
Abstract
Objective
This prospective, longitudinal cohort study examined the trajectory, classification, and features of posttraumatic headache after pediatric mild traumatic brain injury.
Methods
Children (N = 213; ages 8.00 to 16.99 years) were recruited from two pediatric emergency departments <24 hours of sustaining a mild traumatic brain injury or mild orthopedic injury. At 10 days, three months, and six months postinjury, parents completed a standardized questionnaire that was used to classify premorbid and posttraumatic headache as migraine, tension-type headache, or not otherwise classified. Multilevel mixed effects models were used to examine posttraumatic headache rate, severity, frequency, and duration in relation to group, time postinjury, and premorbid headache, controlling for age, sex, and site.
Results
PTH risk was greater after mild traumatic brain injury than mild orthopedic injury at 10 days (odds ratio = 197.41, p < .001) and three months postinjury (odds ratio = 3.50, p = .030), especially in children without premorbid headache. Posttraumatic headache was more frequent after mild traumatic brain injury than mild orthopedic injury, β (95% confidence interval) = 0.80 (0.05, 1.55). Groups did not differ in other examined headache features and classification any time postinjury.
Conclusions
Posttraumatic headache risk increases after mild traumatic brain injury relative to mild orthopedic injury for approximately three months postinjury, but is not clearly associated with a distinct phenotype.
Keywords
Introduction
Mild traumatic brain injury (mTBI; i.e., concussion) affects over 1 million children annually (1). Children with mTBI often experience somatic, cognitive, and affective symptoms (2). These symptoms typically resolve by one month postinjury, but approximately 15–25% of affected children experience persistent symptoms (2). Posttraumatic headache (PTH) is a common symptom after mTBI (3,4), yet its rate, trajectory, risk factors, and clinical presentation in children remain poorly understood (3,5). Acute PTH has been found in up to 96% of pediatric patients, with incidence varying across studies (4). Following mTBI, older children (i.e., 11–18 years) (4–6) and females (5) have shown increased risk of PTH relative to younger children (i.e., ages 5–12 years) and males, but not always (7). Some research suggests that premorbid (i.e., pre-injury) headache history could be another important risk factor (8), but no known study has examined age at injury, sex, and premorbid headache simultaneously as risk factors for PTH in pediatric mTBI. Also unknown is whether premorbid headache features are worsened by mTBI or differ from those of PTH. Further, migraine (i.e., a neurological disease characterized by recurrent moderate-severe headaches and symptoms such as nausea, vomiting, photophobia, or phonophobia) (9) has been reported to be a common phenotype of PTH and is associated with poorer recovery following mTBI (4,7,8). However, direct comparisons of different subtypes of PTH, such as migraine versus tension-type headache (TTH; i.e., a neurological disease characterized by recurrent mild-moderate headaches without nausea, vomiting, photophobia, or phonophobia), are lacking. Finally, PTH characteristics may also vary over time following pediatric mTBI (10), warranting longitudinal investigation.
Addressing the aforementioned knowledge gaps has important implications for prognostication and medical decision-making for children with mTBI (11). Therefore, this prospective, longitudinal study had two main aims: 1) to investigate the rate, trajectory, risk factors, and features of PTH after mTBI; and 2) to examine PTH classification after mTBI. Children with mild orthopedic injury (OI) were included for comparison based on their similarity to children with mTBI in key pre- and postinjury factors (12). Rates of PTH at early (i.e., ∼10 days) and chronic postinjury periods were expected to be greater after mTBI than OI, and especially in children who were older, female, and had premorbid headache (4). Finally, PTH characteristics following pediatric mTBI were expected to be consistent with criteria for migraine more often than for TTH or headache not otherwise classified (NOC) (3,7,8).
Methods
General procedure
Data were drawn from a large, prospective, longitudinal cohort study of outcomes following pediatric mTBI (13). Children aged 8–16.99 years were recruited within 24 hours of sustaining an mTBI or a mild OI during initial emergency department visits at two children’s hospitals in the USA between 2014 and 2017. Information about the injury and acute signs and symptoms were collected along with basic demographic information by medical personnel using a standard injury case report form at the emergency department visit. Participants returned for one early postinjury (i.e., ∼10 days) and two chronic postinjury (i.e., three months and six months) assessments. Participants completed MRI scanning at the early postinjury assessment, which were coded for incidental and trauma-related findings that have been reported previously (14). Briefly, most children had a normal MRI (i.e., 51%) and only four children with mTBI demonstrated trauma-related findings; the rate of incidental findings (e.g., cysts, white matter hyperintensities, mucosal thickening) did not differ significantly between the two injury groups and the presence of incidental findings was not related to outcomes (14).
Standard protocol approvals, registrations, and patient consents
The study was conducted with the institutional review board at each institution. Participants provided informed assent when appropriate and parents/guardians provided written informed consent.
Data availability
Anonymized data will be shared by request from any qualified investigator.
Participants
Mild traumatic brain injury
Children were included in the mTBI group if they sustained a head trauma resulting in at least one of the following criteria, consistent with World Health Organization criteria (15): 1) observed loss of consciousness <30 minutes; 2) Glasgow Coma Scale (16) score of 13 or 14; or 3)
Mild orthopedic injury
Children were included in the OI group following an upper or lower extremity extracranial fracture that resulted in an Abbreviated Injury Scale (AIS) score <4 (17). Children with OI were excluded if they had any probable or suspected head trauma, any acute signs or symptoms of traumatic brain injury, or if they required surgical intervention or sedative medication.
