
Abstract
Background
Posttraumatic headache is difficult to define and there is debate about the specificity of the 7-day headache onset criterion in the current definition. There is limited evidence available to guide decision making about this criterion.
Method
A nested cohort study of 193 treatment-seeking veterans who met criteria for persistent headache attributed to mild traumatic injury to the head, including some veterans with delayed headache onset up to 90 days post-injury, was undertaken. Survival analysis examined the proportion of participants reporting headache over time and differences in these proportions based on sex, headache phenotype, and mechanism of injury.
Result
127 participants (66%; 95% CI: 59–72%) reported headache onset within 7 days of head injury and 65 (34%) reported headache onset between 8 days and 3 months after head injury. Fourteen percent of participants reported pre-existing migraine before head injury, and there was no difference in the proportion of veterans with pre-existing migraine based on headache onset. Headache onset times were not associated with sex, headache phenotype, or mechanism of injury. There were no significant differences in proportion of veterans with headache onset within 7 days of head injury based on headache phenotype (70% migraine onset within 7 days, 70% tension-type headache within 7 days, 56% cluster headache within 7 days; p ≥ .364). Similar findings were observed for head injury (64% blast, 60% blunt; p = .973). There were no significant differences observed between headache onset groups for psychiatric symptoms (Posttraumatic Stress Disorder Checklist for DSM-5 = 1.3, 95% CI = −27.5, 30.1; Patient Health Questionnaire-9 Item = 3.5, 95% CI = −6.3, 3.7; Generalized Anxiety Disorder Screener = 6.5, 95% CI = −2.7, 15.6).
Conclusions
Although most of the sample reported headache onset within 7 days of head injury, one-third experienced an onset outside of the diagnostic range. Additionally, veterans with headache onset within 7 days of head injury were not meaningfully different from those with later onset based on sex, headache phenotype, or mechanism of head injury. The ICHD-3 diagnostic criteria for 7-day headache onset should be expanded to 3 months.
ClinicalTrials.gov Identifier
NCT02419131
Abbreviations
ANCOVA: Analysis of Covariance; CI: confidence interval; DSM-5: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; GAD-7: Generalized Anxiety Disorder Screener; HIT-6: Headache Impact Test; HR: Hazard Ratio; ICHD-2: International Classification of Headache Disorders, 2nd edition; ICHD-3: International Classification of Headache Disorders, 3rd edition; ISI: Insomnia Severity Index; LL: Lower Limit of Confidence Interval; PHQ-9: Patient Health Questionnaire-9 Item; PCL-5: PTSD Checklist for DSM-5; PTH: posttraumatic headache; PTSD: posttraumatic stress disorder; UL: Upper Limit of Confidence Interval.
Introduction
Interest in posttraumatic headache (PTH) has grown significantly over the past 20 years, with annual publications for PTH in PubMed growing from 307 listings in 2000 to over 1300 listings in 2020. Because of its high likelihood for persistence, PTH investigators continue to promulgate PTH research to develop novel treatments that address PTH symptoms and disability (1). A precise and consistent definition is vital to ensure that accumulating data can be meaningfully interpreted and used as a foundation for subsequent advancements in PTH diagnosis and treatment. The third edition of the International Classification of Headache Disorders (ICHD-3, (2)) made few alterations to PTH definition from the second edition of the ICHD (3) and maintained a clinical definition of headache meaningfully linked in time to an injury to the head or neck without defining clinical characteristics. The ICHD-3 requires development of new or worsened headache within 7 days of head injury (or recovery from loss of consciousness), though the International Headache Society Headache Classification Committee clarifies that this 7-day criterion maximizes diagnostic specificity but is “somewhat arbitrary” and subject to revision as new evidence arises (2). The first edition of the ICHD required a 14-day latency between head injury and headache onset, but this was narrowed to 7 days in the second ICHD edition due to concerns about the high prevalence of primary headache in the general population that may be mistakenly classified as posttraumatic (4).
