
Abstract
Introduction
Subcutaneous sumatriptan, a 5HT1B/1D agonist, is the most effective drug in cluster headache acute treatment. About 25% of the patients do not respond to subcutaneous sumatriptan; the reasons for this are unknown. In this study, we compare clinical characteristics of cluster headache patients responding and non-responding to subcutaneous sumatriptan.
Methods
We retrospectively investigated the clinical records of 277 cluster headache patients. Patients reporting repeated satisfactory response to subcutaneous sumatriptan within 15 minutes were considered responders.
Results
Of 206 cluster headache patients who had used subcutaneous sumatriptan (mean age 45.6, 16% females, 48% chronic), 91% were responders, and 9% non-responders. Compared to responders, non-responders had longer and more frequent attacks: 60 (median; IQR 38–90) vs. 100 (60–120) minutes (p = 0.028), 4 (2.5–5) vs. 3 (2–4) attacks/day (p = 0.024). No other difference was found.
Conclusions
In cluster headache attacks with long duration and high frequency, pain mechanisms not involving 5HT1B/1D receptors may play a more relevant role.
Introduction
Cluster headache (CH) is the most frequent trigeminal autonomic cephalalgia (TAC), among the worst painful conditions, characterised by attacks of excruciating head pain lasting 15–180 minutes (1). Subcutaneous sumatriptan (SS), a 5HT1B/1D receptor agonist, is the most effective and probably widely used treatment to abort CH attacks (2). Its efficacy is remarkable for both rapidity and consistency: It terminates CH attacks within 15 minutes from injection in the vast majority of patients (2). However, in clinical trials, about 25% of CH patients do not respond to SS (2). The reasons for this unresponsiveness remain unknown. Given the highly specific action of SS on 5HT1B/1D receptors, identifying clinical phenotypes associated with poor drug responsiveness could help to better understand the pathophysiology of craniofacial pain in CH. In this study, we examined the clinical characteristics of CH patients comparing responders (R) and non-responders (NR) to SS.
Methods
We retrospectively investigated the clinical records of 307 patients diagnosed as TACs, consecutively visited from 1 January 2015 to 31 May 2019 at the Headache Centre of the Besta Neurological Institute, Milan, Italy. This is a tertiary national referral centre for CH and related disorders. Diagnosis of chronic CH (CCH) and episodic CH (ECH) was according to the International Classification of Headache Disorders, 3rd edition (1). The following variables were obtained from the clinical records: Age at last observation, sex, age at onset, disease duration, episodic or chronic CH form, site of pain and in particular whether it was restricted to trigeminal territories or not, average duration of untreated attacks, average attack frequency, presence of autonomic phenomena, presence of restlessness or agitation, headache side, and side shift. The data used for the analysis was extracted from the last available visit. This could be either the first visit to our centre or, more frequently, a follow-up visit. Apart from historical data (e.g. age at onset of the disease, history of side shift), that could be derived from previous records, clinical data refer to the most recent period before the last visit. The duration of attacks always refers to the spontaneous duration, meaning without any acute treatment (sumatriptan or oxygen or any other). The frequency of attacks refers to spontaneous frequency without any treatment in ECH; for CCH the frequency of attacks refers to periods when the patient was unresponsive to prophylaxis. Patients reporting repeated satisfactory responses (complete or near complete resolution) to SS within 15 minutes were considered responders (R). Using SPSS software, version 21.0, we compared non-responders (NR) with R. Continuous variables are presented as mean ± SD or median (interquartile range, IQR) and were compared using the Student’s t-test or Mann-Whitney U-test according to the normal distribution of the variable. For categorical variables, we used the Chi-square test or Fisher’s exact test according to the number of categories. Missing data were excluded from the analyses in a pairwise fashion. Two-tailed tests were used with a significance level of p < 0.05. The study was approved by the Institutional ethical standards committee. Data availability: anonymised data will be shared by request from any qualified investigator.
