
Abstract
Background
The economic burden of headache in European countries is substantial, mostly related to indirect work-productivity loss costs, yet data for Portugal is scarce.
Methods
An anonymous web-based survey of headache was distributed to a convenience sample of Portuguese companies’ workforces, to assess last-year headache and “yesterday”-point prevalence. Preexisting headaches were classified into migraine and non-migraine headache and work impact (absenteeism and presenteeism) was evaluated in relation to point prevalence. If no significant selection biases were detected, projected work-loss costs for the whole country were to be calculated.
Results
Eleven (17%) of 65 invited companies participated, around 15,000 active workers were exposed to the survey and 3624 (24.3%) responded, 73% females, 84.3% with previous (“last-year”) headaches, 53% with migraine. Due to participation and gender bias, national cost-projections were not calculated. Workday point-prevalence was 21% (migraine) and 9% (non-migraine headache), resulting in 14 employees with migraine losing, on average, 4 h and 32 min of work time. Presenteeism occurred in 29% of migraine and 15% of NMH employees. Yearly cost of each employee with a headache disorder was €664.88.
Discussion
Headache has a significant economic burden, as measured by work loss costs, in Portugal. Company-based interventions should aim to support employees’ access to headache diagnosis and treatment, including non-pharmacological coping strategies, in order to reduce headache related economic costs.
Introduction
Migraine is the first worldwide cause of years lived with disability in under-50s (1). However, data evaluating the economic burden of headache in Europe is scarce and outdated (2–4).
The most relevant part of economic burden attributed to headache disorders is the cost of attack-related productivity loss, estimated to account for 79% (5) to 93% (2) of total headache-related costs. No standard method has ever been agreed on to quantify the time of work lost, or its monetary value, due to any disease (6). While it is fairly straightforward to consider objective data, such as absenteeism, and its cost, the total time the employee has been unable to work is not accounted for. Several instruments have been developed aiming to objectively measure productivity reductions during active work hours (presenteeism) but few have been adequately validated (6) and may be unreliable since they were based on retrospective assessment of impairment (7) (and thus sensitive to recall bias), neglected the socio-political context (6) and specific work environment and seem to underestimate lesser degrees of disability (7).
The 2010 economic impact study of the European Brain Council (EBC) evaluated costs all major neurological disorders in the European Union (EU) 27, estimating a total annual cost of €43.514 million in purchasing power parity
Two cross-sectional studies specifically targeted the economic impact of headache (Eurolight project) (2) and migraine (International Burden of Migraine Study, IBMS) in some European countries, but no data from Portugal was obtained. The IBMS was an international cross-sectional open web-based survey focused exclusively on migraine direct-cost estimation. Eligible participants were assessed by a set of validated questions based on ICHD-2 diagnostic criteria for migraine (9) and migraine frequency; health-care resources utilization was prompted for the preceding 3 months and pharmacological interventions for the preceding 4 weeks, to minimise recall bias (10). In this study, an individual annual cost of €2,422.11 for chronic and €793.22 for episodic migraine was estimated, with relevant differences found across countries (3).
The Eurolight study, a questionnaire-based study applied in different healthcare settings across countries (2,11), estimated an annual cost of headache at €173 million, and €111 million (64%) attributed to migraine (2). Headache prevalence (lifetime, last-year and point-prevalence, was assessed by asking about “headache yesterday”), headache diagnosis, and impact. Information about resources and drug utilisation and impact on productivity were used to estimate costs (12). One of the strengths of this bottom-up approach is that it used a societal perspective where costs are considered irrespective of the financer. In this study, the impact of recall bias on indirect cost estimation was reduced by using the productivity impairment related to “headache yesterday” (2,12). Some limitations of the study include the used of an extensive time-consuming questionnaire, which increases attrition and endangers data quality, and there was significant heterogeneity in healthcare settings among the different countries (11).
The absence of specific data on headache related economic costs in Portugal prevents accurate planning public and private health expenses on this common neurological disorder. To fill in this literature gap, we performed a nation-wide evaluation of indirect costs attributed to headache and migraine by surveying a convenience sample of Portuguese companies with a methodology based on the Eurolight project. The secondary objective was to use the obtained data to project headache and migraine economic impact on the active workforce at the national level.