Indeed, there is some controversy surrounding the 7-day onset criterion for PTH, with little emerging evidence to guide decisions about changing this requirement. One study of headache after traumatic brain injury reported that new headaches develop after 7 days for over 25% of individuals with a head injury (5), leading some to recommend that causality of head injury for novel headache should be a clinical decision with onset allowed to vary beyond 7 days (up to 90 days in some cases; cf. (6)). The ICHD-3 (2) includes appendix criteria for “delayed-onset” posttraumatic headache that allows for headache onset between 7 days and 3 months after injury. Thus, researchers can use these delayed-onset criteria to meaningfully compare early (within 7 days) and delayed headache onset patients as a test of the 7-day onset criterion. If the existing 7-day onset latency criterion for PTH is meaningfully contributing to diagnostic specificity, then there should be noticeable phenotypic differences between patients with headache onset within 7 days and delayed onset that are attributable to unique headache mechanisms associated with traumatic injury. The International Classification of Headache Disorders includes varying criteria based on the mechanism of injury leading to posttraumatic headache, including traumatic injury to the head (criteria 5.1 and 5.2), whiplash (criteria 5.3 and 5.4) and craniotomy (criteria 5.5 and 5.6). Differences in pathogenesis of posttraumatic headache can result in different symptom and treatment patterns, so these “sub-types” of posttraumatic headache may not represent a homogeneous patient population. Of the three posttraumatic headache injury mechanisms covered in the ICHD-3, headache attributable to head injury is the most common. Whiplash-related headache occurs in approximately 300 per 100,000 people (7), and posttraumatic headache occurs in up to 30% of individuals who undergo craniotomy, though craniotomy is rare in the general population (8).
Traumatic brain injury (TBI) is increasingly common in both civilian and military populations, and persistent posttraumatic headache attributable to TBI may account for 4% of all secondary headaches (9). Headache attributable to head injury has received the most attention among posttraumatic headache subtypes due to its prevalence, and headache attributable to mild head injury has received the most attention due to the high likelihood of headache persistence after mild TBI (10). There is some debate about the relationship between head injury severity and posttraumatic headache (11), but studies of headache after head injury show strong evidence of increased headache risk after any head injury. For example, a study of 212 individuals with mild head injury treated at a level 1 trauma center found headache onset or worsening up to one year after mild TBI, with over 50% of individuals with mild head injury reporting headache immediately after injury, and at 3, 6 and 12 months post-injury (12). A natural history study of 316 patients with moderate or severe head injury found a similar high risk of headache long after head injury with over one third of patients reporting headache onset or worsening at 3 months, 6 months, 1 year and 5 years after moderate and severe TBI (13).
Diagnostic precision is important because unreliable diagnosis can lead to miscommunication between providers, unnecessary diagnostic testing, poor treatment matching, and prolonged patient suffering (14,15). Posttraumatic headache is particularly vexing because of the difficulty establishing causation between head or neck injury and headache onset or exacerbation. Multiple resources can strengthen diagnostic precision including the use of established diagnostic criteria, clinical examination, use of biomarkers, functional testing and symptom self-report (16–18). Integrating multiple sources of data confirmed by consensus clinical judgment may bolster clinical precision in establishing an “ideal” clinical threshold of posttraumatic headache onset. Establishing an “ideal” threshold for the sensitivity of PTH diagnosis is challenging because concepts like sensitivity, specificity and positive/negative predictive value are highly contextual (19). Thus, we chose a conservative value of 80% as a threshold value for the 7-day headache onset definition as a sensitive criterion for PTH diagnosis. The present study is a nested cohort study of data from 193 veterans recruited for a randomized clinical trial of a nonpharmacological intervention for posttraumatic headache, and the analytic strategy for this cohort study was developed to address the following aims: Aim 1: Identify the proportion of study patients reporting headache onset within 7 days of mild traumatic brain injury. Hypothesis 1: Over 80% of the sample will report headache onset within 7 days of head injury regardless of sex, headache phenotype and head injury mechanism. Aim 2: Examine differences in headache severity and comorbid symptom presentation between patients with headache onset within 7 days of mild traumatic brain injury and those with delayed onset. Hypothesis 2: Participants with headache onset within 7 days of head injury will report more severe headache (based on headache-related disability, intensity, and frequency/duration of episodes) and more severe symptoms of anxiety, depression and insomnia compared to those with delayed headache onset (between 8 days and 3 months).
