
Abstract
Background
The middle meningeal artery is surrounded by a plexus of afferent fibers shown to be involved in the progression of some forms of headache, especially migraine. Posttraumatic headache disorders sharing characteristics with migraine and involving the middle meningeal artery are not readily available in the literature.
Case description
This report describes a posttraumatic headache disorder in a middle-aged woman in which the causative factor proved to be a pathology of the left middle meningeal artery that resulted from trauma. Her pain could be triggered by moderate accelerative changes, occurring in the left frontotemporal region, and shared characteristics with migraine. Resection of a portion of the left middle meningeal artery has completely eliminated her pain syndrome.
Conclusion
This case further elucidates associations between the middle meningeal artery and headache. The presentation of posttraumatic headache sharing characteristics with migraine should suggest the possibility of a middle meningeal artery abnormality.
Introduction
The dura mater and its vasculature are pain-producing intracranial structures that have long been implicated in the pathogenesis of headache (1,2,8). The middle meningeal artery (MMA) is a major vascular constituent of the dura mater and is densely innervated by afferent fibers of the trigeminal nerve (2,3). Vasodilation and mechanical stimulation of the MMA in awake patients have been associated with the production of pain in the frontotemporal region that is consistent with symptoms of headache (1,4), although mechanical perturbation of the MMA is a rarely considered source of posttraumatic headache. A case of recurrent headache induced by physical activity is shown to have developed as a result of tethering of the MMA and dura following traumatic head injury. Consent was received directly from the patient as required by the Institutional Review Board of Spectrum Health.
Case description
A 48-year-old Caucasian woman presented with a two-year history of recurrent left frontal headache. These began following an experience on a rollercoaster in which she was subjected to strong centrifugal forces. Six years prior to this experience, she had suffered a concussion with a loss of consciousness exceeding 10 minutes when she was struck on the left forehead in a waterslide incident. Computed tomography showed no overt cerebral contusion. She had no history of headache prior to this incident or the rollercoaster event. Her pain was characterized as a constant pressing sensation in the left frontotemporal region and was punctuated by extreme lancinating pain during relatively minor physical activity or exertion. Descending stairs, coughing, and Valsalva maneuvers were stated examples of such episodes. The patient also had a history of a dysautonomic condition causing substantial elevations in systolic blood pressure exceeding 200 mmHg. These events initiated a severe pulsating pain in the territory of her left frontotemporal headache. The correlation between blood pressure spikes and headache was observed in hospital while the patient was monitored. The patient reported no instances of sensitivity to light or sound in association with her headaches, although nausea was reported, at most, on two occasions when her headaches were particularly severe. Selective carotid angiography revealed multifocal narrowing of the posterior division of the left middle meningeal artery (MMA; Figure 1). Contrast injection and submaximal balloon angioplasty of the left posterior MMA intensely reproduced her characteristic left frontal lancinating pain. Subsequent intra-arterial verapamil injection failed to provide relief, although injection of local anesthetic did provide relief. Surgical exposure revealed the dura to be strongly adherent to the inner table of the cranium with a calcified pseudomembranous outer layer. A long segment of the MMA was removed from the level of the foramen spinosum along with adjacent pseudomembrane. Pathological study showed near circumferential calcification of the tunica adventitia of the posterior MMA segment in particular (Figure 2). The patient has been free of her presenting headache for 6 months.
