
Abstract
Aims
In this study, we tested the validity of the Severity of Dependence Scale in detecting dependence behaviours in patients with chronic migraine and medication overuse (CM + MO) using the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) and the Leeds Dependence Questionnaire as gold standard measures.
Methods
Four hundred and fifty-four patients with CM + MO filled in the Severity of Dependence Scale and the Leeds Dependence Questionnaire and underwent a psychological evaluation for the diagnosis of substance dependence according to the DSM-IV criteria.
Results
Sixty-nine percent of subjects (n = 313) presented substance dependence according to the DSM-IV criteria. These patients scored significantly higher than those without substance dependence in Severity of Dependence Scale total score (Z = −3.29, p = 0.001), and in items 1 (Z = −2.44, p = 0.015), 2 (Z = −2.50, p = 0.012), 4 (Z = −2.05, p = 0.04), and 5 (Z = −3.39, p = 0.001). Severity of Dependence Scale total score (β = 0.13, SE = 0.04, z = 3.49, p < 0.001) was a significant predictor for substance dependence. Receiver Operating Characteristic (ROC) curves showed that Severity of Dependence Scale discriminated patients with or without substance dependence.
Conclusion
Severity of Dependence Scale could represent an interesting screening tool for dependency-like behaviors in CM + MO patients.
Introduction
Headache is considered one of the most common and disabling neurological disorders (1). In most cases, attacks recur episodically; however, in a small but relevant portion of patients, migraine acquires a chronic pattern (chronic migraine, CM), characterised by at least 15 headache days/month, often associated with overuse of acute medications (MO) (2). Not all patients with CM develop MO and it is yet to be defined with certainty whether medication overuse precedes or follows the progression to CM. Hence, the investigation of the factors of risk to develop CM + MO becomes very important in order to prevent a negative outcome and/or to put in place targeted treatments (3). Current evidence suggests that, besides socio-demographic/lifestyle habits and medical history factors, psychological aspects may also play a relevant role in CM + MO (4,5). CM + MO is indeed strongly associated with anxiety, depression, and personality disorders (6–9), together with childhood traumas, life events, and alexithymia (10,11).
Among psychological factors related to CM + MO, some questions arise from the concept of dependence or dependency-like behaviours (12,13). Some patients show a kind of dependent behaviour from symptomatic drugs, even though the personality characteristics of these patients (and probably the underlying mechanisms) are very different from those of patients with substance addiction (9,14). The presence of a dependency-like behaviour is associated to a negative treatment outcome (15) and this explains the importance of devising reliable tools to assess dependence in the clinical practice. Furthermore, dependence-like behaviour may play a role in the selection of treatment pathways, as withdrawal therapy seems more effective in reducing dependence-like behaviour compared with preventive treatment alone (16).
Two self-administered questionnaires are available to measure dependency-like behaviour. The first one is the Leeds Dependence Questionnaire (LDQ) (17), which is a 10-item instrument to measure substance dependence severity in addiction and psychiatric settings (18,19), but has also been used in CM + MO (20,21). The second tool is the Severity of Dependence Scale (SDS), a brief self-administered five-item questionnaire designed to measure psychological dependence upon a variety of illicit substances (22). SDS has been validated and its cut-off limits have been identified in many settings of abuse, including amphetamine, benzodiazepines, alcohol, cocaine, and heroine (22–26). SDS has recently also been used in the field of medication-overuse headache, where it was shown to be a predictor of MO in samples of primary chronic headache patients from the general Norwegian population (27–29). SDS scores are also able to predict the outcome of detoxification treatment in subjects with MO headache (15). SDS requires a very short time for completion (i.e. <1 min) and it is usually better accepted by patients with respect to other questionnaires for detecting addiction (12,13,30). Furthermore, in the self-reported written version, SDS showed a good correlation with the interview version (31). SDS might therefore qualify as a screening tool prior to headache consultation. The Italian version of SDS has been used in other studies but without a proper validation. For instance, Biagianti et al. (32,33) used it as a control measure when evaluating decision-making processes in CM + MO. To date, no study has validated the SDS as a screening tool for detecting dependency-like behaviors in MO, testing its concurrent validity with respect to other measures of dependence.