Methods
The present study is a nested cohort study of data from a randomized clinical trial supported by the Consortium to Alleviate PTSD, a nationwide posttraumatic stress disorder (PTSD) research consortium jointly funded in 2013 by the Department of Defense and the Department of Veterans Affairs. Study participants were 193 US military veterans recruited from May 2015 to May 2019 through primary care, polytrauma, and neurology clinics at a large Veterans Affairs (VA) hospital in the southern United States. The study protocol was approved by the VA and university institutional review board (protocol number HSC20140339H, ClinicalTrials.gov Identifier: NCT02419131), and all study participants provided written informed consent prior to participating in research activities. Patients were screened for headache symptoms using a structured diagnostic interview for headache between May 2015 and May 2019 and completed a structured diagnostic interview for posttraumatic stress disorder. To qualify for enrollment, patients had to meet modified ICHD-2 and ICHD-3 criteria for persistent posttraumatic headache related to head injury, which included all criteria for ICHD-3 A5.2 Persistent headache attributed to mild traumatic injury to the head or ICHD-3 A.5.2.2.1 Delayed-onset persistent headache attributed to mild traumatic injury to the head (which allows for delayed onset of headache up to 3 months after injury). Qualified participants were also required to report clinically significant symptoms of posttraumatic stress symptoms including exposure to a traumatic event, one or more intrusion symptoms, and one or more avoidance symptoms.
To bolster clinical precision of PTH diagnosis, ICHD-3 criteria were supplemented by clinical judgment to assure that headache onset/exacerbation was reasonably attributable to head injury among participants with delayed headache onset. Clinical judgment for posttraumatic headache diagnosis included retrospective review of patient medical records to confirm clinical attribution of headache to head injury, patient confirmation that headache was related to head injury during baseline research clinical interview, and consensus between the study Principal Investigator, research investigators and clinical physicians that headache was reasonably attributable to the reported head injury. When available, imaging data (fMRI, head CT) were used to confirm mild TBI and rule out other causes of headache. This process occurred as an interactive discussion between the three collaborators, who were not blinded to one another’s determination (blinding was not used because consensus required discussion and collaborative interpretation of diagnostic and medical record data). Data for the present study are derived from baseline assessments.
All patients completed validated structured diagnostic interviews for headache (Structured Diagnostic Interview for Headache (SDIH) (20)) and PTSD (Clinician Administered PTSD Scale for the DSM-5 (21)) at baseline assessment, both of which were administered by a trained independent evaluator. The SDIH was developed by Dr Don Penzien as a structured interview assessing headache characteristics using a format that maps headache symptoms directly to ICHD-3 criteria for primary headache, posttraumatic headache, and medication overuse headache. The SDIH has been used in numerous studies of headache (e.g. (22–24)). Participants also completed a number of prospective self-report measures for headache and comorbid conditions including a valid and reliable assessment of headache-related disability (6-Item Headache Impact Test (HIT-6) (25)), Primary Care Evaluation of Mental Disorders modules measuring anxiety (Generalized Anxiety Disorder Screener (GAD-7) (26)) and depression (Patient Health Questionnaire-9 Item (PHQ-9) (27)), a gold-standard screening assessment for PTSD symptom severity (PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (PCL-5) (28)), a standardized insomnia symptom measure (Insomnia Severity Index (ISI) (29)), a structured clinical interview to assess recent and lifetime head injury, and a standardized 7-day REDCap headache diary (30). All research data were double entered into a secure SQL database by an independent research assistant.
Statistical analyses
This analysis is a secondary analysis of baseline information from the parent clinical trial that was powered to examine treatment differences in several cognitive-behavioral therapies. This analysis was conducted using all available data but was not powered to detect a priori defined differences among onset latency subgroups. To facilitate interpretation, all point estimates are reported along with 95% CI to allow interpretation of the size of the effects along with their uncertainty. After consideration of survival assumptions, examination and comparison of headache onset latency after head injury were illustrated using Kaplan-Meier survival estimates (31) using NCSS 2020 version 20.0.2. Analysis focused on Hazard curves and Cox Hazard ratio coefficients with 95% confidence intervals as the most informative and valid option for illustrating risk for headache onset by time (32,33). Study data were dummy-coded to identify participants who reported headache onset from 0–7 days after head injury (coded as “1”) and those reporting headache onset after 7 days (coded as “2”) for pair-wise comparisons of headache intensity and comorbidity variables. Because sex-based differences may influence outcomes of interest for this study, comparisons between these two groups accounted for sex as a covariate. Kaplan-Meier curve 95% CIs were calculated using log-minus-log transformation as a conservative option with estimates closer to nominal values (34). Where appropriate, all analyses are two-tailed with p < 0.05 used to determine statistical significance.
