
Abstract
Objective
To describe the headache characteristics and functional disability of a large sample of treatment-seeking youth with continuous headache and compare these factors across diagnostic subgroups of chronic migraine and new daily persistent headache.
Methods
This retrospective study utilized clinical information (e.g. diagnosis, headache features, medication overuse, functional disability) from a large data repository of patients initially presenting to a multidisciplinary headache center with continuous headache. Patient inclusion in subgroup analyses for chronic migraine and new daily persistent headache was based on clinician diagnosis using International Classification of Headache Disorders (ICHD) criteria.
Results
The current sample included 1170 youth (mean age = 13.95 years, 78.8% female) with continuous headache. The overwhelming majority of these youth had headaches with migrainous features, regardless of their clinical diagnosis. Youth with chronic migraine reported a longer history of continuous headache symptoms and earlier age of headache onset than youth with new daily persistent headache and were more likely to have medication overuse. Most youth with continuous headache experienced severe migraine-related functional disability, regardless of diagnostic subgroup.
Conclusions
Overall, youth with continuous chronic migraine and new daily persistent headache did not have clinically meaningful differences in headache features and associated disability. Findings suggest that chronic migraine and new daily persistent headache may be variants of the same underlying disease.
Introduction
Continuous – or always present – headache is rare and generally considered to be more treatment resistant than primary headache disorders with intermittent headaches. As a result, clinical research on continuous headache is limited, particularly among child and adolescent populations. For many years, our understanding of continuous headache has long been limited to findings from a broad characterization of chronic daily headache (≥15 headache days/month) (1), where the headache characteristics of a small sub-sample of youth with continuous headache were described and compared to youth with daily intermittent headache and chronic daily headache more broadly. That study suggested that youth with continuous headache may have a unique clinical presentation relative to other pediatric headache patients, but was limited in its ability to examine patients’ clinical characteristics in the context of current nosology. Given the significant refinement of diagnostic classification of primary headache disorders in recent years, additional research is needed to characterize the headache phenotypes of a large sample of youth with continuous headache across primary diagnostic sub-groups.
According to the International Classification of Headache Disorders 3rd edition (ICHD-3) (2), youth with continuous headache who have a primary headache disorder may be classified as having one of the following diagnoses: Chronic migraine (CM), new daily persistent headache (NDPH), chronic tension-type headache (CTTH), and hemicrania continua. Recent research has begun to focus on characterizing youth with NDPH – a type of continuous headache characterized by an abrupt onset (i.e. within 24 hours) that persists for at least 3 months (3). However, there is a lack of research comparing these youth to those presenting with continuous CM, which is much more common among treatment-seeking pediatric patients and tends to progress or chronify over time (4–6). Although NDPH is considered a distinct clinical phenomenon from CM, the overwhelming majority of individuals with NDPH have a migrainous phenotype to their headache, and it has been suggested that NDPH with migrainous features may be a form of prolonged status migrainosus (3,7). Comparisons of continuous headache characteristics in youth with NDPH and CM will therefore provide novel information about the extent to which NDPH is truly distinct from continuous CM, or whether these diagnostic groups simply reflect a different pattern of onset of the same disorder.
The current study extends previous research by evaluating the headache characteristics and functioning of a large cohort of child and adolescent patients presenting to a multidisciplinary headache center with at least 1 month of continuous headache. To address current gaps in the literature, the current study also performed subgroup analyses to identify clinical differences between patients with continuous CM and those with NDPH.
Methods
Study design and patient population
This retrospective, observational study utilized data from a large repository that included clinical information from all pediatric (<18 years of age) patients seen for an initial appointment at the Cincinnati Children’s Hospital Headache Center between August 1997 and March 2019. Headache Center repository data was extracted from all patients who reported having an “always” present headache at the time of their initial appointment (n = 1592). The current study was approved by the Institutional Review Board at Cincinnati Children’s Hospital Medical Center; patients’ families provided informed written consent to have patient information stored in the Headache Center data repository.