Angiographic image showing the irregular multifocal narrowing of the posterior division of the left middle meningeal artery (see arrows). The patient's pain was reproduced with manipulation of the vessel and relieved by lidocaine injection. Photomicrograph of a hematoxylin and eosin stained section identifying the posterior branch of the middle meningeal artery and showing patchy areas of calcium deposition in the adventitia and neighboring dura (see arrows). Sequential sections of the artery identified circumferential involvement of the adventitia by calcium.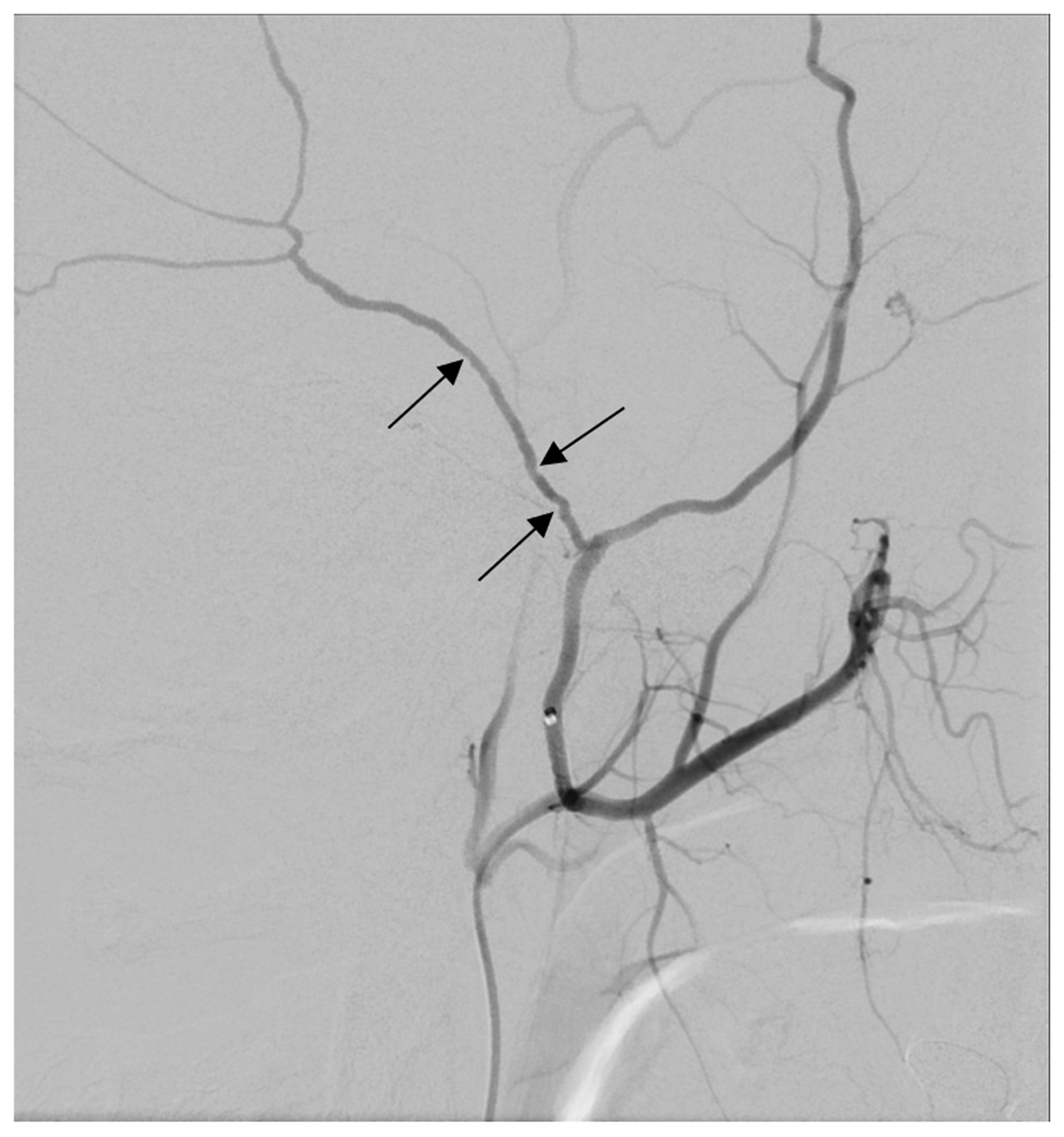

Discussion
An unusual headache presentation attributable to adhesion and traction of the middle meningeal artery against the inner calvarium provides some insight into the nature of headache localized to this area and the categorization of posttraumatic headache. The tethering of such an acutely sensitive site as the proximal distribution of the MMA underlies the mechanism of pain induction by such relatively innocuous activities as descending stairs. Both contrast injection and transient ballooning of the artery accurately reproduced the pain while lidocaine injection eliminated it. Surgical removal of the artery and subsequent elimination of symptoms affirmed the cause was attributable to the adherence of the vascular structure and neighboring dura to the calvarium. Dural adhesion against the calvarium was ostensibly a consequence of the resolution of a posttraumatic epidural hemorrhage. The onset of the headache syndrome from the time of this patient's rollercoaster incident is thought to have resulted from the centrifugal force applied to a tethered MMA such as to induce sufficient traction upon local nociceptors to have perpetuated the problem.