Methods
Our method was tested in a pilot study (13) and consists of providing an anonymous web-based survey of headache impact to the active Portuguese workers through their companies’ websites. A convenience sample of Portuguese companies from all sectors was invited to participate according to the following inclusion criteria:
Having >100 active workers, of which >50 had access to a company intranet or institutional email. We excluded small-sized companies to avoid any chance of identification of any employees’ responses based on age and gender data.
Having the acceptance and cooperation of the board of directors and human resources (HR) manager of each company to implement the study protocol and provide some HR information (total number of employees exposed to the link, their average age and rough gender distribution and the groups’ gross average hourly income (optional)).
The online survey link was made available by email diffusion or on the companies’ intranet for eight consecutive days; a warning email or ad was sent 24 h before survey closure. Participation was promoted by an introductory text explaining the study, which was improved from the pilot (13) by eliminating the focus on headache to promote wide participation. Participation was anonymous and voluntary; no identification data (other than age and gender) was prompted.
Survey questions were adapted and simplified from the Eurolight Study (12) with due authorisation; screening questions were about lifetime headache and last-year headache prevalence; only those with headaches last year (sample) were exposed to headache characterisation questions. Preexisting headaches were classified into migraine or non-migraine headaches (NMH) with ID-Migraine (14) (migraine if ID-Migraine score was ≥2) and, in episodic (<15 days) or chronic ((≥15 days) according to last-month frequency.
To avoid recall bias, headache work impact (absenteeism and productivity loss/presenteeism) was determined in relation to a single headache episode, if it occurred the day before the survey (“headache yesterday”), which was taken as a point prevalence measure (13). Work-related point-prevalence considered only headaches that had occurred on a work day. Absenteeism was quantified in hours of work lost; productivity loss was determined as the ratio between employees that completed less than half or nothing of their work divided by those who had “headache yesterday”, as defined by Steiner et al. (15). Production loss costs were calculated for each company considering the average hourly wage provided by the companies’ HR; if data was unavailable, a sample average was used.
We did not evaluate employee’s turnover or replacement costs, as only those who were actively working were surveyed, or the impact of any employee production loss on workgroup dynamics and global productivity (7) and will assume those to be null for the cost estimations.
To estimate direct headache-related costs, subjects were questioned about healthcare resources use in the previous year. Cost attributed to this were retrieved from the Portuguese Health System price list (€31.00 for an outpatient follow-up visit, €51.00 for a basic emergency visit and €67.00 for a brain CT scan (16)).
Projections of indirect costs (absenteeism and presenteeism) for the total Portuguese workforce (17) were planned to the made separately for migraine and NMH using working-day point prevalence for each diagnosis as accessed from our samples’ data and indirect costs calculation considering the average Portuguese gross hourly-wage (18). We did not plan to include direct costs in the country-wide estimations.
Our objective was to survey at least 10,000 of these companies’ employees, hoping for a 10% response rate to include at least 1000 valid survey responses, which would allow us to obtain a 99% confidence level with a 5% confidence interval for the total Portuguese workforce (17). Data analysis used SPSS v20 and included descriptive statistics and Student’s t and chi-square tests, applied as appropriate in group comparisons. Alpha was set at 0.050.
This study was approved by the Hospital da Luz Institutional Review Board and authorised by the data protection officer. Each companies’ board of directors approved its application in their respective companies.
