
Abstract
Background
While the association between migraine, neck pain, and cervical musculoskeletal dysfunctions is well established in adults, such a relationship remains unclear in the pediatric population. This gap limits our understanding of early pathophysiological mechanisms and hinders the development of targeted interventions.
Objective
To assess self-reported neck pain, pressure pain threshold (PPT), global cervical range of motion (ROM), and upper cervical mobility in children and adolescents with and without migraine.
Methods
A cross-sectional study was conducted with 102 participants in total (51 with migraine – MG – and 51 controls – CG), aged six to 16 years. Neck pain characteristics (presence, frequency, intensity, and duration) were recorded. Cervical ROM was measured in flexion, extension, lateral flexion, and rotation. Upper cervical mobility was evaluated using the Flexion Rotation Test (FRT), and PPT was bilaterally assessed in the sternocleidomastoid, levator scapulae, suboccipital, upper trapezius, and anterior scalene muscles. Comparisons between groups were made using Student's t-test, Mann–Whitney U test, or Chi-square test, with a significance level set at 5%.
Results
Compared to the control group, the MG showed a higher prevalence of neck pain (39.2% vs. 5.9%; p < 0.001) and longer average duration (19 ± 8.6 vs. 8 ± 3.4 h; p = 0.046). Reduced lateral flexion (p < 0.001) and reduced upper cervical mobility (p < 0.001) were observed in the MG. Additionally, all evaluated muscles exhibited significantly lower PPT values in the MG (p < 0.001) than controls, indicating increased pain sensitivity.
Conclusion
Similar to adults, children and adolescents with migraine demonstrate cervical musculoskeletal impairments, including neck pain, reduced cervical mobility—especially in lateral flexion and upper cervical rotation—and heightened sensitivity in craniocervical muscles. These findings support the routine inclusion of cervical musculoskeletal assessments in the clinical management of pediatric migraine.
This is a visual representation of the abstract.
Introduction
Migraine is among the most prevalent primary headaches in the pediatric population, with an estimated global prevalence of 7.8% in individuals under 20 years of age (1). In Brazil, this rate reaches 15%, representing a significant source of disability-adjusted life years in youth and one of the leading reasons for seeking medical care (1–3). Furthermore, pediatric migraine negatively affects quality of life, compromising school attendance and performance, participation in leisure activities, and the ability to engage in daily responsibilities at home (4–6).
Pathophysiologically, migraine involves marked alterations in neural modulation, particularly characterized by neuronal hyperexcitability and central sensitization within the trigeminocervical complex (7,8). This sensitization enhances the transmission of nociceptive signals originating from both trigeminal and upper cervical afferents, leading to neurogenic inflammation and altered sensorimotor perception in the cervical region (8,9). Such mechanisms contribute to the frequent occurrence of referred pain in the neck and head, reinforcing the involvement of the cervical spine in migraine (8,9).
In adults, is well-established that neck pain is highly prevalent among those with migraine (10,11), and its presence is associated with a more severe clinical presentation, increased migraine-related disability (12,13), and higher neck-related functional impairment (14). Adults with migraine also exhibit musculoskeletal cervical dysfunctions, including reduced cervical range of motion (ROM) – particularly in the upper cervical segments (15–17) — and lower pressure pain thresholds (PPT) in craniocervical muscles, indicating peripheral sensitization (18–20).
In contrast, cervical musculoskeletal alterations in pediatric migraine remain poorly investigated. Although 38% of adolescents aged 15 to 18 years report neck pain (21), and neck stiffness is a frequently reported premonitory symptom (22), few studies have examined objective cervical dysfunctions in this population. For example, Anttila et al. (23) reported greater self-perceived tension in the neck and shoulders in 12-year-olds with migraine compared to controls and those with tension-type headache. However, no significant differences in PPT were found, and the analysis lacked muscle-specific detail. Ferracini et al. (24) observed lower PPT values at the occipital insertions and anterior cervical region (C5–C7) in children with migraine aged eight to 12. Meanwhile, a study evaluating cervical ROM in 13-year-olds found no significant differences between migraine, tension-type headache, and control groups (25).
The limited number of studies and their narrow age ranges restrict the generalizability of findings and preclude a comprehensive understanding of cervical dysfunction in children and adolescents with migraine. Given that cervical involvement in adults is consistently associated with symptom severity and treatment responsiveness, it is crucial to determine whether similar patterns occur in younger populations.