The main goal of the present study was to validate SDS in a large sample of patients with CM + MO consulting in an Italian headache specialty centre. To this end, we used the Diagnostic and Statistical Manual of Mental Disorders (DSM–IV) criteria (34) and the LDQ as gold standards to measure dependence.
Patients and methods
This study was conducted from 2017 to 2020 at the Pavia Headache Center (a tertiary referral centre) of the Mondino Foundation in Pavia, Italy. We enrolled patients with CM + MO admitted for the inpatient detoxification program, consisting of the standard CARE in-patient withdrawal protocol described in detail elsewhere (6,35) (including preventive treatment, which was personalised in case of comorbidities and previous prophylactic therapy used by the patient). The study was approved by the local Ethics Committee and written informed consent was obtained from all patients.
CM + MO patients
Inclusion criteria were: a) age ≥18, ≤65 years; b) fulfillment of ICHD-3 criteria (36) for CM and for MO. Exclusion criteria were: a) dementia; b) previous diagnosis of psychosis, and c) mental retardation. An expert neurologist verified the eligibility criteria during the recruitment process based on history, headache diaries, and neurological evaluation.
Procedures
Each consultation was performed by a neurologist that diagnosed the headache type, collected socio-demographic data, migraine characteristics and history, and history of present and previous use of medications. Participants filled in the SDS and the LDQ and underwent a psychological evaluation for the diagnosis of substance dependence according to DSM-IV criteria.
Severity Dependence Scale (SDS)
SDS is a self-completion 5-item questionnaire developed in order to assess the compulsive dimension of psychological dependence. We used the original Italian version of the SDS developed by Grassi and colleagues (37), adapted according to the version by Grande (27). The five questions were as follows: 1) Do you think your use of your headache medication was out of control? 2) Did the prospect of missing a dose make you anxious or worried? 3) Did you worry about your use of your headache medication? 4) Did you wish you could stop? 5) How difficult did you find it to stop or go without your headache medication? Each question applies to the medications taken for the acute treatment of migraine in the past year and it is scored on a four-point scale (0–3). The total maximum score is 15. Higher scores reflect higher dependence. A cut-off score for diagnosing the behavioral addiction for painkillers has been established as greater than or equal to 5 (27).
Leeds Dependence Questionnaire (LDQ)
The LDQ is a self-completion 10-item questionnaire assessing the severity of dependence across a variety of substances, including painkillers. In the present study we used the Italian version, already developed (17). Each item is scored on a four-point scale (0–3), with a maximum score of 30. The total score increases according to the degree of dependence. No cut-off score indicative of dependence has been established (18).
DSM-IV diagnose for dependence
Patients underwent a complete evaluation based on the DSM-IV criteria by expert psychologists (SB and SP) by means of the Structured Clinical Interview for DSM-IV Disorders (SCID-I) (38) in order to diagnose formal substance dependence. The choice of DSM-IV as the gold standard was related to the adoption of these criteria by most studies on this matter. This diagnosis was based on seven criteria. Criteria 1 and 2 referred to the existence of tolerance and previous withdrawal; Criteria 3 to 6 referred to the lack of control over substance use (e.g. intake of larger doses for longer periods, unsuccessful efforts to reduce substance use); Criterion 7 referred to substance overuse. Dependence on acute drugs for headache was diagnosed for those patients who were positive for three or more criteria. Results were dichotomised into substance dependence versus no substance dependence.