Results
The baseline, nested cohort sample of 193 US military veterans were represented mostly by white (58%), non-Hispanic (58%) males (91%), as shown in Table 1. All participants reported headache associated with mild traumatic brain injury and none reported a history of craniotomy. Approximately 16% of the sample reported comorbid whiplash at the time of their head injury to which they also attributed their headache. A higher proportion of participants with comorbid mild TBI and whiplash reported headache onset within 7 days (73%) compared to those with headache attributable to mild TBI only (65%), but Chi-square analysis revealed no statistically significant difference (χ2 = 0.782, p = .377). The most common headache phenotypes in this nested cohort sample were migraine headache (36%) and “other” headache (35%), which included mixed headache and presentations that did not fit criteria for either migraine or tension-type headache. Cluster headache phenotype was reported by 17% of participants, and 13% reported a tension-type headache. There were no cases of medication overuse headache, which was an exclusion for the randomized clinical trial. Almost half of the sample reported headache onset associated with a blast-related injury (48%), and participants reported an average of four lifetime head injuries. Overall, the sample reported headaches of severe intensity with an average numeric rating scale score of 6.9/10 and 14 episodes per month with an average duration of 827 minutes (13.8 hours; see Table 2). There were no missing data for any of the demographic variables or headache phenotypes. Missing data for head injury and headache characteristics are described below.
Continuous demographic summary for full sample with comparison between veterans with headache onset within 7 days and within 3 months.

*There were no missing demographic data at baseline.
**Based on independent samples t-test.
Categorical demographic summary for full sample with comparison between veterans with headache onset within 7 days and within 3 months.

*There were no missing demographic data at baseline.
**Based on Chi-square.
The Kaplan Meier survival plot for reported headache onset after head injury of the entire study sample is presented in Figure 1. Overall, 66% of the sample reported headache onset within 7 days (95% CI: 59–72%), many of whom (41%) reported headache within 1 day of head injury (95% CI: 34–48%). Notably, there were still 29% of patients who had not yet reported headache onset by 14 days post-injury (95% CI: 22–35%) and 21% who had not yet reported headache onset by 60 days post-injury (95% CI: 15–27%).

Kaplan-Meier Survival Curve for full sample (n = 192) with 95% confidence interval.
Hazard model coefficient ratio (HR) examined differences in headache onset between males and females and revealed a non-significant difference in headache onset latency by time between the two sex groups (HR = 1.26, 95% CI: 0.021, 74.0, p = .910). It is of note that the small number of women in the sample (approximately 10%) produced sparse data for relative risk. Figure 2 shows equivalent slopes for headache onset between both sexes with 35% (95% CI: 14–57%) of females reporting headache after 7 days and 34% (95% CI: 27–41%) of males. Approximately 35% (95% CI: 18–62%) of females reported headache onset within 1 day of head injury, but almost 24% (95% CI: 4–38%) reported onset 60–90 days after head injury. Just over 40% (95% CI: 34–49%) of males reported headache onset within 1 day of head injury, but over 21% (95% CI: 15–27%) reported onset 60–90 days post-injury.

Kaplan-Meier Survival Curve by sex (female = 17, male = 175) with 95% confidence interval.
Headache onset was then examined based on headache phenotype (established using structured diagnostic interview, electronic health record review and expert consensus, see Figure 3). Chi-square analysis of headache phenotype revealed no statistically significant difference in the proportion of patients fitting specific headache phenotypes by headache onset (χ2 = 1.472, p = .688). To maintain clarity, 95% confidence intervals are provided in Figure 3 for patients with migraine (dark grey) and tension-type (light grey) symptoms only. Once again, the Hazard Ratio model coefficients were non-significant across all pairwise ratios (summarized in Table 3), suggesting no meaningful difference in the slopes of the Kaplan Meier curves between the four headache phenotypes. Approximately 70% percent of patients who fit migraine (95% CI: 61–80%) and tension-type (95% CI: 53–87%) headache phenotypes reported headache onset within 7 days of head injury, but 14% (95% CI: 7–23%) of migraine type and 13% (95% CI: 3–29%) of tension type patients did not report headache until 60–90 days after injury. Examination of pre-injury headache data (based on patient report and review of medical record) revealed that 14% of the nested cohort sample reported a migraine diagnosis before head injury and there was no significant difference in rates of pre-injury migraine between those with post-injury headache onset within 7 days or with delayed onset (χ2 = 0.002, p = .967).

Kaplan-Meier Survival Curve by headache symptom type (migraine = 70, tension-type = 24, cluster = 32, other/mixed = 66) with 95% confidence interval.
Pairwise hazard ratios across all four clinical phenotype groups.

*There were no missing headache phenotype data at baseline.