Therefore, the aim of this study was to assess cervical musculoskeletal dysfunctions – including global and upper cervical mobility, pressure pain threshold, and the presence and characteristics of neck pain – in children and adolescents with migraine compared to those without headache.
Methods
This cross-sectional study received approval from the institutional Research Ethics Committee (CAAE: 70680023.6.0000.5440). All participants provided age-appropriate assent, and their legal guardians signed an informed consent form detailing the study procedures.
Participants of both sexes, aged six to 16 years, were recruited. The migraine group (MG) comprised patients evaluated at a pediatric headache outpatient clinic of a tertiary hospital between October 2023 and August 2024. Diagnosis was confirmed by an experienced neurologist based on the criteria established in the third edition of the International Classification of Headache Disorders (26). Eligibility required experiencing at least three migraine attacks per month. The control group (CG) included children and adolescents without a history of headaches, recruited from a public school due the practical challenges of identifying and enrolling healthy children and adolescents through other means. Exclusion criteria were diagnoses of headache types other than migraine, neuromuscular or orthopedic conditions, any diagnosed syndrome, attention-deficit/hyperactivity disorder, inconclusive diagnoses, or cognitive inability to follow simple instructions.
Data collected included age, sex, weight, height, physical activity level, and self-reported headache and neck pain characteristics. Migraine characteristics encompassed frequency, intensity (categorized as mild, moderate, severe, or variable), and pain quality (pulsating, pressure-like, burning, undefined, or mixed). Regarding the neck pain, participants were asked to indicate the presence of pain during the last six months. For those reporting pain, frequency, intensity, and duration were assessed with reference to the last month. Both neck pain and migraine intensity were assessed using the Faces Pain Scale–Revised (FPS-R). The FPS-R demonstrates strong convergent validity (r = 0.92 with VAS, r = 0.84 with CAS) in children aged 4–12 years (27), along with evidence of good discriminative validity, responsivity, and reliability across ages 4–17 years (28). To ensure accurate reporting, all assessments were conducted using language appropriate to the developmental level of the participants. In cases where younger children were unable to fully comprehend or respond independently, assistance was provided by a parent or legal guardian during the evaluation process. Cervical musculoskeletal assessment included evaluations of active cervical range of motion (ROM), upper cervical mobility, and pressure pain threshold (PPT). ROM in flexion, extension, lateral flexion, and bilateral rotation was measured using a CROM device (29). In pediatric populations, this test has demonstrated excellent reliability, with inter-rater intraclass correlation coefficient (ICC) of 0.93 and intra-rater ICC of 0.84 (30). The Flexion Rotation Test (FRT) was applied to assess upper cervical mobility (C1/C2), also using the CROM device (29,30). This method shows excellent reliability for all cervical movements in pediatric population, with ICC > 0.70 for all cervical movements (29). PPT was bilaterally assessed using a digital algometer (DDK-20 Kratos) on the sternocleidomastoid, levator scapulae, suboccipital, upper trapezius, and anterior scalene muscles (24,31). Pressure was applied at a constant rate of 0.5 kg/cm²/s, with auditory feedback from a 1 Hz metronome. The order of muscle testing was standardized for all participants, and each point was assessed twice. The PPT presents a moderate to excellent reliability (intra-rater ICC ranging from 0.46 to 0.94) in the pediatric population (32). All assessments were performedby a trained physical therapist.
Statistical analysis
Sample size was calculated using G*Power software, based on pilot data from five participants per group using FRT measurements. Assuming a significance level of α = 0.05 and power (1–β) of 0.80, the minimum required sample size was 47 participants per group.
Descriptive statistics (mean, standard deviation, and percentages) were calculated for all variables. For ROM and PPT, values from both sides were averaged. Between-group comparisons used the Chi-square test for categorical variables and either independent Student's t-tests or Mann–Whitney U tests for continuous variables, depending on distribution. A significance level of p < 0.05 was adopted. Analyses were performed using SPSS version 21 (IBM Corporation, Armonk, NY).
Results
The sample consisted of 102 children and adolescents, with 51 allocated to the migraine group and 51 to the control group. The mean age was 10.8 years in the MG and 10.4 years in the CG. Demographic and clinical characteristics are presented in Table 1. Both groups showed a predominance of females. The MG presented a significantly higher prevalence of self-reported neck pain (39.2%) compared to the CG (5.9%) (p < 0.001), as well as a longer mean duration of neck pain (19.0 h vs. 8.0 h; p = 0.046). The average migraine frequency was 11.5 headache days per month, with a mean age of migraine onset of 6.8 years.
