
Abstract
We performed whole-spine heavily T2-weighted magnetic resonance (MR) myelography using a single-shot fast spin-echo pulse sequence in 17 patients (8 M/9 F) with spontaneous intracranial hypotension (SIH) to detect abnormal cerebrospinal fluid (CSF) collections. In addition, a group of age- and sex-matched controls were recruited. Follow-up MR myelography was also done at 3 weeks. MR myelography showed three kinds of abnormal CSF collections in 15 patients with SIH (88%): epidural fluid collection (n = 15, 88%), C1-2 extraspinal collections (n = 6, 35%) and CSF collections along nerve roots in the lower cervical or upper thoracic spines (n = 6, 35%). One patient (6%) showed a meningeal diverticulum. In contrast, none of the controls showed these findings. Overall, MR myelography results helped in early diagnosis of SIH in four (24%) patients whose initial brain MRIs failed to show typical SIH findings. Follow-up MR myelography results were compatible with the clinical changes with κ statistics of 0.52 and an agreement rate of 76%. Our study showed heavily T2-weighted MR myelography provided a rapid, non-invasive and high yield method to diagnose and follow-up patients with SIH. Whether the CSF collections along the nerve roots represent the ongoing leakage sites warrants further study.
Introduction
Spontaneous intracranial hypotension (SIH) is a syndrome characterized by postural headache. Typical brain magnetic resonance imaging (MRI) findings are diffuse pachymeningeal enhancement, brain descent and pituitary gland enlargement (1, 2); however, previous studies have shown that 7–29% of patients with SIH do not exhibit typical MRI findings of the brain (3–5). Evidence suggests that spinal cerebrospinal fluid (CSF) fistulas are responsible for this syndrome (1, 2). Invasive imaging studies, such as conventional myelography, computed tomographic (CT) myelography or radioisotope cisternography are often required to demonstrate the exact leakage sites (1, 2). However, these diagnostic studies raise some concerns, such as symptomatic worsening following lumbar puncture, contrast medium allergy or exposure to radionuclide irradiation; these, in turn, make imaging follow-up less likely. Furthermore, the sensitivity of these studies varies (6–10).
Heavily T2-weighted magnetic resonance (MR) myelography can be used to image water by generating a superimposed image of the CSF in the spinal canal (11). This technique has been employed in patients with various spinal diseases (12, 13). Theoretically, its ability to demonstrate the ‘CSF collections’ provides an opportunity for its use in patients with SIH. However, only a few cases have been reported to date, including ours (5, 6, 14–18). The characteristics and utilization of this technique in patients with SIH have not been systematically studied.
We present the findings of MR myelography in patients with SIH. For comparison, a group of control subjects was also recruited and the MR myelography findings were correlated with clinical presentations.
Methods
Subjects
We consecutively enrolled patients with SIH who visited Taipei-Veterans General Hospital. Patients had to fulfil the criteria for headache attributed to spontaneous low CSF pressure (code 7.2.3) based on the International Classification of Headache Disorders, 2nd edition (ICHD-2) (19). None had a previous history of dural tear such as lumbar puncture, head trauma or surgical drainage. In addition, age- and sex-matched subjects were also recruited as normal controls. They were recruited from colleagues, their relatives and patients from the clinic and were generally healthy or at most had episodic migraine or tension-type headache. None of them had orthostatic headaches.
Study protocols
Both patients with SIH and control subjects underwent heavily T2-weighted MR myelography. Patients with SIH also underwent brain MRI with contrast medium. Of note, if the initial brain MRI study was negative, a repeat MRI of brain was done 2 weeks later. All SIH patients had repeat follow-up MR myelography 3 weeks after either conservative treatment or epidural blood patches (EBP). Some patients needed more follow-up MR myelography studies based on their clinical condition. Clinical symptoms were recorded for comparison. The study protocol was approved by the Institutional Review Board of the hospital. All patients and control subjects provided written informed consent prior to the study.
Heavily T2-weighted MR myelography
MR myelography was performed with a 1.5-T superconducting system (Signa CV/i and Signa EXCITE; GE Medical System, Milwaukee, WI, USA) using a phased-array synergy-spine coil. A single-shot fast spin-echo (SSFSE) pulse sequence with extremely long effective TE (i.e. heavily T2-weighted) was employed to acquire the MR myelography images of the entire spine. This sequence effectively demonstrated the presence of CSF and rapidly obtained images with minimal motion artefacts (13).