A smaller proportion of patients with cluster headache phenotype (59%) reported headache onset within 7 days of head injury (95% CI: 40–74%) compared to other headache types, and 64% of those who did not fit a specific phenotype reported onset within 7 days (95% CI: 53–75%). Sixty days after head injury, there were still 34% of patients with cluster symptoms (95% CI: 19–51%) and 24% of “other” headache patients (95% CI: 15–35%) who had not yet reported headache onset.
Headache onset proportions were evaluated to identify differences in headache onset latency by head injury type, shown in Figure 4. Three datapoints were censored (two at 1-day onset and one at 75-day onset) due to lack of information about the nature of the head injury. Hazard ratios, shown in Table 4, revealed no significant difference between patients reporting headache caused by blast versus blunt injury (e.g. blunt trauma; HR = 1.16, p = .360), blast versus combined (an injury that included both blunt and blast trauma; HR = 0.97, p = .890) and blunt versus combined (HR = 0.84, p = .428). More patients with headache caused by a combination of blast and blunt trauma (76%; 95% CI: 60–89%) reported headache onset within 7 days than those with headache caused by blast injury (64%; CI: 57–76%) or blunt injury (60%; CI: 48–72%) only. Approximately 18% of patients with blast (95% CI: 11–27%) and combined blast and blunt injury (95% CI: 7–33%) reported headache onset after 60 days, while 25% of those with a blunt head trauma (95% CI: 15–36%) reported headache onset after 60 days.
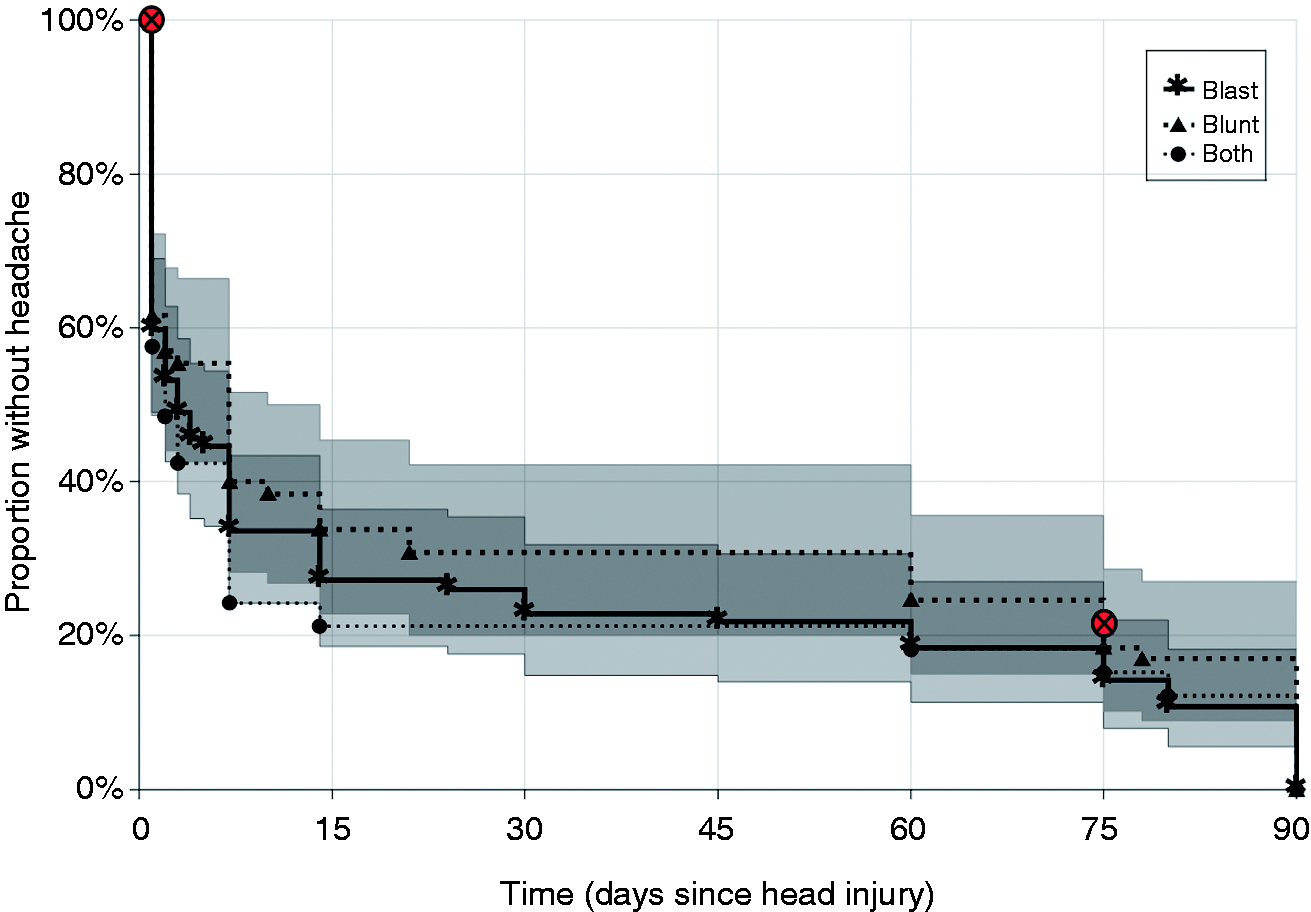
Kaplan-Meier Survival Curve by head-injury mechanism (blast = 92, blunt = 65, both = 33) with 95% confidence interval.
