
Abstract
Background
Few studies of migraine have evaluated migraine disability across multiple countries using the same methodology.
Methods
This cross-sectional, web-based survey was conducted in 2021–2022 in Canada, France, Germany, Japan, UK and USA. Respondents with migraine were identified based on modified International Classification of Headache Disorders, 3rd edition, criteria. Headache features (Migraine Symptom Severity Score (MSSS, range: 0–21), presence of allodynia (Allodynia Symptom Checklist, ASC-12)) and migraine burden (Patient Health Questionnaire-4 (PHQ-4), Migraine-Specific Quality of Life questionnaire version 2.1 (MSQ v2.1), Work Productivity and Activity Impairment (WPAI) questionnaire) were evaluated.
Results
Among 14,492 respondents with migraine across countries, the mean ± SD MSSS was 15.4 ± 3.2 and 48.5% (7026/14,492) of respondents had allodynia based on ASC-12. Of all respondents living with migraine, 35.5% (5146/14,492) reported moderate to severe anxiety and/or depression symptoms. Mean ± SD MSQ v2.1 Role Function–Restrictive, Role Function–Preventive and Emotional Function domain scores were 60.7 ± 22.9, 71.5 ± 23.0 and 65.1 ± 27.2, respectively. The WPAI mean ± SD percentages of respondents who missed work or worked impaired as a result of migraine were 6.8 ± 18.1% and 41.0 ± 30.1%, respectively.
Conclusions
For every country surveyed, migraine was associated with high levels of symptom severity, with allodynia and with substantial burden.
Keywords
Introduction
Migraine affects over one billion people worldwide and is the leading cause of years lived with disability in people aged 15–49 years (1,2). Additionally, migraine is associated with negative effects on daily functioning, health-related quality of life (HRQoL) and work productivity (3–7). For example, in the US-based Chronic Migraine Epidemiology and Outcomes (CaMEO) Study, headache-related disability, psychiatric comorbidities, and financial and occupational burden were observed in many people living with migraine (6). The Eurolight project highlighted the association between depression, anxiety and migraine in 10 European countries (8). The results from the International Burden of Migraine Study (IBMS) demonstrated high levels of headache-related disability in Australia, Canada, France, Germany, Italy, Spain, UK, Taiwan and USA (7). Although the Eurolight project and IBMS confirmed the burden associated with migraine in multiple countries, studies differed in methods and timing; few other studies have been conducted to establish headache-related disability across multiple countries.
The CaMEO–International (CaMEO-I) Study (9) surveyed people with migraine from six countries and was conducted in 2021–2022 as a follow-up to the CaMEO Study (6), which was conducted almost a decade earlier. The objective of the current analysis was to describe headache features and disability, including depression and anxiety symptoms, associated with headache among people with migraine from the CaMEO-I Study.
Methods
Study design
CaMEO-I was a cross-sectional, web-based survey conducted in 2021–2022 in Canada, France, Germany, Japan, UK and USA, as detailed elsewhere (9). Respondents with migraine were identified based on modified International Classification of Headache Disorders, 3rd edition (mICHD-3), criteria by responses to the American Migraine Study/American Migraine Prevalence and Prevention Study (AMS/AMPP) migraine diagnostic questionnaire (10,11). The AMS/AMPP migraine diagnostic questionnaire is labeled as assessing “modified criteria” because it does not assess two of the ICHD-3 criteria; ≥ 5 lifetime migraine events and duration of attack untreated from 4 to 72 h were not confirmed. The questionnaire itself is validated for assessing migraine and chronic migraine.
Data collected from respondents with migraine included headache features as assessed by the Migraine Symptom Severity Score (MSSS) and Allodynia Symptom Checklist-12 (ASC-12). Patient-reported outcomes were evaluated based on the Patient Health Questionnaire-4 (PHQ-4), Migraine-Specific Quality of Life questionnaire version 2.1 (MSQ v2.1) and Work Productivity and Activity Impairment (WPAI) questionnaire, as described below. When validated translations were available, they were used. Otherwise, surveys were translated from English into each country's language and reviewed by local speakers and the CaMEO-I investigator from each country when applicable. Based on feedback from native speakers who met the symptom criteria for migraine, verbiage and content of the survey were adjusted. Before participant recruitment, a central institutional review board or ethics committee reviewed and approved the study design.
