
Abstract
The objective was to develop and validate a patient-based grading scale for PedMIDAS. PedMIDAS was administered to 329 children, who rated their overall disability based on the adult MIDAS grades. This patient-based rating and PedMIDAS scores were compared to develop the grading scale. Headache disability was rated little to none, 49.5%; mild, 26.7%; moderate, 15.8%; and severe, 7.9%, with PedMIDAS raw scores of 4.9 ± 6.3, 17.8 ± 14.9, 40.6 ± 34.2, and 91.4 ± 69.8. Convergence of these results yielded an empirically derived grading system: Grade I, 0-10; II, 11-30; III, 31-50 and IV, > 50. Higher grades corresponded to an increased need for prophylactic treatment. A patient-based grading scale further increases the utility of PedMIDAS in assessing migraine disability in children, so that it can be widely used in routine clinical evaluation and management.
Introduction
Headaches, more specifically migraines, are a frequent problem for children and adolescents. Up to 10% of children between the ages of 5 and 15 have migraines (1), while an even higher number of adolescents have migraines (2).
A key component of migraine evaluation and treatment is assessment of migraine disability. The adult (age 20–50 years old) MIgraine Disability ASsessment (MIDAS) tool was developed for this purpose (3). It does not take into account the developmental differences of children and children's lifestyles. A Pediatric MIgraine Disability ASsessment tool (PedMIDAS) was developed to assess disability due to migraines in children and adolescents (4). A raw score is obtained by adding the six individual questions. The raw score can be used to assess initial disability as well as monitor improvement with treatment over time.
A simplified grading system has been developed for the adult MIDAS that converts the raw score into one of four grades of disability: Grade I, little to no disability; Grade II, mild disability; Grade III, moderate disability; and Grade IV, severe disability. The grading system for MIDAS was developed by expert opinion with subsequent physician validation in a small number of patients (5). A clinical application proposed for MIDAS was to guide decisions about the intensity of treatment – the stratified care model (6). In this model, different levels of therapy are used based on the adult MIDAS grade level. In the adults studied, the use of the grading system for MIDAS resulted in improved outcome compared with step-care (6, 7). A clinically useful grading system for PedMIDAS has not yet been developed.
For children, the interpretation of pain and pain-related symptoms is often inadequately assessed by adults (8). Adults are often unable to incorporate a child's developmental level in their pain ratings. Adolescents often perceive this as a lack of belief by the adults in their lives that they are truly having headache pain, therefore resulting in a misinterpretation by the adults of the adolescent's disability. We addressed these issues through the development of a grading system for PedMIDAS based on the patient's perception of their disability in correlation with a validated disability tool for children, PedMIDAS, thus eliminating the potential of the adult or physician biasing the patient's disability. This system can be used by the practitioner to guide treatment and monitor response.
Methods
Patient population
Children with migraine headaches were evaluated in either the Cincinnati Children's Headache Center or its satellite out-patient facility. As part of the standard assessment, a detailed questionnaire at initial and follow-up evaluations is obtained. This questionnaire includes information about headache frequency, severity, duration, and characteristics, as well as some general health screening, documentation of school absences, and ratings of functioning at home and school. Frequency was measured in headache days per month, severity was measured on a 0–10-point scale, duration was measured in hours, school absences were measured in days per semester (half of academic year), and percent function was patient's self-report of functioning. Diagnosis was determined using International Headache Society criteria as well as a clinical impression of the headache diagnosis. PedMIDAS was administered to all of the patients as part of this questionnaire at initial and follow-up evaluations (4). The questionnaires were reviewed, a detailed history obtained, and a general physical and neurological examination conducted at each evaluation.
PedMIDAS questionnaire
Details of the PedMIDAS questionnaire and its validation have been described previously (4). PedMIDAS has been validated with internal consistency and test–retest reliability in 441 patients. In brief, PedMIDAS is based on the adult MIDAS with developmentally appropriate changes and adjustments for childhood lifestyle. PedMIDAS is a six-item questionnaire. The initial three questions deal with impact of headache on school; question 1 asks about school day absences; question 2 asks about partial day absences; and question 3 asks about functioning at 50% or less ability in school. The fourth question assesses the impact due to headache at home and includes inability to perform homework and chores. The final two questions assess disability in social functioning including sports; question 5 asks about complete absence from activities, while question 6 asks about functioning at 50% or less of their ability.