Statistical analysis
Statistical analyses were performed using R 4.0.2. Descriptive statistics presented continuous variables as mean and standard deviation, or median and range where appropriate, categorical variables as row counts and percentage. The level of significance was set at 5%. The normality of continuous variables was assessed using the Kolmogorov–Smirnov test. Due to strong deviation from the normal distribution of some variables, non-parametric analysis was performed. Wilcoxon tests was used to test group differences for continuous data. Convergent validity measures the degree to which two measures are related and was assessed using Spearman’s rank correlation coefficient between SDS and LDQ. A correlation of 0.5 or above was considered a good correlation and the related p-value evaluates the statistical significance of the correlation. The reliability of the questionnaire was measured based on its internal consistency using Cronbach’s alpha. As the questionnaire could not be retested with the same users, the split-half method was used. In general, a Cronbach’s alpha score >0.7 is accepted; in our setting we considered a value >0.6 as acceptable due to the small number of items in the SDS. Logistic regression analysis was performed to determine whether the SDS score is a good predictor for substance dependence. The SDS score was considered as a continuous predictor variable and substance dependence as the dichotomous outcome variable of the model. Confounding variables of age and sex were included in the model. The optimal cut-off probability for the model was defined to be the one that yields the lower misclassification error. Performance indexes were evaluated in-sample. Specifically, we considered accuracy, sensitivity, specificity, Receiver Operating Characteristic (ROC) analysis with reference to the Area under the ROC Curve (AUC) index. AUC confidence intervals and tests were performed through the De Long procedure. A cut-off value for the SDS score was selected maximising the Youden index.
A sample size greater than 300 is considered Good and a ratio of 10:1 between subjects and items is suggested, according to all criteria reviewed in Boateng et al. (39).
Results
Patient population
We enrolled 454 subjects with CM + MO. Patients had the following characteristics: 83% were female (n = 376), average age was 47.4 ± 11.7, the average age at onset of migraine was 14.8 ± 8.4, the average duration of chronic headache (in months) was 111.5 ± 98.1; whereas the average duration of MO (in months) was 71.8 ± 76.7. The average number of drug doses per months was 41.0 ± 28.6, the average number of days with medication intake per month was 24.2 ± 5.7, and the average number of days with headache per month was 23.7 ± 7.6. Thirteen percent of the patients overused triptans, 29% analgesics, 9% combination of analgesics, and 49% were poly-drug users. None overused ergotamins or opioids. All patients received a prophylactic treatment: 8% beta-blockers, 25% antiepileptic drugs, 10% calcium antagonists, 33% tryciclics, and 24% polytherapies.
The average SDS total score was 7.0 ± 2.9 and the average LDQ total score was 10.1 ± 6.1. Sixty-nine percent of the subjects (n = 313) satisfied DSM-IV criteria for substance dependence.
Comparison between patients with and without substance dependence according to DSM-IV
When comparing demographic and clinical features (Table 1) between these two groups, we observed older age, W = 25170.50, p < 0.001; higher duration (in months) of chronic migraine, W = 13260.00, p < 0.001; higher duration (in months) of overuse, W = 11104.50, p = 0.001; higher number of doses per months, W = 12918.00, p < 0.001; and higher number of days with medication intake per month, W = 14023.50, p < 0.001, in the patients with dependence when compared to the patients without dependence. No other demographic or clinical differences resulted between these two groups.
Demographic, clinical, and psychological characteristics of CM+MO patients with or without substance dependence according to DSM-IV criteria

SDS and LDQ scores in patients with and without substance dependence
As regards SDS, patients with substance dependence scored significantly higher than those without dependence in the total score, W = 27843.50, p = 0.001; and in item 1, W = 28711.50, p = 0.015; item 2, W = 28720.50, p = 0.012; item 4, W = 29498.00, p = 0.04; and item 5, W = 27787.00, p = 0.001. Groups did not differ in item 3 (p = 0.78) (Table 2).
Total score and score at the individual items of the Severity of Dependence Scale (SDS) and Leeds Dependence Scale (LDQ).