Demographic and clinical characteristics, including migraine and cervical pain features, of children and adolescents with migraine (n = 51) and controls (n = 51).
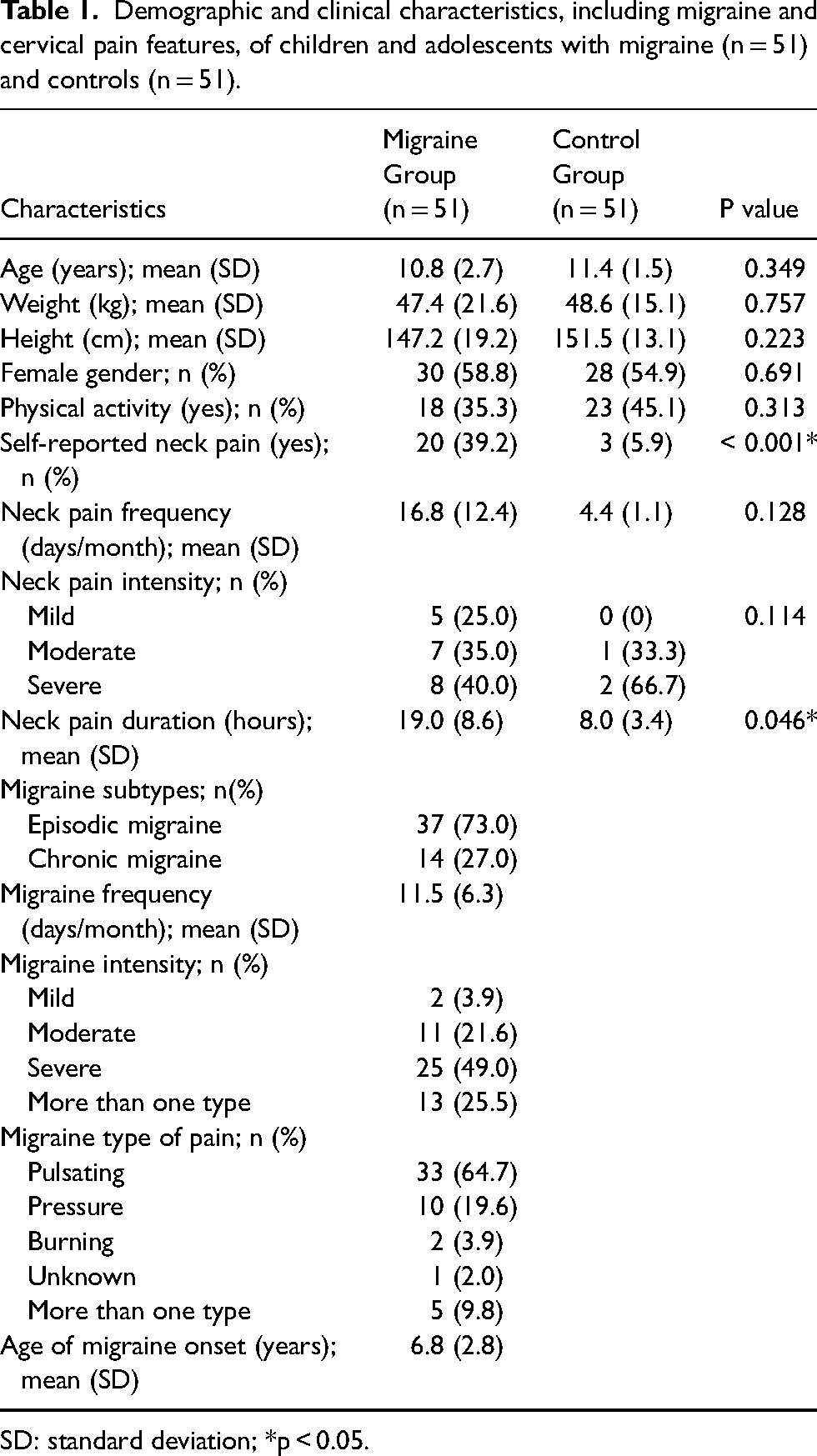
SD: standard deviation; *p < 0.05.