Longitudinal planes
Four longitudinal MR myelogram planes—coronal, midline sagittal and bilateral oblique orientations—were obtained for the cervical, thoracic and lumbosacral spines. The parameters were as follows: matrix size 320 × 256, TE 950 ms, TR 6000 ms, 50 mm section thickness and field of view (FOV) 280 mm.
Transverse planes
The whole-spine transverse planes of MR myelogram were taken from the cervical to the lumbar regions using the following parameters: matrix size 320 × 256, TE 950 ms, TR 6000 ms, 6 mm section thickness and FOV 200 mm.
It took 13 min to finish both longitudinal and transverse planes of the heavily T2-weighted MR myelography.
Image evaluation
One experienced neuroradiologist blinded to patient clinical conditions evaluated all MR myelogram images. Abnormal CSF collections were searched. The MR myelography findings in patients with SIH were recorded and compared with those of control subjects. The changes in imaging findings of SIH patients during follow-up were also recorded and compared with their clinical presentations.
Statistical analyses
Descriptive statistics were presented as means ± SD, median or percentages. SPSS Version 13.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for analysis. κ, χ2 and Fisher's exact tests were used, as appropriate. All statistical tests were two-tailed and significance levels were set at P-values of <0.05.
Results
Seventeen consecutive patients with SIH (8 M/9 F; mean age 43.5 ± 9.3 years) and 17 control subjects (8 M/9 F; mean age 41.7 ± 12.8 years) participated. Of the control subjects, four had episodic migraine and two had episodic tension-type headache. Initial MR myelography in patients with SIH was done after a median duration of 21 days (range 1–77 days) from disease onset. All patients received follow-up MR myelography 3 weeks after treatment. Five patients received one more follow-up MR myelography and, of those, one underwent a total of six MR myelographies due to a persistent extraspinal CSF collection.
Brain MRI findings
Thirteen patients (76%) showed typical SIH characteristics in the initial brain MRI, including diffuse pachymeningeal enhancement (n = 13, 76%), bilateral subdural haematoma (n = 6, 35%) and brain descent (n = 12, 71%). Of the four patients (24%) who showed negative results initially, three received follow-up brain MRI studies 2 weeks later. All showed typical diffuse pachymeningeal enhancement.
Initial MR myelography findings
MR myelography was done within 1 day of the brain MRI studies in patients with SIH. The findings of the initial MR myelography in longitudinal and transverse planes are summarized in Table 1. All four patients with an initial negative brain MRI showed abnormal CSF collections on MR myelography.
Findings of initial magnetic resonance myelography in patients with spontaneous intracranial hypotension and control subjects

SIH, Spontaneous intracranial hypotension; CSF, cerebrospinal fluid.
χ2 or Fisher's exact tests.
Epidural fluid collection
An epidural fluid collection was found in 15 patients (88%) and was more easily identified in transverse than in longitudinal planes. A low-density dura could be seen between the collapsed thecal sac and the epidural fluid leakage (Fig. 1). The involved segments of epidural fluid collections were at all levels (from cervical to lumbar regions) in eight patients, thoracic to lumbar regions in five and only the thoracic region in two. The average number of involved segments of the epidural fluid collections was 16 ± 6 (range 2–20) levels.

The transverse planes of the T-spine magnetic resonance myelogram demonstrate dura as a curvilinear low-signal component (arrowhead) and epidural fluid collections (arrows) over the ventral (A) and dorsal aspects (B).
Extraspinal fluid collections in the high cervical region
Six patients (35%) showed this finding (Fig. 2). The CSF fluid was located retrospinally in the C1–2 intervertebral space and within the paraspinal muscles (Fig. 3A). All these six patients showed epidural fluid collections involving all levels of the spine, i.e. from C2 to L2, 20 segments.

(A) The midline sagittal plane of the C-spine magnetic resonance myelogram shows retrospinal cerebrospinal fluid (CSF) leakage at the C1–2 level, from the dorsal aspect of the dural sac to the suboccipital region (arrow). (B) No further CSF leakage is found after treatment (arrow).