Results
1. Study sample and population
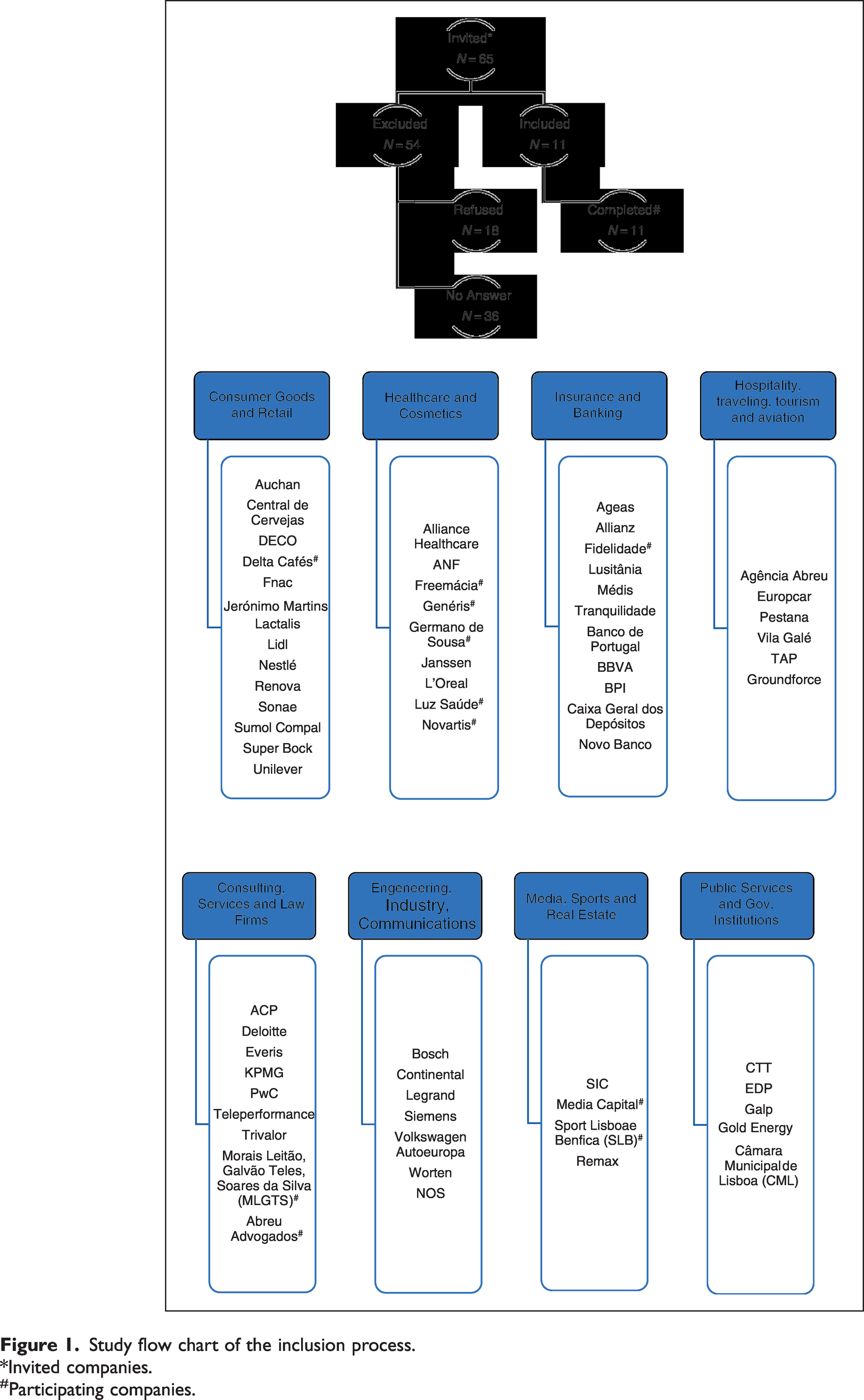
Sixty-five national companies were invited to participate from the several economic activities yet only 11 (17%) were included, five healthcare-related (Luz Saúde, Germano de Sousa, Freemácia, Generis and Novartis), one insurance group (Fidelidade), one media company (Media Capital), one coffee company (Delta Cafés), one sports club (Sport Lisboa e Benfica) and two law firms (Morais Leitão, Galvão Teles, Soares da Silva & Associados and Abreu Advogados). Altogether, these companies employ around 24,000 collaborators, from which 14,888 were exposed to the survey link (Figure 1); those who weren’t had no access to a company intranet or institutional email or were on sick leave or vacation at the time the survey was conducted.

Study flow chart of the inclusion process.
The total number of respondents was 3624, 24.3% of the exposed sample (Table 1), representing the surveyed universe with a 99% confidence level at 1.86 confidence interval.
Included companies, response rates and productivity loss.
NI: No Informtion.