The relationship between innervation of dural arteries and headache disorders, especially migraine, has been studied extensively. The headache phase of a migraine has been closely associated with the activation of intracranial paravascular nociceptive pathways (5), which originate primarily from the trigeminal nerve (2). Nociception within the dural vasculature is mediated by unmyelinated (C fibers) and myelinated (Aδ) axons that surround vessels and form a plexus (6). Activation of these fibers by electrical, chemical, or mechanical stimulation activates the trigeminovascular system and produces headaches that emulate features of migraine (7). Two recent studies have found that MMA circumference increases ipsilaterally during the onset of one-sided migraine attacks (4,8), with significantly less dilation (8) or no dilation (4) of the contralateral MMA. This association supports the notion that nociception along meningeal vasculature plays a significant role in headache. It remains unclear, however, whether vasodilation of the MMA represents a causative factor in headache, a point emphasized by another study that recorded MMA vasodilation without headache (9). The elimination of this patient's headache by removal of a pathological MMA supports the notion of a meningeal origin for some forms of headache.
Surgical treatment for migraine headache has gained popularity in recent years, especially those targeting extracranial trigger sites. A recent meta-analysis of such procedures determined a migraine-elimination rate of 38%, although varying methodologies and documentation make it difficult to form a consensus on surgery as a treatment for migraine (10). Surgical treatments for migraine targeting the MMA have also demonstrated some efficacy. Ligation of the MMA, superficial temporal artery, and greater superficial petrosal nerve has provided relief in some cases of intractable migraine (11). Despite sharing some characteristics with migraine – durations exceeding 4 hours, a pulsatile quality, persistent unilateral features, aggravation by routine physical activity – this patient's headaches were not migrainous by definition, according to the third edition of the International Classification of Headache Disorders criteria (12). Rather, her headache disorder would be characterized as being posttraumatic by causation and induced by a subsequent event when a strong centrifugal force was exerted upon a tethered MMA that resulted from the earlier trauma. In this sense, the current timeframe of 6 years following trauma far exceeds the standard definition of delayed onset persistent posttraumatic headache, which extends to 3 months (12). Hence, this case describes a two-stage process whereby vulnerability was created by an initial traumatic event, but headache induction followed a second unrelated circumstance. It remains of interest, however, that the MMA has been so strongly implicated in the progression of migraine headaches and its resection brought about relief of some of the symptoms of migraine in this patient's posttraumatic headache syndrome.
Here, we demonstrate that head trauma can bring about a headache syndrome attributable to the tethering of the MMA to the cranium, and that resection of the pathological vessel can provide relief. A surgical approach is not without risk of CSF leakage, infection, or postoperative hematoma; the benefit in this situation far exceeded the risk. Presentation of posttraumatic headache sharing some features of migraine and consistently in a specific frontotemporal distribution may suggest the possibility of an MMA abnormality, for which further study may elucidate a source amenable to surgical correction.
Footnotes
Clinical implications
Traumatic head injury disrupting the middle meningeal artery can cause recurrent headache that emulates migraine.
Resection of the disrupted artery can eliminate the headache syndrome.
A direct association exists between the middle meningeal artery and some features of headache.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.