Pairwise hazard ratios across all four clinical phenotype groups.

*Missing data from two participants who could not recall the mechanism of their head injury.
Finally, to examine clinical sensitivity of a 7-day onset criterion for posttraumatic headache, patients reporting headache onset within 7 days (n = 127) and after 7 days (n = 65) were compared on frequency of headache symptoms, head injury severity and severity of comorbid conditions using analysis of covariance (ANCOVA) to account for sex-based differences. Data for headache symptoms and comorbid conditions are summarized in Table 5. All analyzed variables had complete data with the exception of headache duration (missing data from 25 participants who reported that they were unsure of the duration of their last headache) and headache frequency (missing data from one participant who reported that he could not recall the frequency of his headaches). ANCOVA revealed no significant differences in headache intensity (p = .364), frequency of headache episodes per month (p = .877) and duration of headache episodes in minutes (p = .999). There was no significant difference in headache-related disability between participants with 7-day and delayed headache onset based on total HIT-6 score (p = .973). Participants with headache onset within 7 days reported slightly more lifetime head injuries than those with onset beyond 7 days, though ANCOVA revealed no significant between-groups difference when controlling for sex (p = .635). The two groups did not differ significantly on any of the comorbid psychiatric symptom measures.
Comparison of headache severity and comorbid symptoms between patients with headache onset within 7 days and those with onset after 7 days.

*Headache duration data missing for 25 participants who reported that they were unsure how long their last headache lasted; headache frequency data missing from one participant.
Discussion
The present study represents an examination of a large, nested cohort sample of veterans with posttraumatic headache attributable to mild head injury. Findings from this analysis offer some of the first evidence supporting expansion of the posttraumatic headache onset criterion from 7 days to 3 months. There were several important strengths of this study that support the value of the findings to the field. First, the sample was purposely designed to include individuals who met diagnostic and research criteria for headache attributable to a mild injury to the head. Although the sample was not balanced, enrollment reflected a surprisingly high proportion of veterans with delayed headache onset (approximately 30%) who were phenotypically similar to those with 7-day onset. The sizable sample of delayed onset participants allowed for one of the first clinical comparisons of early and delayed-onset posttraumatic headache. Second, in recognition of the difficulty establishing a causal link between head injury and delayed onset headache, the research team establish a multi-component process for confirming a reasonable likelihood of causation. All participants completed a structured clinical interview for headache, and Veterans Affairs medical records were reviewed to identify collateral diagnosis of posttraumatic headache by clinical providers. When available, relevant diagnostic test results were reviewed, and all delayed-onset cases were discussed between research staff and expert clinicians to ensure a consensus of posttraumatic headache. Finally, the sample chosen for this study represents only a portion of individuals with posttraumatic headache (i.e. headache attributable to mild trauma to the head), but mild TBI is highly prevalent and individuals with headache attributable to mild TBI represent a significant proportion of individuals with persistent posttraumatic headache worldwide.