Most respondents were females 73.2% (2654), with an average age of 40.7 ± 10.7 years, ranging from 19 to 73 years old. The sample had more female responders than the surveyed population (73.2% vs. 59.9%, p < 0.0001) and women were younger than men (39.8 ± 10.5 vs. 43.3 ± 10.8 years, Student’s t test 8.822, p < 0.001). Seven (0.2%) respondents were excluded for providing only demographic information, six females (85.7%) with an age average 35.6 ± 10.3 years (Table 1).
2. Headache occurrence
Lifelong headache incidence was 89.8% (3249); the total sample considered for this study included only those with headache in the last year – 3050 (84.3%), of which 2716 (75.1%) had at least one headache episode in the last month.
In all instances, females were more likely to suffer from headache than males, lifelong prevalence of 93.2% versus 80.7%, (χ2 120.586, p < 0.0001), last-year prevalence of 96.3% vs. 85.9%, (χ2 111.322, p < 0.0001) and last month prevalence of 96.6% vs. 84.1%, (χ2 58.498, p < 0.0001).
One thousand six-hundred and thirteen respondents had migraine, 52.8% of those with headache in the last year. Staff with migraine were more often females (85.4% vs. 14.6%, χ2 111.375, p < 0.0001) and younger than those with NMH (38.5 ± 9.9 vs. 41.1 ± 10.6, Student’s t test 6.974, p < 0.0001).
Headache average monthly attack frequency was higher in migraine than NMH employees (4.9 vs. 2.6 days, Student’s t test −14.232, p < 0.0001); chronic headache was identified in 144 (5.3%) of the individuals with headache in the last month, more often in migraine (115, 7.5%) than NMH (29, 2.4%, χ2 34.220, p < 0.0001).
Point-prevalence of headache (“headache yesterday”) was 17.1% (552), migraine occurred more frequently than NMH (77.9% vs. 27.8%, χ2 113.699, p < 0.0001). Of those, 466 (84.4%) headaches occurred in one working day, resulting in point prevalence on working days of 15.3%, 21.0% (339) for migraine and 8.9% (127) NMH.
3. Impact on productivity
Absenteeism due to “headache yesterday” was reported by 14 employees (0.46% of the total sample), all had migraine (3.5% vs. none with NMH, χ2 5.196, p = 0.023). The average time of absence from work due to migraine was 4 h and 32 min ± 2 h and 53 min (ranging from 1 to 8 hours); five employees (35.7%) missed a full day of work and two (14.3%) more than a half-day.
Chronic migraine was not associated with higher point absenteeism than episodic migraine (2.7% vs. 2.6%, χ2 0.004, p = 0.949, ns) nor with more time lost at work (5 h and 15 min vs 4 h and 25 min, p = 0.720, ns).
Three additional employees reported missing work the day before, but not because of a headache – one due to another health problem and two for personal reasons – on average for 3 h and 20 min ± 1 h and 9 min (from 2 to 4 h) of absenteeism, in which two employees (66.7%) missed a half-day’s work.
All causes considered, 17 employees missed work the day before, which represents 0.6% absenteeism, 82.3% of which was due to migraine.
Productivity was affected by headache in 310 (59.4%) of those who had headache the day before, 253 (54.3%) of which occurred within a working day. One hundred and fourteen employees reported having completed less than half or none of the work planned for that day, which resulted productivity losses (15) between 0 to 38.1% in different companies, with an average of 24.46% in the total sample (Table 1).
Employees with a headache disorder who reported having completed less than 50% of their planned work during their attack more often had migraine (29% vs. 15.2% with NMH, χ2 11.348, p = 0.001). Having chronic or episodic headaches (irrespective of diagnosis) had no influence on the ratio of employees that completed less than 50% of their planned work (25.3% vs. 27.0%, χ2 0.098, p = 0.755).
4. Healthcare use in the last year
Health care use for headache evaluated in this sample included outpatient visits in 366 (12%), ER visits in 147 (4.8%) and brain scans in 142 (4.6%) of employees in the last year.
Employees with migraine were more likely to have had an outpatient visit (25.2% vs 5.6% NMH, χ2 160.496, p < 0.0001), an ER visit (10.1% vs. 2.2% NMH, χ2 58.512, p < 0.0001) and a brain scan (9.7% vs. 2.2% NMH, χ2 54.368, p < 0.0001) than employees with non-migraine headache; the same was true for employees with chronic compared to episodic headache or migraine – outpatient visits 44.6% versus 15.9% (χ2 75.254, p < 0.0001), ER visits 18.7% versus 6.2% (χ2 32.009, p < 0.0001) and brain scans 19.4% versus 6.1% (χ2 36.843, p < 0.0001).