Continuous headache screening criteria
To be included in the current study, patients had to have reported experiencing continuous headache symptoms for at least 30 days prior to their initial Headache Center appointment (i.e. endorsing experiencing headache every day over the past month on an intake questionnaire). This initial screening criterion was established in an attempt to rule out patients presenting to clinic with status migrainosus, while casting a relatively wide net for clinical diagnoses so as to capture as heterogeneous a sample of continuous headache patients as possible. Patients also needed to have reported an average headache duration of 24 hours per day; this screening criterion was established to rule out individuals who reported experiencing an intermittent headache every day. If discrepancies existed in patient headache duration and frequency information (e.g. a patient’s data repository records indicated that participants had a headache 30 days per month, but average duration was less than 24 hours/day), co-authors BLR and EJR attempted to review source records to resolve discrepancies. Patient data was included in the current study if data discrepancies could be resolved by clinician or patient comments on source documents.
Inclusion criteria for diagnostic subgroups
All patients included in the current study received a clinical diagnosis from a headache medicine neurologist using current ICHD criteria (2). Patients were included in our diagnostic subgroups if they had been given a diagnosis of CM or NDPH; ICHD-3 criteria for these conditions were retrospectively applied to the extent possible during our data extraction (see the Statistical Approach section for more information regarding our diagnostic subgroup classification).
Data collection procedure and measures
Primary data extracted from the Headache Center repository included information provided by patients in a detailed questionnaire completed during their initial Headache Center appointments. This questionnaire was reviewed by a headache medicine neurologist during a thorough interview with the patient and patient’s family, and the reported data was amended and finalized to reflect the consensus of the interview process. As part of this appointment, Headache Center providers also completed physical, neurological, and headache-specific examinations of patients and established a clinical diagnosis for patients in accordance with ICHD criteria.
Throughout the entirety of the data collection period for the current study, it should be noted that the record keeping strategy and management of the clinic was consistent. Over time, specific questions were added to the initial appointment questionnaire that facilitated the headache medicine neurologist’s history taking with patients; however, the general approach to establishing clinical diagnoses for patients has been consistent across physicians and over time. Specific data extracted from this Headache Center visit is described below.
Demographic information was collected regarding patient sex, race, and age at the time of their initial Headache Center visit. Information was extracted regarding patients’ headache characteristics, and included patients’ clinical diagnoses, as well as patient endorsement of migraine features associated with their headaches (e.g. vomiting or nausea, photophobia or phonophobia), patient-reported history of continuous headache experience (in months), patient age of headache onset (continuous or intermittent), and patient average self-reported headache severity, as rated on a scale of 0 (no pain) to 10 (worst possible pain).
Factors associated with headache presentation: Information was also collected regarding patients’ probable medication overuse, as reported by Headache Center providers. Given that retrospective analyses have demonstrated that youth with NDPH, and to a lesser extent CM, are most likely to have onset of symptoms during months in which children start or return to school (8), information was also calculated regarding month of headache onset by subtracting the number of months the patient reported experiencing a continuous headache from the date (month, year) of that patient’s initial Headache Center appointment.
Headache-related functional disability was assessed using the PedMIDAS, a 6-item, interview-based measure of migraine-related disability at school and at home (9). Higher scores on this scale indicate higher levels of headache-related disability, such that scores between 0–10 = little or no disability, 11–30 = mild disability, 31–50 = moderate disability, and 51+ = severe disability.
Statistical approach
Primary analyses were conducted in SPSS version 25.0 (IBM Corp) and Mplus Version 8.3 (10). Descriptive statistics were conducted to summarize the demographic and diagnostic make-up of our sample. In the current study, youth with continuous headache that had a migraine diagnosis (i.e. migraine with and without aura, chronic migraine) were categorized as having CM. The exceptions to this were individuals diagnosed with NDPH and a migraine diagnosis; in these cases, the NDPH diagnosis superseded the migraine diagnosis (i.e. they were only coded as having NDPH) in accordance with ICHD-3 criteria.