Subsequent to the CaMEO Study being conducted, there have been many novel insights on the migraine disease state, which prompted changes to the questionnaire for CaMEO-I. One of the goals for conducting CaMEO-I was to explore areas that were not well understood, including allodynia, stigma and cognitive function.
Study population
Respondents were selected from large panels established in each country by Dynata (Shelton, CT, USA) based on specific demographics and socio-economic makeup. Respondents who were aged ≥18 years, met modified criteria for migraine consistent with the mICHD-3, could read and understand the national language of their country of residence, and provided informed electronic consent were eligible to participate in this study. A sample representative of each country was invited electronically to participate in the survey. Those who completed the survey were compensated by a small financial incentive.
Assessments
Headache features
The MSSS incorporates information about seven cardinal headache features and one additional item on visual aura (12). Data on the frequency of unilateral pain, pulsatile pain, moderate or severe pain intensity, pain with routine activities, nausea, photophobia and phonophobia were collected through the survey. The MSSS response options and scoring are: never (0), rarely (1), less than half the time (2) and half the time or more (3). The overall MSSS ranges from 0 to 21, with higher scores indicating greater severity of symptoms.
The presence of allodynia was assessed using the Allodynia Symptom Checklist-12 (ASC-12), which is a 12-item questionnaire that evaluates the frequency of various allodynia symptoms associated with headache attacks (13). For each item, the response options and scoring are: does not apply to me (0), never (0), rarely (0), less than half the time (1) and half the time or more (2). Those who reported mild (scores 3–5), moderate (6–8) or severe (≥ 9) allodynia were considered to have the presence of allodynia.
Patient-reported outcomes
Symptoms of depression and anxiety were assessed using the PHQ-4, a four-item depression and anxiety symptom screener (14). The PHQ-4 total score ranges from 0 to 12. A score of ≥ 3 for depression or anxiety symptoms suggests the presence of depression or anxiety symptoms, respectively. Respondents indicated the frequency of problems associated with anxiety and depression symptoms over the prior two weeks with the following response options and corresponding scores: not at all (0), several days (1), more than half the days (2) and nearly every day (3).
Quality of life was evaluated using the MSQ v2.1, which is a 14-item questionnaire that measures the effect of migraine on daily functioning across three domains (Role Function–Restrictive (RFR), Role Function–Preventive (RFP) and Emotional Function (EF) over the last four weeks (15). Each of the 14 items has the following response options and corresponding scores: none of the time (1), a little bit of the time (2), some of the time (3), a good bit of the time (4), most of the time (5) and all of the time (6). MSQ v2.1 rescaled scores range from 0–100 with higher scores indicating better HRQoL (16).
Rates of presenteeism, absenteeism, and lost productivity were assessed via the WPAI questionnaire. The WPAI is a validated instrument that evaluates the impact of migraine on work productivity and regular activities (17). Respondents who reported currently working for pay entered the number of work hours missed for headaches and rated how headaches affected their productivity while working over the previous seven days.
Statistical analysis
Statistical analysis was performed using SPSS, version 29.0 (IBM Corp., Armonk, NY, USA). Missing data were prevented by the electronic survey platform, which required each question to be completed before displaying the next question; therefore, no data imputation was performed. Descriptive statistics were used in this observational study. Mean ± SD values were generated for MSSS, MSQ v2.1 domain scores and WPAI domain scores. Counts and percentages were used to describe all other variables. Pooled estimates for the countries included in the study were generated from computed results for each individual country, with countries weighted uniformly, justified by the approximately equal sample size from each country. National sample sizes ranged from 2382 (Canada) to 2464 (France).
Results
Baseline characteristics
This analysis included 14,492 respondents with migraine, including about 2400 people in each of six countries. Baseline demographics of the sample by country have been published previously (9). Briefly, the mean age was 41.7 years and the majority of respondents were female (71.2%; 10,318/14,492). The percentage of respondents with a body mass index of 30 kg/m2 or greater was 22.6% (3280/14,492), with the highest proportion of respondents identified in the USA (33.8%; 812/2404) and the lowest proportions in France (16.6%; 408/2464) and Japan (5.4%; 130/2409). The percentage of respondents who were currently using a preventive treatment for migraine was 11.2% (1625/14,492).