Employees with absenteeism due to headache yesterday were more likely to have had an outpatient visit (57.1% vs. 26.3%, χ2 9.522, p = 0.009), an ER visit (35.7% vs. 11.8%, χ2 9.823, p = 0.007) but not a brain scan (21.4% vs. 11.5%, χ2 3.743, p = 0.154, ns) in the previous year than those whom were able to work, despite having had headache the day before.
5. Cost estimations
5.1 Cost evaluation in our sample
Direct costs with headache of this sample in the last year added up to €28,357.00, including 366 outpatient visits (€11,346.00), 147 ER visits (€7497.00) and 142 brain scans (€9514.00). Considering our total sample of employees with a headache disorder, the average yearly direct cost, per headache of employees with a headache disorder, is €9.30.
Absenteeism costs of headache in this sample relate to a total of 60 h and 30 min of work lost due to headache in a single day, an estimated total daily cost of €608.71, adding up to €146,090.40 in each full 240-day working year (Table 1). The average yearly absenteeism cost, per employee with a headache disorder, is €47.90.
The total wage cost of headache in this sample was €7722.59, adding up to €1,853,421.60 (€1.8 million) per 240-day working year (Table 1). The average yearly absenteeism cost, per employee with a headache disorder, is €607.68.
All costs considered, yearly cost of each employee with a headache disorder in this sample is €664.88 (€9.30 direct costs + €655.58 indirect costs). Considering the total sample of 3050 employees with a headache disorder, these companies lose €2,027,884.00 (€2 million) per year, due to headache – €8449.51 per day.
5.2 Indirect cost projections for the total Portuguese workforce
We decided not to extrapolate our data for the total Portuguese workforce, since there was a significant participation and gender bias likely to lead to inaccuracy of this estimation.
Discussion
This is the first nation-wide study to estimate the cost of headache and migraine in Portuguese companies, hoping to raise awareness for the huge impact of these disorders beyond patients’ suffering, in their professional dynamics and to their companies’ productivity. We collected data on headache and migraine costs in a sample of the Portuguese workforce, including part of the direct cost (healthcare resource utilisation, not treatment-related costs) and most of the tangible indirect costs (absenteeism and presenteeism).
Workday point-prevalence of headache in this sample was 15.3% (21.0% migraine, 8.9% NMH), identical to that assessed in the pilot study (13) and lower than that reported in the Portuguese population study (19) of 23.3%. Our value is in line with the European population average of 17.2%, although there was significant international variability, values ranging from 11% in Lithuania to 25% in the UK (20). Differences to population studies are expected, as age-range and health status of our sample differs by including only active workers. As point prevalence is influenced by disease activity, our sampling method will exclude highly disease-impacted individuals, who are more likely to be on sick leave or to have lost their jobs due to headache and/or other health-related conditions (21). On the other hand, it will also exclude older healthy retired individuals, who are expected to have lower headache and migraine prevalence and lower attack frequencies (22). Considering all these factors, we trust our point-prevalence to be a fairly accurate estimation.
Data from our sample demonstrates a yearly cost for each employee with a headache disorder of €664,88 (€9.30 direct costs + €47.90 absenteeism + €607.68 productivity loss). Considering the total sample, in these companies €2 million is lost per year due to headache and migraine.
Chronic headache, in our sample, had the same impact on absenteeism and presenteeism as episodic migraine, as was expected because these metrics were evaluated in relation to a single headache day. Our data supports, as was previously recognised in the previous European study (11), migraine having more work-related impact than NMH.