Relative frequencies of migraine symptoms, medication overuse, migraine-related functional disability, and month of continuous headache onset were calculated for primary diagnostic subgroups, as well as for our combined continuous headache sample. Multivariate 2-group (CM vs. NDPH) analyses were conducted to assess differences in continuous demographic and headache characteristic variables among our two diagnostic subgroups of interest. Potential type-1 error inflation of post hoc pairwise comparisons was controlled for using false discovery rate procedures (11). Multivariate logistic regression was conducted to determine the extent to which binary headache characteristic variables predicted diagnostic subgroup membership, and chi-square analyses were also conducted to determine potential differences in the distribution of migraine-related functional disability and month of continuous headache onset seen across diagnostic subgroups.
Pairwise missing data for the multivariate 2-group comparison ranged from 0.6–35%. With the exception of clinical information assessing history of continuous headache (in months), which was not obtained from patients presenting to clinic prior to March 2009, variables assessing patient demographic and headache characteristics had less than 5% missing data. Missing data was 3.3% for our logistic regression. Maximum likelihood estimation was used to account for missing data in both of these subgroup analyses.
Results
The final pediatric sample included 1170 youth (ages 3–17) with continuous headache. The sample was 78.8% female and 89.1% White, 7.2% Black/African American and 3.6% other. Mean age at initial Headache Center appointment was approximately 14 years old. On average, patients had experienced a continuous headache for almost 1 year. The vast majority of this sample (96.1%) had received a migraine diagnosis at their initial Headache Center appointment, and 84.3% were diagnosed with CM. Over 150 youth were diagnosed with NDPH (n = 155, 13.2%), and the remaining 29 youth (2.5%) were diagnosed with another primary ICHD diagnosis (e.g. CTTH [n = 13], post-traumatic headache [n = 3], probable migraine [n = 7]). Due to the relatively small sample sizes of these three diagnostic subgroups, they were not included in any subgroup-level analyses.
Tables 1 and 2 summarize results from our multivariate 2-group comparison and multiple logistic regression analyses and provide the relative frequencies of various migraine features and associated headache characteristics for the entire pediatric continuous headache sample, as well as for CM and NDPH subgroups. Some statistically significant differences were found in the clinical presentation of youth with NDPH and CM. When compared to youth with CM, youth with NDPH experienced their first headache at a slightly later age on average, and experienced continuous headache for fewer months prior to their initial Headache Center appointment (see Table 1). As shown in Table 2, youth with CM were more likely than youth with NDPH to report photophobia with their headaches, although the majority of youth with NDPH also endorsed this migraine feature. Youth with CM were also more likely to be diagnosed with medication overuse (∼1/3 of patients) than were youth with NDPH (∼1/5 of patients; see Table 2). Of note, we tested our subgroup models regarding headache characteristics and associated features in the context of youth age and sex. Diagnostic subgroup differences were not moderated by these factors.
Results from multivariate 2-group comparison analyses, with summary of relevant pediatric continuous headache characteristics in full sample and primary diagnostic subgroups.

*Bolded values denote significant subgroup differences after accounting for type-1 error inflation.
CI: confidence Interval; ESd: effect size: Cohen’s d.
Results from multiple logistic regression subgroup analyses, with summary of relevant pediatric continuous headache characteristics in full sample and primary diagnostic subgroups.

*Bolded values denote significant subgroup differences after accounting for type-1 error inflation.
b: Unstandardized regression coefficient; CI: confidence interval; ESOR: effect size: Odds ratio.
As highlighted in Figure 1, the majority of youth with continuous headache (57.9%) reported severe migraine-related functional disability. No subgroup differences in patterns of functional disability were identified (χ2 (3, 1103) = 3.73, p = .29). Similarly, no subgroup differences emerged when month of continuous headache onset trends were compared between youth with CM and those with NDPH (χ2 (11, 767) = 2.56, p = .995). Frequencies of continuous headache onset are illustrated in Figure 2, and highlight an increased incidence of continuous headache onset around the start of the academic year (August, September, and October).