Headache features
MSSS
Among all respondents living with migraine, the mean ± SD MSSS was 15.4 ± 3.2 (Figure 1). The MSSS ranges from 0 to 21 with higher scores indicating greater symptom severity across cardinal migraine features. The lowest mean ± SD MSSS was reported in Japan (13.7 ± 3.3) and the highest was reported in the USA (16.2 ± 3.1).

Migraine symptom severity scores across countries. Based on responses to the Migraine Symptom Severity Score, which ranges from 0 to 21 with higher scores indicating greater severity of symptoms.
ASC-12
Overall, 48.5% (7026/14,492) of respondents had allodynia with headache as assessed by the ASC-12 (Figure 2). Rates of allodynia were highest in the USA (58.2%; 1399/2404) and lowest in France (43.1%; 1063/2464). Across all six countries, mild, moderate and severe allodynia were reported by 22.2% (3218/14,492), 12.9% (1875/14,492) and 13.3% (1933/14,492) of respondents, respectively.

Presence of allodynia across countries. Presence of allodynia during migraine was based on the 12-item Allodynia Symptom Checklist .
Patient-reported outcomes
PHQ-4
Based on the PHQ-4, 35.5% (5146/14,492) of all respondents living with migraine reported moderate to severe symptoms of anxiety and/or depression (Figure 3), with the highest rates reported in the UK (42.9%; 1046/2436) and the lowest rates in France (28.9%; 712/2464). Overall, 37.4% (5425/14,492) of respondents reported the presence of anxiety symptoms. Proportions of respondents with the presence of anxiety symptoms ranged from 31.3% (755/2409) (Japan) to 45.2% (1100/2436) (UK). Similarly, 36.4% (5278/14,492) of all respondents with migraine reported the presence of depression symptoms. Proportions of respondents with the presence of depression symptoms ranged from 29.7% (732/2464) (France) to 42.9% (1044/2436) (UK).
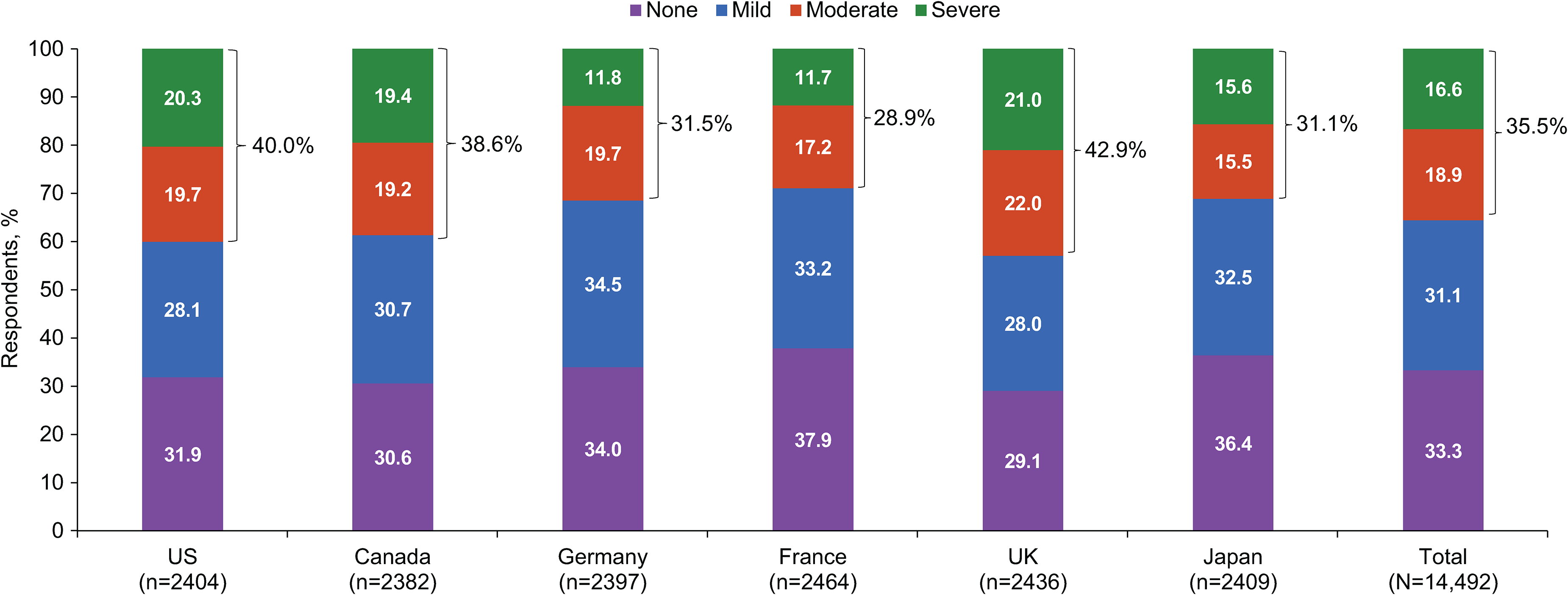
Moderate to severe anxiety and/or depression symptoms across countries. Presence of depression and anxiety symptoms over the past two weeks was based on responses to the Patient Health Questionnaire-4.