PedMIDAS grading system
Three hundred and twenty-nine consecutive patients completing PedMIDAS were asked after completion to rate their overall disability due to headache in the preceding 3 months (global rating). The patients were prompted with the choices of none to little, mild, moderate, and severe – the terms used by the adult MIDAS grading system. Responses to this question were obtained prior to discussing PedMIDAS scores and their significance with the patients. Mean PedMIDAS scores with standard deviations were determined for each of the four global rating responses. The convergence of the global rating and PedMIDAS raw score values was used to develop a non-overlapping grading system that mirrors the grading system terms of the adult MIDAS.
Treatment analysis
Longitudinal improvement in PedMIDAS scores and disability grades over the course of treatment was measured. PedMIDAS was administered to all patients at all visits, new and follow-up, attending the Cincinnati Children's Headache Center (n = 1290). The abortive and prophylactic treatments used in this population that had completed PedMIDAS were analysed in comparison with the new PedMIDAS grading scale.
Statistical analysis
Statistical analyses were performed with means and standard deviations applied to z and P scores using a normalized distribution. A statistical standard of P < 0.001 was used throughout the study to minimize the influence of potential interdependent variables.
Results
Patient characteristics
Three hundred and twenty-nine patients completed PedMIDAS and reported a global rating of disability due to headaches. One hundred and twenty-two patients were evaluated at their initial visit, while 207 were seen at follow-up appointments. The mean age for the total group was 12.4 ± 3.9 years (range 5–20), while the mean age was 11.9 ± 3.3 years (range 6–18) for the initial group and 12.8 ± 3.4 years (range 5–20) for the follow-up group. The demographics of these patients were similar to the population seen in the Headache Center (Table 1). Patients received multidisciplinary, standardized treatment (9–11). At presentation, the follow-up group had similar headache characteristics to the initial group and showed improvement of all features with treatment. Of the 207 patients seen in follow-up, 64 were seen at their first follow-up evaluation, 35 at their second, 30 at their third, 24 at their fourth and 54 at later follow-up evaluations. Table 2 presents information regarding headache diagnosis and characteristics for the initial and follow-up groups. Table 3 presents information regarding school absences and reported functional ability at home and school during a headache attack.
Patient demographics

∗P < 0.001 compared with total population.
Headache characterization

IHS, Internationa Headache Society.
∗P < 0.001 compared with total population (reflects response to treatment).
†P < 0.001 compared with initial group (reflects response to treatment).
‡P < 0.001 compared with the total grading population (reflects response to treatment).
Headache disability
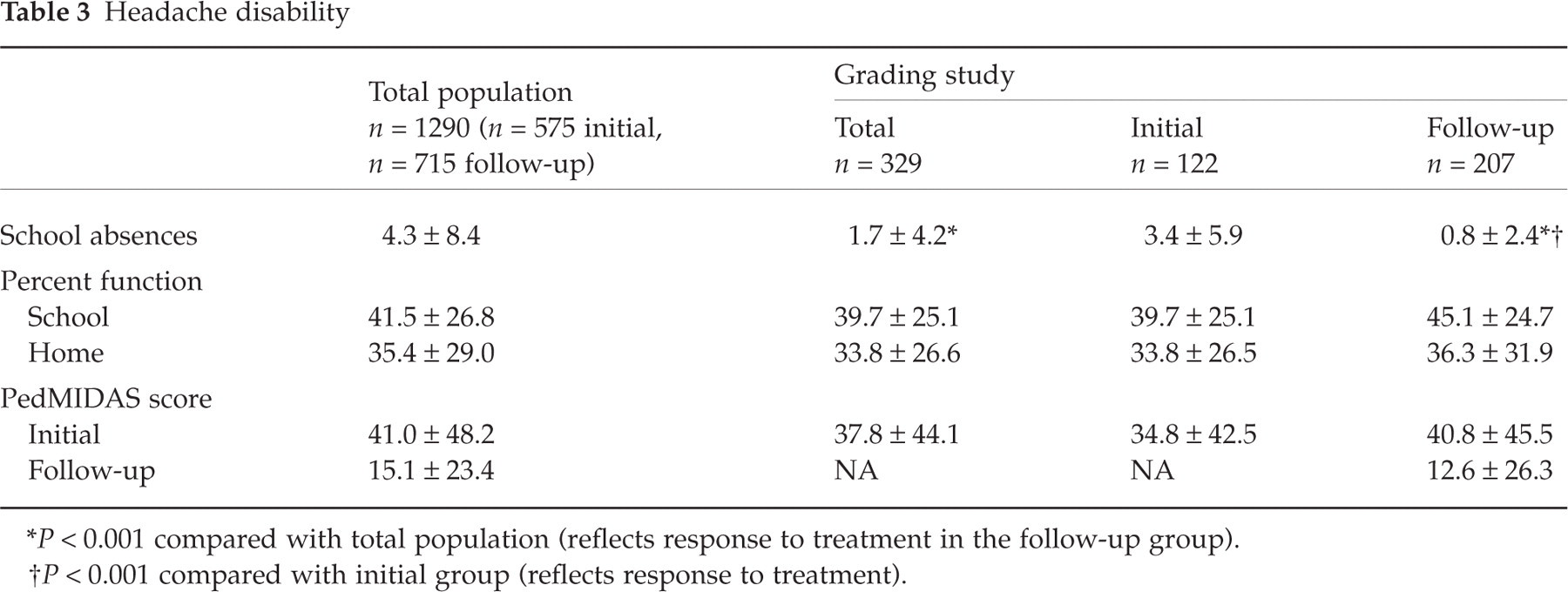