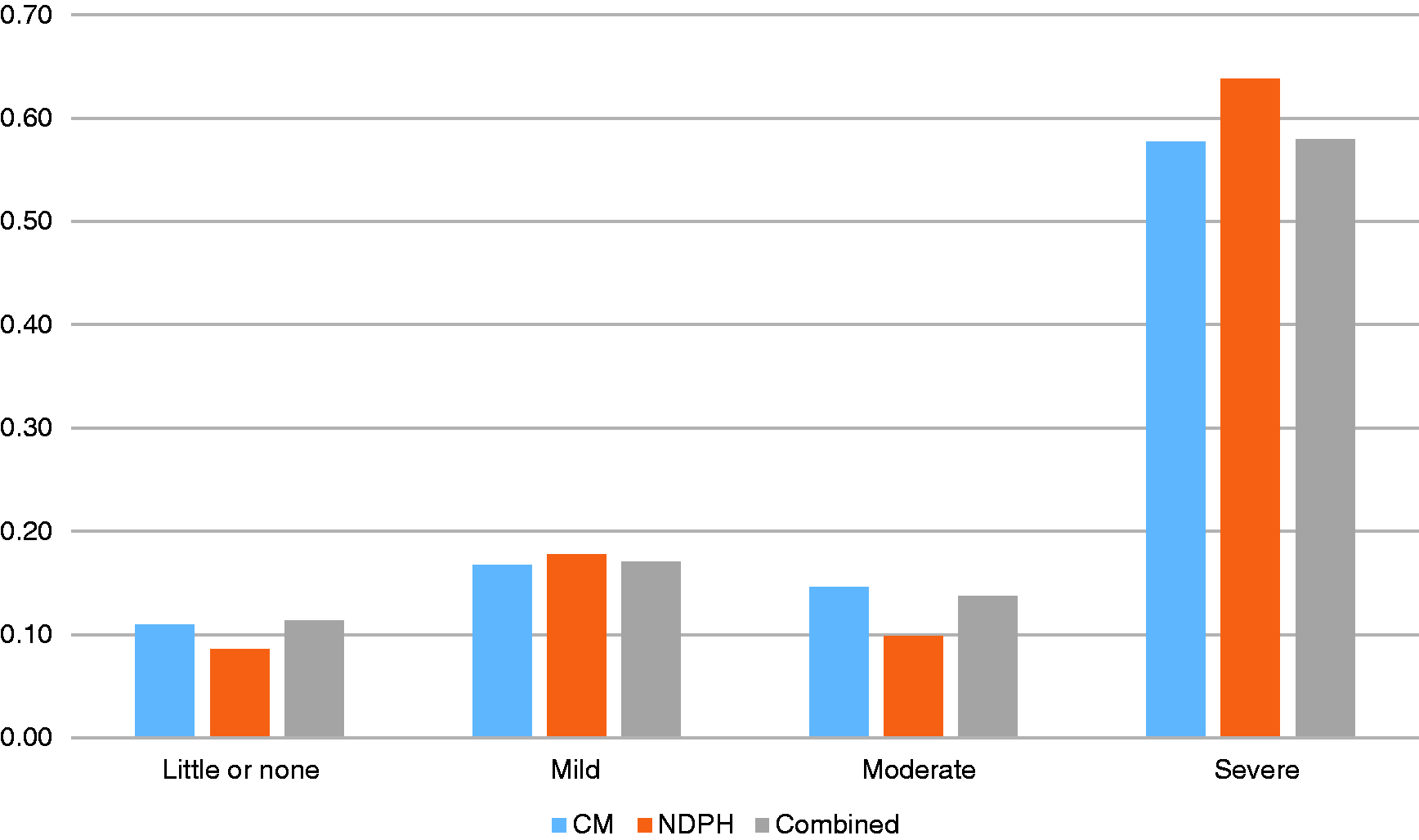
Continuous headache-related functional disability, as indicated by PedMIDAS severity rating percentages.

Frequencies of estimated continuous headache onset by calendar month in the child and adolescent sample.