MSQ v2.1
Among all respondents living with migraine, the mean ± SD MSQ v2.1 RFR, RFP and EF domain scores were 60.7 ± 22.9, 71.5 ± 23.0 and 65.1 ± 27.2, respectively (Figure 4). Mean ± SD MSQ v2.1 RFR domain scores ranged from 57.7 ± 23.4 (Canada) to 63.3 ± 21.1 (France); mean MSQ v2.1 RFP domain scores ranged from 67.6 ± 22.9 (Germany) to 77.3 ± 22.7 (Japan); and mean MSQ v2.1 EF domain scores ranged from 63.9 ± 29.1 (USA) to 69.2 ± 24.8 (France).

Mean Migraine-Specific Quality of Life questionnaire scores across countries. Based on responses to the Migraine-Specific Quality of Life questionnaire version 2.1.
WPAI
Based on the WPAI, the mean ± SD percentage of respondents who reported currently working for pay who missed work in the previous seven days was 6.8 ± 18.1% (Figure 5). The lowest mean percentage of respondents who missed work was observed in France (4.3%), whereas the highest was observed in Germany 9.0%. The mean ± SD percentage of respondents who reported currently working for pay who reported working impaired in the previous seven days was 41.0 ± 30.1%. The lowest mean percentage of respondents who reported working impaired was observed in France (31.2%) and the highest was observed in Japan (47.8%). The mean ± SD percentage of respondents who reported currently working for pay with overall work impairment was 43.7 ± 31.9%. The lowest mean percentage of respondents with overall work impairment was observed in France (33.5%); the highest was observed in Japan (49.4%). The mean ± SD percentage of respondents who reported currently working for pay who reported activity impairment was 45.8 ± 30.1%. The lowest mean percentage of respondents who reported activity impairment was observed in France (39.3%) and the highest was observed in Japan (50.7%).

Work productivity and activity impairment scores across countries. Based on responses to the Work Productivity and Activity Impairment Questionnaire.
Discussion
This analysis of CaMEO-I data demonstrates high levels of migraine symptom severity and rates of allodynia across Canada, France, Germany, Japan, UK and USA. A substantial burden was demonstrated across all six countries surveyed. Based on the PHQ-4, moderate to severe anxiety and/or depression symptoms were reported by more than one-third of all respondents living with migraine. Mean MSQ v2.1 RFR, RFP and EF domain scores were 60.7, 71.5 and 65.1, respectively, and the percentages of work missed and work impaired were 6.8% and 41.0%, respectively. The findings were broadly similar across the six countries and build upon previously published CaMEO-I data.
The severity of headache symptoms is associated with adverse headache impact (18). The present study evaluated headache features including mean MSSS and allodynia. The mean MSSS was 15.4 and nearly half of the respondents reported the presence of allodynia in the present study. The rates of allodynia varied across countries and ranged from 43.1% in France to 58.2% in the USA. The probability of inadequate responses to various acute treatments for migraine, including non-steroidal anti-inflammatory drugs, triptans and ergots, is increased with the presence of allodynia (19). Moreover, unmet needs have been associated with higher cutaneous allodynia scores, demonstrating the importance of tolerable and effective pharmacologic treatment to manage migraine and associated symptoms, as well as the importance of effective preventive approaches (20).