Diagnostic precision is vital in guiding the growing body of research on PTH mechanisms and treatment, but there has been some concern that the current ICHD-3 criterion for 7-day headache onset is too restrictive. In order to promote the conduct of high quality research to better understand the applicability of the ICHD-3 7-day criterion, Appendix 5.2 offers an expanded time window such that “the maximal time interval between head injury and headache onset is set at 3 months”. The present study relied on rigorous medical record review and consensus from at least three clinicians to establish that headache was related to head injury and allowed onset to extend up to 3 months post-head injury. Most of the sample enrolled in this trial reported headache onset within 7 days of injury, but a large proportion of participants reported headache onset after the 7-day latency criterion established by the ICHD-3, including 20% who reported headache onset up to 3 months after head injury. Notably, there was no significant difference based on headache onset latency between sex, headache phenotype, and head injury mechanism groups. Furthermore, indices of headache severity and comorbidity did not differ between those who developed headache within 7 days compared to with delayed onset. All reported posttraumatic headaches clinically resembled one another regardless of when they began after head trauma, and this lack of distinction casts some doubt about the sensitivity of the ICHD 7-day onset criterion while highlighting the arbitrary nature of how posttraumatic headache is operationally defined under current criteria. Restricting the onset criterion for posttraumatic headache to a narrow 7-day range is concerning because emerging data (similar to what is presented in this study) increasingly shows that up to 20–30% of individuals with head injury are likely to report headache onset after 7 days (6,35). Thus, the narrow definition of posttraumatic headache established in the ICHD-3 is incompatible with the growing body of research on headache after traumatic brain injury that includes individuals with headache alteration or onset beyond 7 days after the injury (cf. (36)).
There is increasing recognition that central pain processes (i.e. central sensitization) are strongly implicated in headache experience and disability (37,38). Posttraumatic headache, by definition, occurs in the context of significant trauma that can give rise to biopsychosocial problems that may significantly impact how headache pain is processed (39). The sample examined for this study was required to present with both headache and comorbid trauma symptoms. Posttraumatic stress disorder (PTSD) commonly co-occurs with traumatic head injury (40), and individuals with enduring PTSD symptoms are vulnerable to trauma-related headache as long as PTSD is present. Furthermore, alterations in mood and sleep after head injury can raise the risk for headache onset or alteration through direct and indirect mechanisms (10,41,42). Headache pain is subjective, and delay in reported onset after head injury is dependent on patient and situational factors that could affect pain processing and headache symptom awareness. Military service members, for example, experience numerous distractions during deployment that may delay notice or report of headache after a head injury that may not be discussed with a healthcare provider until post-deployment examination (43). Thus, strict adherence to a 7-day onset criterion may artificially misclassify service members with posttraumatic headache due to delayed reporting or distraction. There is additional concern that the complex matrix of clinical comorbidities that accompany posttraumatic headache may add risk of headache misclassification bias. For example, headache attributed to head injury may be secondary to PTSD, depression or insomnia that accompany head injury, rather than attributable to the head injury itself. This distinction is vital because the putative mechanisms of headache may vary based on the cause, resulting in different treatment recommendations. Prospective trajectory studies of posttraumatic headache and comorbid psychiatric conditions are needed to develop more robust models of PTH that can help distinguish between headache secondary to head injury or other trauma comorbidities.
There are limitations to the present study. First, the clinical trial from which this nested cohort sample was derived included US military veterans with comorbid posttraumatic headache and clinically significant posttraumatic stress symptoms. The presence of comorbid PTSD symptoms could affect pain phenotype (44,45). Interestingly, one study of military personnel with headache after traumatic brain injury reported that PTSD may not contribute to headache prevalence (46) though it does contribute significantly to headache-related disability (47). Regardless, PTSD co-occurs with head injury and headache at high rates in both military (48) and civilian populations (49), so the sample examined in this study is likely representative of a large portion of PTH sufferers. The research team recruited clinical trial participants through the VA community and across multiple clinics. Part of recruitment included education for providers about the possibility of a causal link between head injury and headache even when onset is beyond 7 days. This education may have influenced referral patterns that were biased toward longer headache latency. It is equally likely, however, that the sample was skewed toward short-term onset based on referring providers who adhere closely to existing diagnostic criteria for posttraumatic headache and mistakenly identify posttraumatic headache with delayed onset as primary headache.
Although analyses showed no significant sex-based differences in headache onset, the proportion of females in this study was small (10%) and analyses of sex-based differences are likely underpowered. Sex differences are highly relevant in both posttraumatic headache and traumatic brain injury (50,51), so future studies of sex in these populations are strongly encouraged. Because the sample chosen for this study included veterans with military service-related headache, most of the sample included in this nested cohort reported headache onset over 1 year prior to study enrollment. The long delay between headache onset and study enrollment resulted in a sample with significant headache chronification who may have had difficulty recalling specific dates and circumstances of headache onset. We implemented a multi-pronged approach to establishing caseness in this study to protect against bias in delayed recall. All participants completed a structured diagnostic headache interview and interview data were corroborated with retrospective VA medical records (including relevant diagnostic data) that were more proximal to the date of head injury and included disability discharge records detailing military injury. Additional review of military medical records would have added to diagnostic precision, but these records were unavailable to the research team during this study. Future studies of military samples would benefit from including military medical records. Headache attributable to mild TBI is at relatively high risk for long-term persistence (52), and many individuals who develop persistent PTH will report headache up to 4 years after injury (53). Thus, combining increased diagnostic rigor with the likelihood of long-term headache persistence after mTBI, the diagnostic precision of the present study is believed to be reasonably high.