Long-term follow-up of C1–2 retrospinal leakage in a patient with a protracted course. He received three blood patches within 3 months but still complained of intermittent non-orthostatic neck pain. A series of transverse planes of the C-spine magnetic resonance myelogram demonstrated decreased retrospinal C1–2 cerebrospinal fluid leakage (arrow) and epidural fluid collection (arrowhead) at 21 days (A), 4 months (B), 7 months (C) and 15 months (D) after headache onset.
CSF collections alongside the nerve roots
Six patients (35%) showed this finding, which was detected as a high-signal, irregular, thread-like appearance, extending from the thecal sac to the extraspinal region (Fig. 4). Collections were located at the lower cervical (C6, n = 1) or thoracic region (T1–T5, n = 5; T8–10, n = 1). Of these, two patients had single nerve root involvement, whereas four had multiple nerve root involvement.
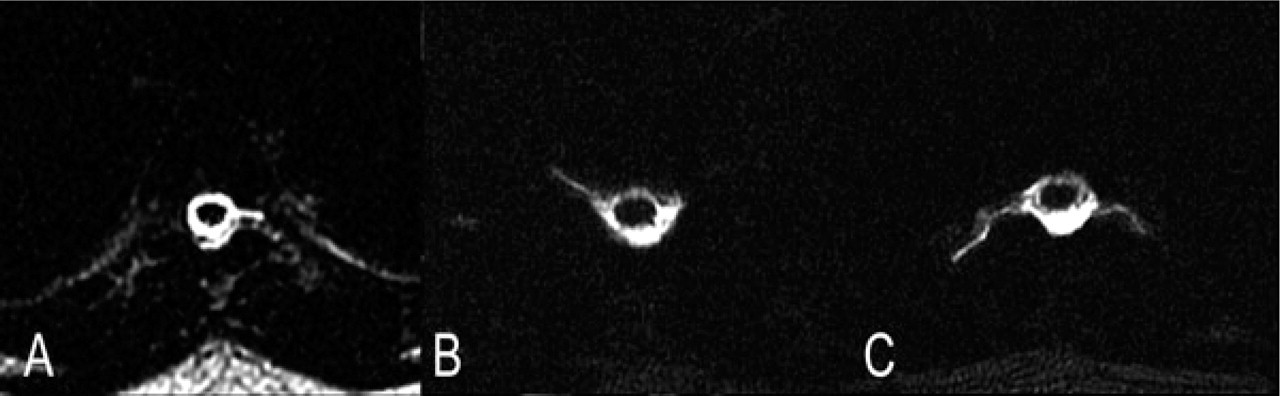
The transverse planes of the magnetic resonance myelogram (A–C) show different appearances of cerebrospinal fluid collections along the nerve roots.
Meningeal diverticulum
Only one patient showed a 2-cm diameter, dumb-bell shape meningeal diverticulum at the right C6–7 level (Fig. 5). However, no other abnormal CSF collections were found in this patient.

The transverse (A) and coronal (B) planes of the magnetic resonance myelogram show a meningeal diverticulum extending from right aspect of the spinal canal to the intervertebral foramen at the C6–7 level.
Dilated perineural cysts
Six patients (35%) showed dilated and rounded perineural cysts, of which most were symmetrical and located in the lumbar region (only one thoracic and one unilateral), with an average number of involved segments of four (range 1–7).
Control subjects
No control subjects showed epidural or extraspinal fluid collections. The percentage of control subjects with perineural cysts (n = 10, 59%) did not differ from that of patients with SIH (n = 6, 35%, P = 0.169). Therefore, dilated perineural cysts were not considered to be abnormal CSF collections.
Treatment efficacy and MR myelography follow-up
Six patients received conservative treatment only and 11 also received EBPs. Two patients received EBP once, six twice, two three times and one patient six times. At the 3-week follow-up, MR myelography was normal in nine patients and abnormal in the other eight. Of the nine patients with normal MR myelography, only one still suffered from orthostatic headache; whereas, of the other eight patients with abnormal MR myelography, two had orthostatic headache and three had non-orthostatic headache. The κ statistics gave a value of 0.52 and the agreement rate was 76%
One patient with SIH suffered from a very protracted course even after three EBPs within 3 months. He was left with intermittent but non-orthostatic neck pain after treatment. However, MR myelography studies at 7 months (fourth follow-up) still showed C1–2 extraspinal leakage, which finally resolved by 15 months (fifth follow-up) (Fig. 3).