Results
A definite diagnosis of CH was found in 277 out of the 307 TAC patients (30 had other forms of TAC); 63 CH patients (22.4%) had never tried SS; in eight patients, the response to SS wasn’t clearly reported. These 71 patients were excluded from subsequent analyses (Figure 1). Clinical characteristics of the 206 CH patients who had tried SS were: Mean age at observation, 45.6 ± 10.5 years; 33 females (16%); 98 chronic CH (CCH, 47.6%); median disease duration 13 years (IQR 7–22). There were 187 (90.8%) R and 19 (9.2%) NR. NR had longer attack duration and higher attack frequency compared to R: Median 100 (60–120) versus 60 (38–90) minutes (p = 0.028), and 4 (2.5–5) versus 3 (2–4) attacks per day (p = 0.024) (Figure 2). No other differences were found (Table 1). CCH patients have been reported to have longer attack duration and higher headache frequency compared to ECH (3). As this resembles what we observed in NR to SS, we conducted a post-hoc analysis comparing these variables between CCH and ECH patients in our population. CCH patients had a higher headache frequency (3.6 vs. 2.8 mean attacks/day respectively; mean difference 0.8, 95% CI 0.4–1.3; p < 0.001 at uncorrected t-test). The attack duration was similar (CCH 73.1 minutes; ECH, 77.7; p 0.6 at t-test).
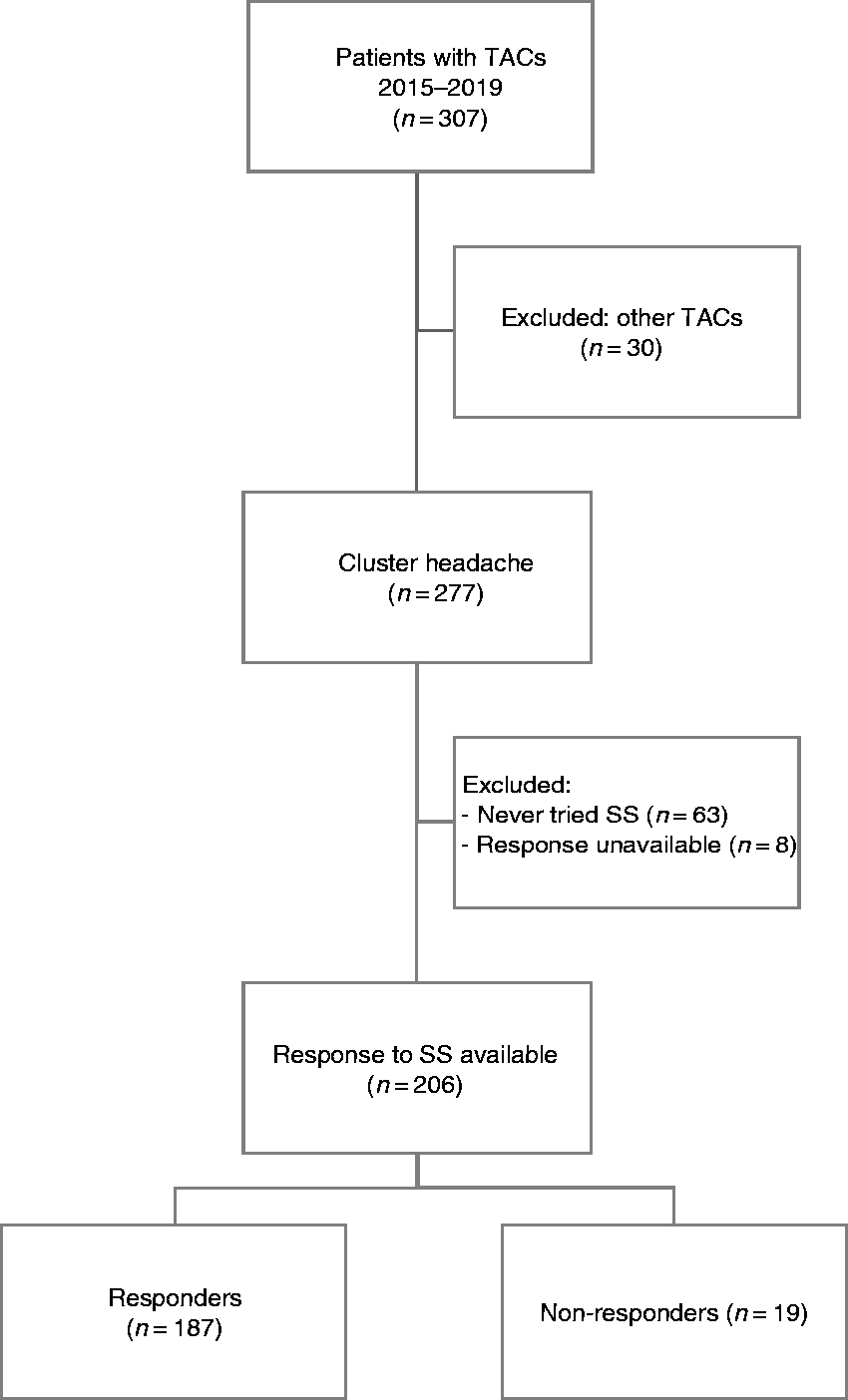
Flow chart of the selection of patients.