∗P < 0.001 compared with total population (reflects response to treatment in the follow-up group).
†P < 0.001 compared with initial group (reflects response to treatment).
PedMIDAS scoring
The mean PedMIDAS raw score at the initial evaluation for the entire group of patients in this study was 37.8 ± 44.1. This is representative of all the initial PedMIDAS scores obtained at Cincinnati Children's Hospital (4). PedMIDAS scores at presentation for the initial and follow-up groups are comparable (Table 3). For the follow-up group, the PedMIDAS score had improved to 12.6 ± 26.3 compared with 40.8 ± 45.5 at initial presentation (P < 0.0001).
PedMIDAS grading
For the global rating, 163 patients reported their headaches were of little to no disability, 88 reported mild disability, 52 reported moderate disability and 26 reported severe disability. When only the initial 122 patients were asked to rate their disability, 33 patients reported their headache disability was little to none, 36 reported mild disability, 35 reported moderate disability and 18 reported severe disability. An improvement in disability perception is seen in the 207 follow-up patients, where 130 patients reported their headache disability was little to none, 52 reported mild disability, 17 reported moderate disability and eight reported severe disability. Table 4 describes the mean PedMIDAS raw score for each global rating category for the total group, the initial group and the follow-up group.
PedMIDAS grading

∗P < 0.001 for comparison within total, initial, or follow-up groups between global rating scales, except for P = 0.00109 for mild to moderate in the initial group, P = 0.022 for the moderate to severe in the initial group, and P = 0.00125 for the mild to moderate in the follow-up group.
†P < 0.01 for comparison of little to none rating scale between initial and follow-up (reglects response to treatment).
‡P < 0.001 for comparison of mild rating scale between initial and follow-up (reflects response to treatment).
Based on the convergence of patient global ratings with PedMIDAS raw score, a PedMIDAS grading system was developed. Using a principle of non-overlapping ranges this corresponds to Grade I (little to none disability), 0–10; Grade II (mild disability), 11–30; Grade III (moderate disability), 31–50; and Grade IV (severe disability), > 50. Figure 1 shows the relation of patient's global report and the new PedMIDAS grading system. The percentage of patients in the total group is presented.

Correlation of patient reported disability to PedMIDAS grade. Based on the PedMIDAS grading scale developed in this study, a patient's PedMIDAS grade (I, II, III, or IV) was determined from their individual PedMIDAS score (i.e. if their PedMIDAS score was 42 they would be defined as Grade III). This was compared with the patient's self-reported global-rating score (little to none, mild, moderate, or severe). The percentage of patients reporting each global-rating score for each PedMIDAS grade is plotted. For example, 87% of patients reporting a global rating score of little to none had PedMIDAS Grade I, while 55% of patients reporting a global rating score of severe had PedMIDAS Grade IV.