Our sample size was adequate for the universe of the companies included but not representative, as there was a gender-response bias driven by the fact that women are more affected by headache and migraine (23), are more prone to report poor health status (24) and are more interested in health-related information (25). This bias probably overestimates the prevalence and impact of migraine headache in our sample and was already detected in the pilot study (13). Efforts to overcome it were made by re-writing the surveys’ invitation text; this improved the participation of non-headache sufferers, as our samples’ life-long (89.8%) and last-year (84.3%), prevalence were equivalent to those described in a Portuguese population study of 88.6% and 85.7% (19). Migraine, however, was present in 52.8% of our sample, a higher value than the expected 9.9% (19) from the populational study, so our efforts were not enough to correct the gender and participation bias towards migraine sufferers. Two additional factors might explain this difference: a) The use of ID-migraine (14) as a diagnostic tool, which has a sensitivity of 0.94 yet only 0.60 specificity for migraine diagnosis, contributing to migraine overdiagnosis; b) the Portuguese population prevalence data is not up to date, as the only Portuguese population study is a doctoral thesis dating back to the early 1990s (19), just after the first version of the ICHD was published (26).
As our sample was a non-probability convenience sample, it was also not representative of the total Portuguese workforce as it including only medium to large-sized companies, which mostly had highly educated professionals (business executives, health-related and clerk-like or administrative) with higher than average incomes – the average hourly income of our sample was 68.9% higher than the national average and represented a gross estimation, without proportional evaluation for different working categories and incomes. In sum, the cost of headache and migraine in our sample is most probably overestimated, which prevented the generalisation of results to the total Portuguese workforce, so we have not met our secondary objective due to unadjustable bias.
In the Eurolight study, total annual costs for headache varied in different countries, from over €20,000 million in Spain, Italy, Germany, and France to less than €1,000 miillion in Luxemburg and Lithuania; Austria, which has the closest population size to Portugal, had a yearly cost of around €3,000 million, 0.75% of its 2019 GDP.
All these values ignore work-related intangible costs – the loss of productivity related to increase entropy of work teams that occurs when a core worker underperforms due to headache is an example; others include the fear of being misunderstood by co-workers when experiencing an attack, which can contribute to a work environment of mistrust and poor team performance, and even personal disengagement, fueled by headache sufferers’ perceptions of the impact of headache on their performance, career and work progression (27). Also, it does not account for non-market production (household or volunteer work, informal care and so forth) or other personal intangible costs, due to pain, suffering and social isolation.
In sum, in the screened companies the cost of headache and migraine was high, around €2 million yearly, 87% of which related to productivity loss. Companies, probably more effectively than national health systems’ policies, could be motivated to identify and better understand these patients’ limitations and become more flexible, learning to adjust to migraine and headache-related transient impairment, as the majority of patients will try to compensate for lost work (13).
Occupational medicine teams could introduce headache-impact evaluation in their routines and have the ability to establish a clinical diagnosis of migraine and to use this type of survey to all employees, therefore overcoming all the observed bias in this study. Data obtained could be used to establish a company-based approach to set in place treatment strategies and working-condition adjustments in order to reduce headache and migraine economic impact, while improving individual patients’ lives.
Public health relevance
Work productivity was affected in 54.3% of the employees in a large sample of an active work force population during a headache attack. Yearly indirect costs projected for headache in the surveyed companies add up to €664.88 per employee with a headache disorder. A company-based approach both offering adequate access to diagnosis/treatment and supporting non-pharmacological coping strategies may increase headache patients’ productivity and can contribute to significant cost reductions.
Footnotes
Authors' contributions
RGG and RM are responsible for the study design, study implementation and review and approval of the final manuscript; RGG is responsible for statistical analysis and manuscript draft.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received support from the Portuguese Headache Society (SPC)-Novartis grant. Part of this data was publicly presented as a Public Health Masters’ thesis by RM on 5 February 2020.
Ethical approval
The study protocol was approved by the Institutional Review Board and Data Protection Officer of Hospital da Luz. Each of the participating company’s administration board also approved the study implementation.
Availability of data and material
Any data not published within the article will be shared, anonymised, by request from any qualified investigator.
Acknowledgments
The authors acknowledge the help from each of the participating companies HR management staff, and of Nuno Silva and Gonçalo Luís, from Learning Health, for setting up the on-line survey and monitoring the database safety. We would also like to thank António Gouveia Oliveira for helpful critical input to the final manuscript and Ruth Geraldes for the English review. We would also like to recognise the commitment of a reviewer who was tireless in their efforts to ensure that the manuscript achieved the quality necessary for publication.