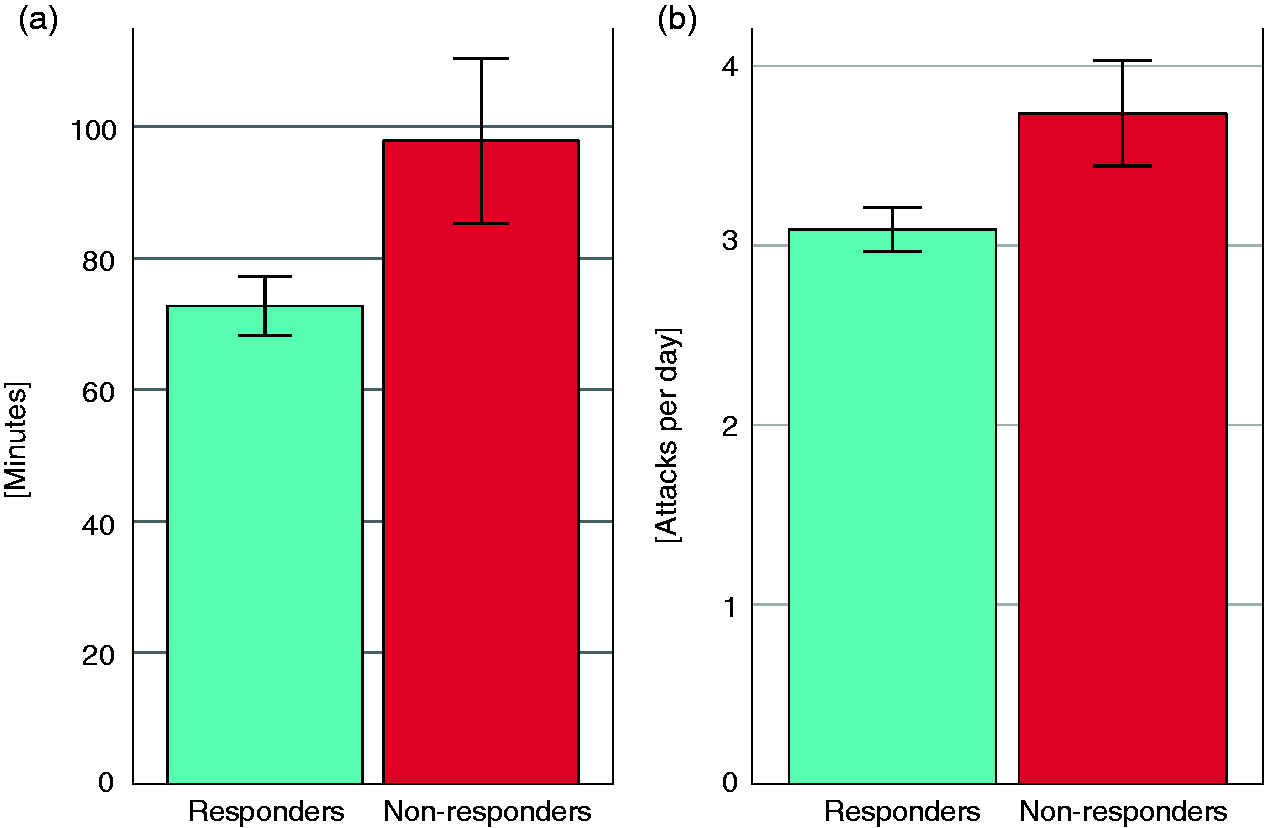
Mean duration (a) and frequency (b) of cluster headache attacks in responders and non-responders to subcutaneous sumatriptan. Error bars indicate standard errors of the mean.
Clinical characteristics of responders and non-responders to subcutaneous sumatriptan.