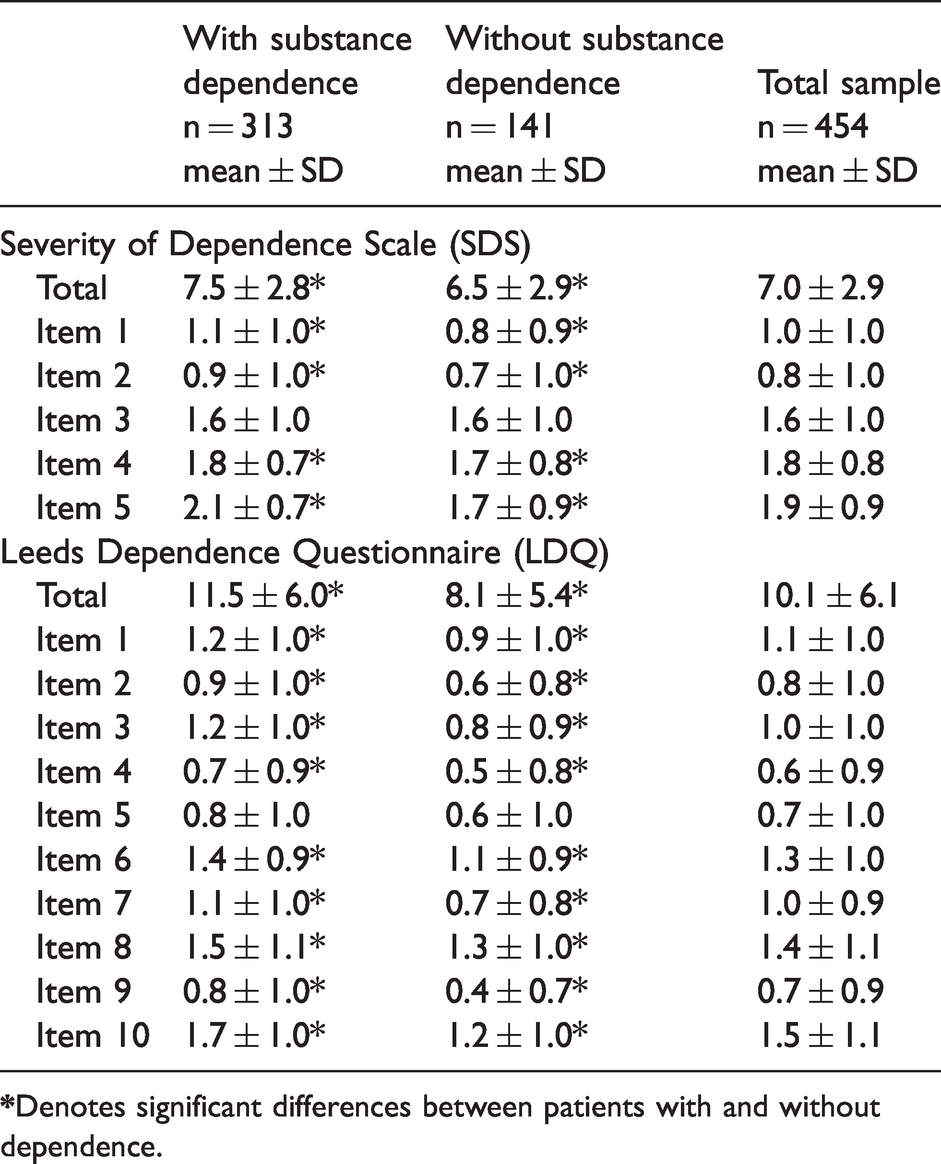
As regards LDQ, patients with dependence scored higher in the total score, W = 25035.50, p < 0.001; and in item 1, W = 28157.00, p = 0.003; item 2, W = 27354.50, p < 0.001; item 3, W = 25709.00, p < 0.001; item 4, W = 28861.00, p = 0.011; item 6, W = 26854.50, p < 0.001; item 7, W = 26627.00, p < 0.001; item 8, W = 28820.50, p = 0.019; item 9, W = 27063.50, p < 0.001; item 10, W = 26136.00, p < 0.001. Groups did not differ in item 5 (p = 0.11) (Table 2).
Convergent validity between SDS and LDQ
As illustrated in Table 3 and Figure 1, significant positive correlations resulted among SDS and LDQ items, as well as between SDS and LDQ total scores, with the only exceptions being SDS item 4 with LDQ items 5 and 6.
Correlations of the Severity of Dependence (SDS) and the Leeds Dependence Questionnaire (LDQ) scores.


Scatter plot illustrating the relationship between the Severity of Dependence Scale – SDS (abscissa) and the Leeds Dependence Questionnaire – LDQ (ordinate) total scores.
Validity analysis
Internal consistency for the SDS items (Cronbach’s α) was 0.61. The half-split reliability was 0.66.
Logistic regression analysis
The SDS total score (β = 0.13, SE = 0.04, z = 3.49, p < 0.001) adjusted for age and sex was a significant predictor for substance dependence.