Discussion
In the largest study of pediatric patients with continuous headache to date, we found that the vast majority of youth with continuous headache met ICHD criteria for CM. This is consistent with prior studies showing that pediatric patients with chronic daily headache have a migrainous phenotype. In the subset of patients meeting criteria for NDPH, the majority would have also met criteria for CM, but for the characteristic sudden onset described in NDPH. In line with this finding, frequencies of migraine features and patterns of migraine-related disability were generally the same amongst CM and NDPH subgroups, which support the idea that – at least among children and adolescents – these diagnostic categories may not reflect meaningfully different disease processes, but rather differences in the manifestation of continuous chronic migraine over time. This hypothesis is supported by the fact that patients with NDPH tended to seek treatment more quickly after onset of their continuous headache in the current study, perhaps reflecting the increased concern families may have over a sudden onset unrelenting headache as opposed to one that develops gradually from intermittent headaches over the course of months or years. The increased rates of medication overuse in CM in the current study may also reflect the role of excessive medication increasing the risk of more gradual headache chronification in some youth with migraine (6,12).
That said, to formally test whether continuous CM and NDPH are variants of the same underlying disease process, prospective longitudinal studies are needed to classify and capture the temporal progression of continuous headache symptoms, particularly in the context of current ICHD-3 criteria for CM and NDPH. Although we retrospectively applied ICHD-3 criteria to the extent that this was possible, we were unable to retrospectively assess specific aspects of patient’s initial headache presentation (e.g. number of migraine days in a given month) that were used to make clinical diagnoses. Future prospective studies that capture this diagnostic information, and then track patient’s headache and migraine-related symptoms over time, will be able to provide novel information about clinical/diagnostic features that serve as prognostic indicators in this patient population.
Studies have demonstrated that several other factors may predispose individuals to continuous headache. For example, infections, physical stress and joint hypermobility have all been implicated as potential risk factors for NDPH (13). Genetic factors, comorbid pain symptoms, low socioeconomic status, female sex, stressful life events, obesity and sleep problems have also been implicated as potential risk factors for headache chronification (6,13). Our study supports other findings that suggest that the start of the school year – a time of increased psychosocial stress – is a period of vulnerability for continuous headache onset. Additional research is needed to determine the role of these potential etiological factors on the rate of continuous headache onset in pediatric populations. Studies that explore the role of development in the rate of continuous headache onset are also needed, as patients with NDPH tended to have slightly older age of onset of headache than those with CM in the current study.
Given that this was a single center study focused on treatment-seeking youth, additional study of youth with continuous headache is needed to replicate the current findings, particularly among samples of youth from other geographic regions and diverse racial, ethnic, and cultural backgrounds. As highlighted above, future research should also examine the course of headache symptoms and treatment response for youth with continuous headache over time. A present study is evaluating additional psychosocial characteristics and initial treatment response in this cohort of continuous headache patients. However, given the limitations of this study’s retrospective design, future prospective, longitudinal studies are needed to more comprehensively examine patterns of treatment utilization – as well as factors that influence pain and functional treatment outcomes – in youth with continuous headache. Such work is in the planning stages and will be critical in informing the development and systematic evaluation of treatments for this understudied population.
Clinical implications
The vast majority of treatment-seeking youth with continuous headache have migraine features. This group is also characterized by notable migraine-related functional impairment. Few clinically meaningful differences exist between youth with continuous chronic migraine and those with new daily persistent headache. Clinical research should focus on factors associated with treatment response in youth with continuous headache.
Footnotes
Acknowledgements
This project would not be possible without the clinical coordination and research efforts of the faculty and staff embedded in the Cincinnati Children’s Headache Center.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ADH reports receiving consulting fees from the following industry sources: Alder, Amgen, Avanir, Biohaven, Curelator, Electrocore, Eli Lilly, Impax, Supernus, Teva, Theranica, and Upsher-smith. Additionally, ADH, MAK, and JK have received research funding for participation in ongoing studies sponsored by Amgen, Teva, Impax, and Curelator. All consulting and research funds for this work are paid directly to Cincinnati Children’s Hospital Medical Center. This work does not impact the current findings. The authors declare that there is no other potential conflict of interest for this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an NIH-funded T32 training grant (T32DK063929) in Child Behavior and Nutrition at Cincinnati Children’s Hospital Medical Center.