Larger, population-based studies are needed to assess a broader onset inclusion criterion for posttraumatic headache, though the rigor of clinical judgment used in this study highlights that there are individuals with headache that started beyond 7 days post-injury who clinically fit the spirit of the causation criterion in the ICHD-3 criteria. Data from this nested cohort sample relied on baseline assessment and do not shed light on response to treatment that may differentiate headaches based on onset latency. The parent randomized clinical trial for this study has completed the treatment and follow-up phases and is pending publication of the study outcomes. Treatment outcomes data from the randomized trial will be evaluated for influence of onset latency in future outcomes publications. The present study is a secondary analysis of a large PTH clinical trial and was not powered for direct comparisons of PTH with onset before and after 7 days. However, the data presented in this nested cohort study offer compelling evidence that the 7-day onset criterion should be examined further. Finally, the sample used for this nested cohort analysis focused specifically on headache attributable to mild head injury. The findings of this study offer support for possible revision of the ICHD-3 criteria for head onset after mild TBI but may not be representative of individuals with headache attributable to mechanisms other than mild TBI or from non-military samples. Because of the high frequency of mild TBI among military veterans, we anticipate that findings from this nested cohort study likely apply to many persistent posttraumatic headache sufferers worldwide. The present sample found mean headache frequency of 14 headaches per month, which is less frequent than reports from some posttraumatic headache studies (cf. (54)) but matches data from other military TBI samples (55). Lower than expected headache frequency may also be due to recall bias associated with a long delay between headache onset and headache assessment, which is endemic to military service-related pain.
This nested cohort study represents a large and robust examination of headache onset latency in posttraumatic headache. Outcomes from baseline data revealed no significant differences in study participants reporting posttraumatic headache onset within 7 days of head injury or between 8 and 90 days of injury. These findings cast serious doubt on the sensitivity of the existing 7-day headache onset criterion in the ICHD-3 and it is recommended that the onset criterion for headache attributable to mild injury to the head be revised to 3 months, as currently reflected in the ICHD-3 Appendix. Additional studies evaluating this criterion are needed to guide decisions on revision or preservation of the existing criterion, especially for non-TBI injuries. Future research including treatment outcomes and neuroimaging data are needed to better understand the etiology of PTH. Scientific confirmation of an appropriately sensitive onset criterion for PTH is vital to ensure that all patients with PTH receive appropriate attention in the research literature and have access to PTH-specific treatments as they develop.
Key findings
There is some debate about the specificity of the 7-day ICHD-3 onset criterion for posttraumatic headache. Up to one-third of veterans with clinically confirmed posttraumatic headache report onset beyond the 7-day ICHD-3 criterion. There were no significant demographic, phenotypic, or clinical differences between veterans with headache onset before and after the 7-day cut-off. Findings from this nested cohort analysis support review and possible revision of the ICHD-3 criteria for posttraumatic headache.
Footnotes
Additional contributions
We would like to thank Juan Carlos Aguilera, Antoinette Brundige, Deanne Hargita, Clara Stiefel, Rachel Rosenfield, Daisy Rodriguez, Suheily Valderrama, Nicole Brackins, and Adrianna Cole for their research support on this project.
Disclaimer
The views expressed herein are solely those of the authors and do not reflect an endorsement by or the official policy or position of the Department of Veterans Affairs, the Department of Defense, or the US Government.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Consortium to Alleviate PTSD award numbers W81XWH-13-2-0065 from the U.S. Department of Defense, Defense Health Program, Psychological Health and Traumatic Brain Injury Research Program (PH/TBI RP), and I01CX001136-01 from the U.S. Department of Veterans Affairs, Office of Research & Development, Clinical Science Research & Development Service.
Role of the funding source
The funding sources were not involved in the study design, the collection, analysis and interpretation of data, the writing of this report, or the decision to submit this article for publication.