In the present study, we evaluated burden through patient-reported outcomes using validated patient-reported outcome measures, including the PHQ-4, MSQ v2.1 and WPAI. Anxiety and depression are comorbid with migraine (8,21–24). In the Eurolight study, among participants with migraine, the prevalences of depression and anxiety were approximately 7% and 19%, respectively (8). Our results support these findings because over one-third of respondents reported symptoms of anxiety and depression. The presence of anxiety and depression symptoms across countries varied, with 31.3% (Japan) to 45.2% (UK) of respondents reporting the presence of anxiety symptoms and 29.7% (France) to 42.9% (UK) of respondents reporting the presence of depression symptoms. Furthermore, both migraine and depression may negatively affect HRQoL, and depression is a risk factor for migraine progression in longitudinal studies (23,25).
We found that HRQoL differed across countries. Mean MSQ v2.1 RFR domain scores ranged from 57.7 (Canada) to 63.3 (France); mean MSQ v2.1 RFP domain scores ranged from 67.6 (Germany) to 77.3 (Japan); and mean MSQ v2.1 EF domain scores ranged from 63.9 (USA) to 69.2 (France). It was previously documented that people living with migraine tend to have a lower HRQoL than those without migraine (23). Little work comparing HRQoL of people with migraine from different countries has been carried out, although there are possible hypotheses to explain differences (26). Overall, the impact of migraine on work and school activities, as well as the overall impact of migraine, has trended upward (27,28). In our findings, nearly 7% of respondents reported missing work in the previous seven days as a result of a headache, with varying results from 4.3% (France) to 9.0% (Germany). Additionally, over 40% reported working impaired in the same period, with results differing across countries and ranging from 33.5% (France) to 49.4% (Japan). Taken together, these findings demonstrate the substantial burden associated with migraine. Although our findings suggest that the impact of migraine may be lower in France than in the other countries studied, further research is needed to fully explore the effects of headache features and migraine-related disability on HRQoL in each country to ensure adequate patient care. Differences in findings among countries may be attributable to differences in healthcare delivery and to differences in rates of obesity, a factor associated with migraine severity (29), psychiatric comorbidities and allodynia, or other factors. Psychosocial factors, such as the degree of stigma by country, could also contribute to country differences. Future work will explore factors that could account for differences in illness severity indicators among countries.
The present study is limited by self-reported data and the possibility of selection bias because of the survey-based format and limited number of countries included in the study. The survey did not allow for assessment of the effect of unmeasured comorbidities on burden, although they are known to have a relationship (22,30). An additional limitation may arise from recall bias because respondents answered questions based on their headaches over the previous four weeks. Additionally, these results apply only to the high-income countries we evaluated, leaving low- and middle-income countries unexplored. The study did not have a control group of people without migraine, although some patient-reported outcomes are only pertinent to those with migraine. Another limitation is that the performance of various survey instruments in various languages and countries has not been evaluated. Therefore, some of the differences we observed could be attributed to differential performance of the survey instruments by language or country. Although the associations between headache features and disability and headache frequency and intensity were not assessed in this analysis, future analyses may be of interest to evaluate these associations on an individual country basis. Furthermore, the CaMEO-I Study utilized a cross-sectional approach and cannot assess research questions that require a longitudinal study design. Study strengths include the implementation of uniform methodology and validated migraine-related burden and HRQoL instruments. Moreover, the study included a large sample size across multiple countries and quality checks to ensure the validity of surveys.
Conclusions
For each country surveyed, migraine-specific burden, including poor quality of life and work and activity impairment, was substantial. Further research is warranted to explore potential differences between countries in the prevalence of specific headache features, disability and quality of life, and additional work is needed to raise awareness of the burden and overall impact of migraine worldwide.
Clinical implications
This analysis of CAMEO-I demonstrates the severity of headache features and the impact of migraine on HRQoL in six countries. Across all six countries, nearly half of respondents reported having allodynia. Substantial burden was demonstrated across all six countries, with over 30% of respondents experiencing anxiety and depression and over 40% reporting work impairment in the previous seven days.
Footnotes
Acknowledgments
We acknowledge the contributions of Ryan Bostic of MIST Research, Wilmington, NC, USA, for data analyses. We also thank the study participants, site collaborators and survey translators. Medical writing support was provided to the authors by Anny Wu, PharmD, of Peloton Advantage, LLC, an OPEN Health company, and was funded by AbbVie.
Author contributions
Study design: Dawn C. Buse, Richard B. Lipton, Aubrey Manack Adams and Kristina Fanning. Study investigator: Richard B. Lipton. Enrolled patients: Kristina Fanning. Collection and assembly of data: Kristina Fanning, Aubrey Manack Adams and Karen Carr. Data analysis: Richard B. Lipton and Kristina Fanning. Data interpretation: All authors. Manuscript preparation: Aubrey Manack Adams and Karen Carr. Manuscript review and revisions: All authors. Final approval of manuscript: All authors.
