well-being may predict an improvement in HRQoL (36). In fact, in the current study, the level of anxiety and depression was associated with worse generic (EQ-5D VAS and EQ-5D index scores) and migraine-specific (MSQ) HRQoL, and higher migraine-related disability (MIDAS). Since HRQoL improvement and pain control are the goals of migraine treatment (37), the management of psychological distress or psychiatric comorbidity should not be overlooked.
Due to a higher frequency of headache, it is expected that CM patients would have a higher disability compared with EM patients (26,38–40). In this study, we used the new scoring system of five-grade MIDAS as suggested by the IBSM study to better characterize headache-related disability (29). The traditional four-grade MIDAS scoring system, with grade IV ≥21 points indicating severe disability, may mask the worse disability in patients with CM. In fact, almost half of the patients (41.3%) with CM in our study were grouped into MIDAS grade IV-B, i.e. ≥41 points. In addition, in all migraine patients with MIDAS grade IV, EM patients had a higher proportion of grade IV-A (64%) but CM patients had a higher proportion of grade IV-B (69%, p < 0.001).
Regarding the use of medical resources, CM patients had more emergency room visits and hospitalizations compared to EM patients. Such a trend is also seen in most European countries (28), possibly reflecting the high frequency of headaches in CM patients and unmet treatment needs, i.e. poorer pain control. In addition, in our study, as expected, more CM patients were using migraine-preventive medications compared to EM patients (48.5% vs. 31.7%). Of note, the rates of preventive-medication use in both subgroups were higher than those in most European countries (28). Such a difference might reflect the different clinical settings between studies (headache-specific clinic-based vs. Internet Web-based survey). Still, in our study, more than half of the CM patients were not receiving preventive medications, highlighting the issue of under-treatment in CM patients.
Despite the remarkable difference between EM and CM, we found that the participants with EM with and without a prior history of CM were indistinguishable regarding disease burden. It indicates that after treatment, HRQoL, migraine-related disability, and health care utilization would improve along with the change from CM to EM. Many EM patients with a prior history of CM in our study were still on migraine-prophylactic agents (57.9%). These findings support an optimal treatment of CM to improve the welfare of the patients and to reduce the burden of the health care system.
Though the comorbidity, disability, and HRQoL differed between CM and EM patients in our study, most of the headache characteristics and associated symptoms were not different between CM and EM. Such findings were reported in two recent studies, including the IBMS study (29,41). However, this observation conflicted with the previous belief that, after transformation from EM to CM, migrainous features become less prominent and the characteristics of “transformed migraine” are similar to chronic tension-type headache (42,43). Therefore, identification of migrainous features in those with chronic daily headache is crucial during the clinical assessment to establish a correct diagnosis.
Certain aspects should be emphasized for this study especially in comparison with the IBMS study: (1) The participants in our study were diagnosed and classified by headache specialists rather than questionnaires. (2) The study was a paper-and-pen questionnaire design rather than an Internet Web-based survey. (3) Most important, selection bias existed based on different settings, i.e. Web-based vs. clinic-based surveys. The patients with EM in this study might represent a more severe subgroup of EM due to the fact they were followed up at headache-specific clinics, and the proportion of use of migraine-preventive medication was relatively high (31.7%). However, in Taiwan this is less of an issue given that our health care system does not adopt a strict referral system and thus almost all patients in these two headache clinics were self-referred and more than 99% of the population is covered by national health insurance. In addition, the current study recruited patients from a national medical center as well as a primary-care clinic. Therefore, our study results accurately reflect the general population in need of medical care in Taiwan. Last, some of the items in the questionnaire of the current study, including MIDAS, EQ-5D and MSQ, have been validated in Taiwan, but other parts of the questionnaire, including demographics, past medical history, drug history, use of medical resources, etc., were modified and translated from the IBMS study by experts. Still, the similarity between our study and IBMS, the Web-based survey that adopted prescreened panelists, are complementary. However, more studies are mandatory to understand the true sampling framework of the Internet-surveyed studies.
The identification of disease-specific needs of CM and EM patients in Taiwan is, in general, compatible with the Web-based multinational IBMS study. Additionally, the indistinguishable disease burden between EM with and without a prior history of CM further suggests that optimal treatment of CM is mandatory. In summary, the current study is not considered as merely filling the gap of under-representation of Asians in the IBMS study, but, since the clinical settings and methodologies differed, both studies can be considered complementary to a certain degree.
Clinical implications
In Asian subjects, chronic migraine (CM) is associated with a higher disease burden than episodic migraine (EM). CM is associated with higher disability, measured by the Migraine Disability Assessment (MIDAS), and lower health-related quality of life (HRQoL), measured by EuroQol five-dimensions (EQ-5D), and Migraine-Specific Quality of Life v2.1 (MSQ). CM is associated with higher levels of anxiety and depression, measured by the Patient Health Questionnaire-4 (PHQ-4). CM is associated with greater health care resource utilization and productivity loss. Positive correlations were found between the above instruments and the levels of anxiety and depression.
Footnotes
Acknowledgement
The funders had no role in data collection and analysis. Part of this study was published as an abstract at the XXth World Congress of Neurology, Marrakesh, Morocco, 12–17 November 2011.
Funding
The study was supported in part by the Taiwan Headache Society and Allergan Singapore Pte Ltd.
Conflict of interest
None declared.