The MG exhibited reduced cervical mobility in lateral flexion (p < 0.001) and in the Flexion Rotation Test (FRT) (p < 0.001) when compared to the CG. Additionally, pressure pain thresholds (PPT) were significantly lower in the MG for all assessed cervical muscles (p < 0.05), indicating greater sensitivity (Table 2).
Mean and standard deviation of global and upper cervical mobility (degrees) and pressure pain threshold (kgf) in cervical muscles of children and adolescents with migraine (n = 51) and controls (n = 51).

ROM: range of motion; FRT: flexion rotation test; PPT: pressure pain threshold; † mean of left and right side; *p < 0.05.
Discussion
Children and adolescents with migraine exhibited a higher prevalence of self-reported neck pain compared to controls (39.2% vs. 5.9%), as well as longer neck pain duration. Additionally, the migraine group demonstrated reduced cervical range of motion (particularly in lateral flexion), decreased upper cervical mobility as assessed by the Flexion Rotation Test (FRT), and lower pressure pain thresholds (PPT) in cervical muscles.
To our knowledge, this is the first study to evaluate upper cervical mobility in children and adolescents with migraine. The FRT is widely used in adults, and previous studies have validated its application in healthy children and adolescents, as well as in those with cervicogenic headache, supporting its feasibility in pediatric populations (33). In adults with migraine, reduced cervical mobility is well documented, and both FRT and global cervical ROM assessments are recommended components of the musculoskeletal evaluation (34). In our study, comparisons within the same age range revealed significantly lower FRT mobility and lateral flexion ROM in the migraine group compared to controls. These findings contrast with those of Oksanen et al. (25), who reported no differences in cervical mobility between adolescents with migraine and controls. However, their sample was restricted to a single school grade, limiting age variability and external validity. When analyzing cervical ROM in younger populations, it is important to consider anatomical and biomechanical particularities of the immature cervical spine, which is generally more mobile than in adults, especially in flexion-extension and rotation (35). Given these differences, one might expect mobility restrictions to be less evident in pediatric populations. In adults, reduced cervical mobility has been associated with higher migraine frequency and increased neck-related disability (15,17); whether these associations are also present in children remains an open question for future research. Nonetheless, our findings suggest that musculoskeletal impairments related to migraine begin in childhood, particularly in the upper cervical region, as evidenced by reduced FRT values. This region, where the upper cervical nerve roots originate, is a known site of increased sensitivity, these roots convey nociceptive afferents to the trigeminocervical complex, and it 's a common therapeutic target in adult migraine (8,36). Epidemiological studies report a 32–36% prevalence of neck pain among children and adolescents in the general population, often linked to ergonomic or behavioral factors such as desk height, posture, or backpack use (37,38). In contrast, only 5.9% of the control group in our study reported neck pain. Since population-based studies rarely stratify participants by headache status, our results underscore the need for more targeted investigations into the specific relationship between migraine and neck pain.
Our findings are supported by Blaschek et al. (21), who reported that 38% of adolescents with migraine experienced neck pain, and that migraine individuals were twice as likely to report neck pain as those without headache (39). This risk increases sevenfold in cases of chronic migraine, even after controlling for confounding variables such as sex, stress, and lifestyle habits (40). Given this evidence – and the low prevalence of neck pain in our control group – our data strengthen the hypothesis that migraine is independently associated with neck pain, and that this association correlates with migraine frequency.
The direct relationship between neck pain and migraine is well established in adults (17,41), where it is not only highly prevalent but also associated with increased attack frequency and risk of chronification (10,41). Our study reinforces the finding that neck pain may also be a core component of the migraine phenotype in children and adolescents as well in adults. Indeed, symptoms such as neck pain, stiffness, and muscle tension have been observed during all migraine phases – including the prodrome, headache, and postdrome – even in pediatric populations (42,43). Although our study did not specifically investigate the temporal relationship between migraine attacks and neck pain, the prolonged duration of neck symptoms in our sample suggests their presence during interictal periods. This phenomenon, also well documented in adults, is thought to result from trigeminal pathway sensitization, which amplifies nociceptive inputs and contributes to pain persistence and migraine chronification (14,17,44).