Discussion
In this study, heavily T2-weighted MR myelography resulted in a high yield rate (88%) in SIH patients, which was at least compatible with previous invasive methods, such as CT myelography (50%) (6) and radioisotope cisternography (28–100%) (6–10). Based on the ICHD-2 criteria (19), if brain MRI is negative, the diagnosis can be made only with evidence of CSF leakage or with a low opening pressure. In this study, because of the MR myelography results, we were able to meet the requirement and achieve an early diagnosis of SIH in four patients (24%) whose initial brain MRIs were negative. In fact, if brain MRI results are combined, the diagnostic rate was 100% in our study patients.
In this study, heavily T2-weighted MR myelography demonstrated three types of abnormal CSF collections in patients with SIH: (i) high cervical extraspinal fluid collections (35%), (ii) CSF collections alongside the nerve roots (35%), and (iii) epidural fluid collections (88%). These findings can be interpreted as evidence of CSF leakage because none of them was found in our control subjects. However, whether these CSF collections can be used for targeted interventions awaits further study. A high cervical extraspinal CSF collection has been considered as a ‘pseudo-localization’ sign (20). It is hypothesized that, in SIH patients, some undemonstrated CSF leakage sites drain the CSF into a potential epidural space; the fluid flows along this space as a ‘gutter’, to the high cervical region, and then leaks out through the C1–2 space to the extraspinal region (20). In a previous study, 50% of patients with postlumbar puncture headache also had extraspinal fluid collections in the C1–2 region (21). Therefore, C1–2 might not be the actual ongoing CSF leakage site. Accumulations of CSF along nerve roots called ‘irregular nerve roots’ were considered to be an indication of the CSF leakage sites on CT myelography studies due to contrast medium leakage (7, 20, 22). In this study, six patients showed nerve root CSF collections in the lower cervical or upper thoracic levels on MR myelography studies. We considered these nerve roots to be possible ongoing leakage sites because they were located at the most common leakage sites for patients with SIH (2).
The characteristics of heavily T2-weighted MR myelography, i.e. time-saving, no administration of contrast medium and non-invasiveness, make it a useful tool for follow-up studies of patients with SIH, especially when multiple follow-ups are needed. More importantly, the follow-up findings were generally compatible with clinical changes in this study, with a moderate strength of agreement (κ = 0.52). Of note, some SIH patients may lose characteristic orthostatic headaches as the disease becomes chronic (1, 23). For example, one of our patients had a protracted course of SIH even though his symptoms became mild, non-orthostatic and intermittent. The study done at 7 months still demonstrated C1–2 extraspinal leakage.
Our study has confirmed that perineural cysts are not pathogonomic in patients with SIH (17). Their frequency did not differ between patients and control subjects. The characteristics of the perineural cysts were bilateral and involved multiple levels. The shape was rounded with distinct margins. In addition, only one patient demonstrated a meningeal diverticulum, which was considered to be the predilection site of the CSF leak (1, 24). However, her MR myelography did not show any evidence of leakage. Therefore, it was uncertain whether the meningeal diverticulum in this patient was the exact CSF leakage site.
Our study did not set out to determine whether the abnormal CSF collections demonstrated by the MR myelography were the exact CSF leakage sites. This is because MR myelography was not able to demonstrate the dynamic change of CSF flow as detected by conventional myelography, CT myelography or radioisotopic cisternography, in which the contrast medium leakage from the CSF fistula was visible. In order to resolve this issue, further studies should compare MR myelography with standard procedures, e.g. CT myelography, or directly target these abnormal CSF collections with EBP.
In conclusion, this study suggests that heavily T2-weighted MR myelography is helpful in the diagnosis and follow-up of patients with SIH. The clinical significance of different CSF collections detected by MR myelography should be further studied.
Acknowledgements
The study was supported in part by a grant from the Taipei-Veterans General Hospital (V96C1-041), Taipei, Taiwan.