Data availability
AbbVie is committed to responsible data sharing regarding the clinical trials we sponsor. This includes access to anonymized, individual and trial-level data (analysis data sets), as well as other information (e.g. protocols, clinical study reports or analysis plans), as long as the trials are not part of an ongoing or planned regulatory submission. This includes requests for clinical trial data for unlicensed products and indications. These clinical trial data can be requested by any qualified researchers who engage in rigorous, independent, scientific research, and will be provided following review and approval of a research proposal, Statistical Analysis Plan (SAP), and execution of a Data Sharing Agreement (DSA). Data requests can be submitted at any time after approval in the USA and Europe and after acceptance of this manuscript for publication. The data will be accessible for 12 months, with possible extensions considered. For more information on the process or to submit a request, visit the following link: ![]() .
.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Zaza Katsarava, MD, has been a speaker and/or consultant for, and/or received research support from Allergan, Amgen/Novartis, Eli Lilly, Merck and Teva. Dawn C. Buse, PhD, has received grant support and honoraria from AbbVie, Amgen, Biohaven, Collegium, Eli Lilly, Lundbeck, Teva and Theranica and for work on the editorial board of Current Pain and Headache Reports and is the national principal investigator in the United States for the CaMEO-I Study. Elizabeth Leroux, MD, has received speaker fees and consulting fees from Allergan, Eli Lilly and Teva Neuroscience; consulting fees from Aralez Pharmaceuticals, McKesson Canada and Medscape; speaking fees, consulting fees and reimbursement for travel from Novartis; and reimbursement for travel from IHS-GPAC. Michel Lanteri-Minet, MD, reports personal fees for advisory boards, speaker panels, or investigation studies from Allergan, Amgen, Astellas, ATI, BMS, Boehringer, Boston Scientific, CoLucid, Convergence, GlaxoSmithKline, Grunenthal, IPSEN, Lilly, Lundbeck, Medtronic, Menarini, MSD, Novartis, Orion Pharma, Pfizer, Reckitt Benckiser, Saint-Jude, Salvia BioElectronics, Sanofi-Aventis, Teva, UCB, UPSA and Zambon. Fumihiko Sakai, MD, is a consultant, speaker or scientific advisor for Amgen, Eisai, Eli Lilly, Otsuka and Teva, and the national principal investigator in Japan for the CaMEO-I Study. Manjit Matharu, MD, serves on the advisory board for Abbott, AbbVie, Eli Lilly, Lundbeck, Medtronic, Pfizer, Salvia and Teva; has received payment for the development of educational presentations from AbbVie, electroCore, Eli Lilly, Novartis and Teva; and is the national principal investigator in the United Kingdom for the CaMEO-I Study. Aubrey Manack Adams, PhD, and Karen Carr, PhD, are employees of AbbVie and may hold AbbVie stock. Kristina M. Fanning, PhD, is managing director of MIST Research, which has received research funding from AbbVie, Allay Lamp, NYC Langone Health, Juva Health and GlaxoSmithKline via grants to the National Headache Foundation. Richard B. Lipton, MD, receives research support from the Marx Foundation, the National Headache Foundation, the National Institutes of Health and the US Food and Drug Administration. He serves as a consultant or advisory board member for or has received honoraria or research support from AbbVie/Allergan, Amgen, Biohaven, Dr Reddy's Laboratories (Promius), electroCore, Eli Lilly, GlaxoSmithKline, Lundbeck, Merck, Novartis, Teva, Vector and Vedanta Research; receives royalties from Informa and Wolff's Headache, 8th edition (Oxford University Press, 2009); holds stock/options in Axon, Biohaven, CoolTech and Manistee; and is the overall principal investigator for the CaMEO-I Study.
Ethical statement
Before participant recruitment, a central institutional review board or ethics committee reviewed and approved the study design. Eligible participants provided informed consent.
Funding
The following financial support was received for the research, authorship and/or publication of this article: AbbVie funded this trial and contributed to the study design, the collection, analysis and interpretation of data, as well as the review and approval of the final manuscript for publication. All authors had access to relevant data and participated in the drafting, review and approval of this publication. No honoraria or payments were made for authorship.