Treatment effects
In the stratified care model for the adult MIDAS, the grading level was used to suggest treatment options (i.e. triptans) (6). When the use of triptans in children was compared with the patient-reported global rating, the results were similar for all follow-up evaluations for all PedMIDAS grades (I, 23%; II, 30%; III, 22%; and IV, 25%). When the PedMIDAS score was used to determine the disability grade (using the new PedMIDAS grading scale), the use of triptans was also similar (I, 19%; II, 28%; III, 22%; and IV, 23%).
For prophylactic therapy, there was a clear differentiation. At the visit starting prophylactic medication, the patient-reported global ratings stratified with increasing likelihood of initiation of prophylactic medication (I, 23%; II, 44%; III, 88%; and IV, 83%; P < 0.001). When the PedMIDAS score was examined (using the new PedMIDAS grading scale), prophylactic medication was more likely to be initiated as the severity increased (I, 20%; II, 49%; III, 83%; and IV, 91%; P < 0.001).
Discussion
Migraines are increasingly recognized as a significant health problem in adults and children. They frequently result in lost time at work, home or school, and decreased social functioning. Classically, the impact of migraine has been measured through an assessment of frequency, severity and duration. This had led in the past to attempts to develop headache indices. More recently, the impact of migraines on a patient's quality of life (12) and the level of disability (4) related to the disorder have been emphasized as more sensitive measures and of more importance to the patient.
In this regard, MIDAS was developed for adults age 20–50. The adult MIDAS provides a simple measure of disability that can be easily used in a busy clinical practice. It yields a raw score, which can measure initial disability and track the improvement in this disability over time. In addition to the raw score, a grading system was developed to characterize the degree of disability based on this raw score. This was developed largely by expert opinion and retrospectively validated using physician-based perception of disability. The grading system has increased the clinical usefulness of the adult MIDAS and is being expanded worldwide. Its usefulness has been demonstrated in comparing the improvement in patient outcome using the stratified care vs step-care model (6, 7).
The adult MIDAS, however, was not designed for children and adolescents and does not involve a developmentally appropriate assessment. PedMIDAS was developed to address this problem and has been validated and proven reliable for this purpose. The adult MIDAS grading system, however, did not accurately correlate with the raw scores for PedMIDAS. Using the adult MIDAS grading system, the PedMIDAS raw score skews the disability to a more severe range than appears to be present. This is probably due to children and adolescents being able to miss out in school, home, and social activities more frequently than adults with less of a consequential disability. For example, missed school days can often be made up, whereas missed days of work result in diminished employer production and lowered job performance. Therefore, a new, empirically derived grading system was needed for PedMIDAS.
A further complication for children and adolescents is correct determination of the impact of disability on their lives. Adults are often inaccurate in assessment of this impact even in their own children (8). This can only be solved by having the young patient rate his or her own disability. Even with this in mind, not all patients may rate their disability appropriately. Patients may over- or underestimate this disability. Therefore, a standardized, patient-based disability grading scale was needed. This study demonstrates that PedMIDAS can provide the raw score and standardizing this score with a large group of patients yields a reproducible grading system of disability. Using the same terms of the adult MIDAS allows the two disability tools to be compared in continuum, thus allowing disability assessment for migraines over all practical age ranges.
The new PedMIDAS grading scale can be easily administered in a busy clinical practice. Whereas the adult MIDAS is based on intervals of ‘5s’ (i.e. little to no disability is a score of 0–5, mild disability 6–10, moderate disability 11–20 and severe disability > 21), the PedMIDAS grading system is based on intervals of ‘10s’ (i.e. little to no disability is a score of 0–10, mild disability 11–30, moderate disability 31–50 and severe disability > 50). The implication is that the appropriate tool can be given to patients based on their age and a resultant disability grade obtained. This grade can then be used to assist in prescribing therapy, with a greater disability indicating the need for prophylactic medications.
This study also demonstrates that the disability grade can be tracked during treatment. PedMIDAS raw scores have been observed to improve with time and the grading scale correlates well with this improvement. Using the patient-based rating, the improvement in the PedMIDAS raw score is seen by the patients as an improvement in their global rating of disability. In a clinical practice, PedMIDAS can therefore be used to demonstrate to the patient how their individual PedMIDAS score is improving with treatment, while their overall disability grade is similarly responding.