Comparison of clinical characteristics between responders (R) and non-responders (NR) to subcutaneous sumatriptan (SS). NR had longer attack duration and higher frequency of attacks. No other difference was found.CH: cluster headache; IQR: interquartile range; N: number of subjects; SD: standard deviation.Bold values denote significant results at p < 0.05.aFisher’s exact test; bChi-square test; cStudent’s t-test; dMann-Whitney U-test.
Discussion
This study confirms that in a minor proportion of CH patients, sumatriptan injection does not improve the ongoing acute pain. Patients not improving after SS had longer duration of untreated attacks and higher attack frequency compared to R.
These results could have been biased by the fact that: a) This is a retrospective study; b) the low number of NR might have reduced the power of analysis; c) the population is from a tertiary headache centre with a higher proportion of CCH patients compared to the general population (almost half of the present sample were CCH, compared to 10–15% among the general population) (1).
Notwithstanding these limitations, given the established efficacy and the specificity of action of sumatriptan in CH, our findings could contribute to better understanding the pathophysiology of pain in CH.
Great importance is attributed to CGRP in CH pathophysiology (4) and a number of observations link the mechanism of action of sumatriptan to the CGRP pathway in CH: Sumatriptan inhibits the release of CGRP from trigeminal nerve endings in experimental animal models (5); in humans, SS simultaneously reduces CH pain and CGRP plasma levels in the external jugular vein ipsilateral to the pain, while opioids reduce pain without affecting CGRP levels (6). Recent studies suggest a different role of CGRP in episodic and chronic CH: Patients with CCH are less susceptible to developing CH attacks after CGRP infusion than ECH during active cluster periods (7), and the anti-CGRP monoclonal antibody galcanezumab is not effective in CCH (8) but improves ECH (4). Taken together, these observations may indicate that CGRP-related mechanisms are less important in CCH than in ECH. Accordingly, if the mechanism of action of SS was linked to CGRP, NR to SS should be more represented in CCH than in ECH, but this was not the case (Table 1). We found that CCH had higher headache frequency (3) compared to ECH, but attack duration did not differ between the two groups. At least in part, this observation could confirm the hypothesis that CGRP-related mechanisms are less relevant in CCH than in ECH. This could explain why SS is less effective when CH pain has a higher frequency. Unfortunately, the small number of NR does not allow further analysis to confirm this hypothesis. More studies are needed to better understand if the diagnosis – ECH versus CCH – affects the responsiveness to SS or if it is just due to attack frequency and duration irrespective of the diagnosis. In addition to the possible link between sumatriptan and the CGRP pathway at peripheral level, other mechanisms of action of sumatriptan in CH can be hypothesised to occur within the central nervous system. In an animal model of TAC, sumatriptan reduced the activity in the trigeminocervical complex (TCC) after parasympathetic activation more than the CGRP-receptor antagonist olcegepant (9).
A recent animal study showed that the highest sumatriptan concentration in the CNS was reached in the hypothalamus after 1 and 5 min of a subcutaneous injection of the drug (10). It is noteworthy that the hypothalamic concentration of the drug was higher compared to the trigeminal ganglion and the meninges (10), both peripheral sites where sumatriptan is commonly thought to exert its action in CH. The administration of 6 mg subcutaneous sumatriptan in humans was associated with a decrease in 5-HT1B receptor binding in the brain, particularly in pain-modulating regions (11). Sumatriptan regularly terminated CH attacks in a patient whose trigeminal nerve was completely lesioned (12). Also, when given orally, 100 mg sumatriptan reaches sufficient CSF concentrations to exert pharmacological actions in humans (13).
The results of our study suggest that additional non-5HT1B/1D extra-hypothalamic mechanisms could intervene when CH attacks are long lasting and more frequent. In other words, hypothalamic 5HT1B/1D-related pain mechanisms may play a pre-eminent role in terminating the pain in the initial phases of CH attacks. Further studies are needed to confirm our findings.
Investigating the correlation between the response to highly specific treatments such as sumatriptan and clinical phenotypes offers an important tool to unravel the mechanisms of the disease, and possibly has the potential to develop patient-tailored treatment.
Clinical implications
Patients with cluster headache who are resistant to sumatriptan have longer and more frequent attacks. Specific pain mechanisms may be considered in different patients with cluster headache.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Italian Ministry of Health [research program RF-2016-02364909].