ROC curves were computed to evaluate the substance dependence sensitivity and specificity of the SDS total score (Figure 2, Table 4). The results show good values for this parameter, which is comparable to the LDQ total score in the ability to discriminate between patients with or without substance dependence.

Receiver operating characteristics (ROC) curve depicting relationship between sensitivity and specificity at different Severity of Dependence Scale (SDS) cut-off scores for predicting substance dependence.
Statistical comparison to determine differences between the Severity of Dependence Scale (SDS) total score and the Leeds Dependence Questionnaire (LDQ) total score in terms of sensitivity, specificity, AUC, and confidence intervals in predicting substance dependence.

p-value = comparison with the SDS total score.
AUC: area under the curve; CI: confidence interval; J: Youden J statistic; SDS total: Severity of Dependence Scale total score; LDQ total: Leeds Dependence Questionnaire total score.
Using a cut off value of 6, the resulting model gave a sensitivity of 76% and a specificity of 40% for predicting substance dependence and correctly identified 65% of patients.
Discussion
The main goal of the present study was to validate SDS, a screening tool to detect substance dependence in a sample of CM + MO patients treated in an Italian headache specialty centre. Our principal finding is that the SDS score showed accurate association with the DSM-IV dependence diagnosis in the ROC analysis and that it resulted comparable to the LDQ. Statistical analysis showed also that SDS has good internal consistency and reliability. To the best of our knowledge, this is the first study carried out on a large sample of patients with CM + MO validating the SDS score against two gold standard measures of substance dependence represented by DSM-IV and LDQ.
Our results show that SDS total score and the score of individual items differed between subjects with and without substance dependence. In particular, we found that the CM + MO patients with dependence scored higher that those without dependence in the total SDS score and in all single items, with the exception of item 3 only.
SDS is a questionnaire created to measure general dependence-like behavior rather than drug-specific physical withdrawal symptoms. In other fields of application (40), it has been highlighted that items 1, 2, and 5 of the SDS explore the emotional and behavioural components of compulsive behaviour, whereas items 3 and 4 were more of motivational nature with respect to the idea of stopping. In this view, our findings underscore a general tendency towards a loss of control over the medications used in the subjects with substance dependence. Other studies showed the existence of a “bio-behavioral” disorder in CM + MO characterised by impulse control disorders and behavioral impulsivity (41–43) resulting in compulsive reward-seeking behavior, active coping attempts for headache and fear of future attacks (44). In this frame, it seems that CM + MO patients may find it difficult to stop using medications, either because of their impaired control or as a consequence of the negative reinforcement to take them for pain relief. Notably, patients with and without dependence had a similar pattern of response to item 3, which explores worries about medication use. The observed moderate level of worry probably reflects the generalised need for painkillers to cope with continuously recurrent attacks.
Sixty-nine percent of the 454 CM + MO patients taking part in this study were found to be dependent on a substance according to DSM-IV criteria. Such a proportion is in perfect line with previous studies on this topic with CM + MO patients recruited from headache clinics in other countries (12,13). Slightly lower proportions of substance dependence were observed when patients were recruited from the general population (15), suggesting that patients seeking help in specialised centres are more complicated.
The assessment of dependency-like behaviors via the SDS showed good correlation and agreement with LDQ, both in terms of global scores and – in most cases – of single items. These findings suggest the opportunity to use SDS in the clinical practice as a very quick self-administered screening tool. Of course, SDS can be associated to LDQ if a more thorough evaluation is desired. In analogy to the study carried out by Ferrari (17), we use LDQ in a sample of CM + MO patients, but we took a step further by also evaluating our patients with the DSM-IV criteria for the diagnosis of dependence. What is interesting here is that, even if the overall LDQ score in our population was similar to Ferrari’s study (11.6 ± 6.4 and 10.1 ± 6.1, respectively), the score dramatically changes in our study when considering the two sub-groups with/without dependence (11.5 ± 6.0 vs. 8.1 ± 5.4, respectively). This finding is very interesting as it suggests the importance of further differentiating this complex group of seriously affected patients in different subtypes.