Mechanistically, cervical musculoskeletal dysfunctions are increasingly recognized as relevant to migraine expression through the convergence of trigeminal and upper cervical afferents, which amplifies nociceptive input, promotes neurogenic inflammation, and contributes to central sensitization (7–9) (Figure 1). These dysfunctions may not represent coincidental comorbidities; rather, they can act as potential triggers by increasing peripheral nociceptive drive or as perpetuating factors by maintaining central excitability. In pediatric populations, this interplay may be further shaped by the ongoing maturation of cervical biomechanics, proprioception, and deep muscle control, which could influence the vulnerability to musculoskeletal dysfunctions and their impact on migraine burden (10,41,45). Within this framework, our findings of higher prevalence of neck pain, reduced cervical range of motion, and lower pressure pain thresholds in the migraine group are consistent with the hypothesis that cervical dysfunctions contribute to the clinical expression of migraine in children—not necessarily as causal drivers, since this is a cross-sectional study, but as modulators that may interact with neurophysiological processes. Thus, early identification and treatment of neck pain could potentially delay or prevent disease progression in this population. Supporting this, recent clinical trial data indicate that both aerobic and cervical exercises can reduce migraine frequency, intensity, and duration in children and adolescents (46).

Hypothesized mechanism linking cervical dysfunction and pediatric migraine.
Our study also found significantly lower PPT values in the cervical muscles of pediatric migraine patients, consistent with previous findings of increased pain sensitivity in the neck and shoulder region (23), suboccipital muscles, and pericranial areas (24). Landgraf et al. (47) further demonstrated that sustained palpation of myofascial trigger points in the neck can provoke migraine attacks in children . Additionally, Pieniak et al. (48) found that pediatric migraine patients exhibited generalized hypersensitivity beyond the cervical region, negatively impacting daily function . These findings highlight the role of altered cervical sensory processing in migraine pathophysiology and suggest the need for targeted therapeutic strategies to modulate this hypersensitivity.
In adults, lower PPTs are observed not only in cervical regions but also in extratrigeminal and pericranial sites (20,49), and this pattern appears independent of disease chronicity, as both episodic and chronic migraine patients exhibit cervical sensitization (17,19,50). Our majority sample was classified as having episodic migraine (73%), and although we did not compare participants by episodic vs. chronic status, our findings indicate that decreased PPT is already present in episodic cases during childhood.
Taken together, these results support the view that migraine-related musculoskeletal impairments begin early and may influence the course of the disease, mirroring the clinical picture seen in adults. In addition to cervical mobility and sensitivity deficits, adults with migraine also present poorer muscle performance, endurance, and strength (17) – aspects that merit further investigation in pediatric populations.
This study has limitations. Its cross-sectional design precludes causal inference and the ability to establish causal relationships between migraine and cervical musculoskeletal findings. The analysis of a wide age range (six – 16 years) may be considered a limitation, as it encompasses different stages of growth and biomechanical development of the cervical spine. However, the present study was not designed to perform age-stratified analyses, which could be addressed in future investigations. The examinator was not blinded to group allocation, which may have introduced assessment bias, and the migraine group was recruited from a tertiary hospital, which may not fully represent the broader population of children and adolescents with migraine, particularly those managed in primary or community-based care. These factors should be considered when interpreting the generalizability of the results. Despite these limitations, strengths of this study include a well-defined and age-diverse sample, children and adolescents were diagnosed with migraine by neurologists specialized in headache disorders, use of standardized and validated assessment tools, and the presentation of clinically relevant and novel findings in pediatric migraine. From a clinical perspective, our results emphasize the importance of investigating neck pain and conducting cervical musculoskeletal evaluations in pediatric migraine. Scientifically, the relationship between cervical dysfunction and migraine characteristics warrants further exploration. Longitudinal studies may reveal whether the severity of cervical dysfunction correlates with migraine progression across developmental stages.
Children and adolescents with migraine, compared to controls, exhibit cervical musculoskeletal dysfunctions, including neck pain, reduced range of motion, and heightened peripheral sensitivity in cervical muscles. These alterations appear to be integral components of migraine clinical presentation, even at early ages. Our findings underscore the importance of including cervical musculoskeletal assessments in the clinical evaluation and management of pediatric migraine.
Footnotes
Consent to participate
All participants provided age-appropriate assent, and their legal guardians signed an informed consent form detailing the study procedures.
Data availability statement
The datasets used and/or analyzed during this study are available from the corresponding authors upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The study protocol was approved by the Institutional Research Ethics Committee of Ribeirão Preto Medical School, University of São Paulo (CAAE: 70680023.6.0000.5440).
Funding
This research was supported by the São Paulo Research Foundation (FAPESP), grant numbers 2023/09538-5 and 2023/12002-2.