A still open and debated question is whether CM + MO should be regarded as a real substance dependence (45) or rather as a dependency-like behavior in which the overuse of medication is solely motivated by the need to control the intensity of a debilitating headache (46). Clinical, pathophysiological, and genetic evidence (47) suggests the presence of a behavioral disorder of dependence that manifests itself as an impaired control over the medication use and plays a role in promoting and maintaining CM + MO. For instance, LDQ scores were found to be similar in chronic daily headache and drug-addicted patients (17). However, other studies suggested the existence of two different subgroups of CM + MO patients: Those with substance dependence and those without. This subdivision also seems relevant in the view of the outcome of withdrawal from overused drugs (e.g. 15,16,20,29). Accordingly, patients fitting these two different profiles should receive two different approaches of treatment. We believe that such a consideration should also be analysed in the view of the country of origin. For instance, overuse of barbiturates and opioids is common among CM + MO patients in the USA (47). A large Chinese study (12) reported a quite substantial amount of ergotamine users in CM + MO. In the present study, no patient reported overuse of opioids or ergotamine, and the types of overused medications did not differ among patients with or without substance dependence diagnosis. Hence, future studies are needed in order to further explore the link existing between the different pharmacological mechanisms and the “dependence” topic in CM + MO.
This is the first study using SDS to assess dependence from medications in a large sample of Italian CM + MO patients. According to our findings and to the concurrent validity with respect to LDQ and DSM-IV, SDS proved to be a valuable tool able to reliably detect dependency-like behaviors. Given its ease and quick format, it can be easily adopted routinely in all those settings where time for visiting patients is limited. Hence, it could be used as a screening tool by general practitioners in order to select patients taken from the general population that should be referred for specialist treatment. Even if we tested SDS in patients seen in a headache specialty center, there are many successful experiences of its use in the general population of headache sufferers (e.g. 15,28,29). Furthermore, SDS could be used during headache consultations in order to help clinicians in delivering more precise treatment strategies. In particular, CM + MO patients with high SDS scores should be considered for in-patient withdrawal treatment, given that they are less likely to benefit from out-patient withdrawal (32). These patients should be also considered as best candidates for the integration of cognitive behavioral therapy into a standard withdrawal program. By contrast, patients with low SDS scores may undergo detoxification as out-patients (35).
There are some limitations that should be noted. First, this study enrolled CM + MO patients taken from a specialised headache centre. Hence, they might not be representative of the general population of CM + MO. However, it is important to consider that, even if this study was performed on a selected clinical population, it is characterised by a large sample. Second, given the large population recruited, the enrolment in the study started in 2017. Thus, it is possible that some uncontrolled variables were introduced during the long enrolment. Third, our study used the DSM-IV criteria for substance dependence instead of those for substance use disorders (SUD), introduced by the more recent fifth edition of DSM. In fact, such a revision combined both substance abuse and substance dependence into a single continuum, which is defined as SUD. In particular, the consideration of those criteria referring to the concept of “impaired control”; that is, criteria from 1 to 4 of DSM-V, should further shed light on this topic. Future studies should better explore this issue. In any case, the use of DSM-IV criteria allowed us to compare our findings with those from the existing literature, given they used the same criteria (12,13,15). Another interesting future development in this area could be to distinguish the dependence habitus from the compulsive behaviors by using instruments such as the Yale-Brown Obsessive Compulsive Scale (Y-BOCS) (48,49).
In conclusion, our findings support the use of SDS in the screening of dependency-like behaviors in CM + MO. SDS use will contribute important information on the factors involved in CM + MO occurrence and is critical to further differentiate this complex group of seriously affected patients in different phenotypical and/or endotypical subtypes.
Clinical implications
SDS could be used in the screening of dependency-like behaviors in CM + MO. SDS can be easily adopted routinely in all those settings where the time for visiting patients is limited
Footnotes
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: [Zenodo; 10.5281zenodo.5145269]
Acknowledgements
This study was supported by a grant from the Italian Ministry of Health to C. Mondino National Neurological Institute (Current Research 2017-2019).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Research Grant from the Italian Ministry of Health to IRCCS Mondino Foundation (Ricerca Corrente 2017-2019).