Exclusion criteria
Additional exclusion criteria for both groups included: 1) any severe injury (i.e., AIS score
Headache measures
Headache questionnaire
Parents of enrolled participants completed a standardized questionnaire at the emergency department visit and at all follow-up visits to assess premorbid headache and PTH, respectively (see online
Classification
For children with premorbid headache or PTH, questionnaire responses were classified according to ICHD-3 criteria (20) as migraine or probable migraine, TTH or probable TTH, or headache not otherwise classified (NOC; see Table 1).
Classification criteria for headache subtype at all timepoints, adapted from ICHD-3.
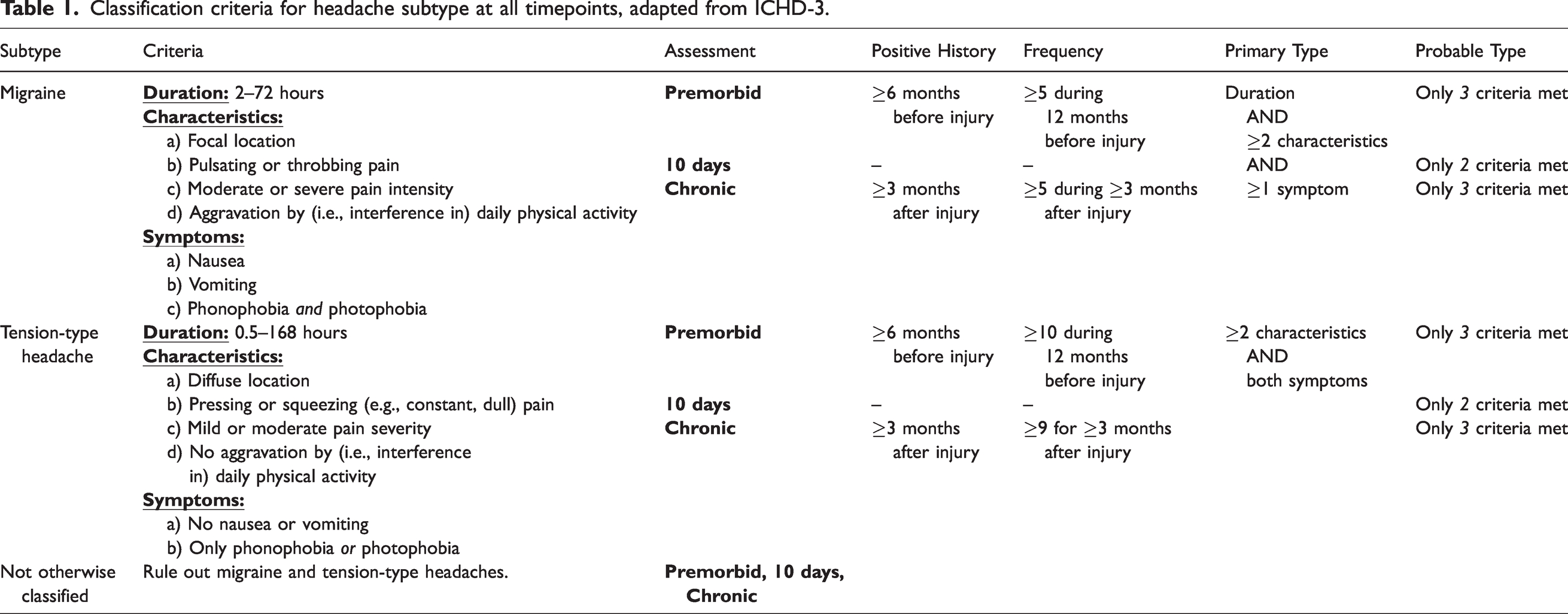
Migraine
Migraine criteria included a headache duration of 2-72 hours; any nausea, vomiting, or combined phonophobia and photophobia; and any two of the characteristics listed in Table 1. Premorbid migraine additionally required headache history
Tension-type headache
TTH criteria required excluding migraine or probable migraine, headache duration of 0.5-168 hours, no more than one of phonophobia or photophobia, neither nausea nor vomiting, and any two of the characteristics listed in Table 1. Premorbid TTH classification additionally required headache history
Not otherwise classified
Headaches that did not meet criteria for migraine, probable migraine, TTH, or probable TTH were treated as not otherwise classified (NOC).
Headache characteristics
Headache frequency, duration, and severity were rated based on the items listed in Table 2. Worsening headache was defined as PTH with an increase in frequency or severity that met worsening headache criteria (see Table 2) compared to premorbid levels, according to the ICHD-3 definition and criteria used in clinical practice (20).
Criteria for worsening headache.

Statistical analysis
Group differences in demographic variables were examined with
Results
Sample
As previously described (13), consent was obtained for 315 children who completed the initial (emergency department) assessment; 217 (69%), 159 (50%), and 143 (45%) of those children returned for the 10-day, three-month, and six-month assessments, respectively. This rate of attrition is consistent with other pediatric mTBI studies (12,23). Premorbid headache questionnaire data were complete for 311 (99%; 192 mTBI/119 OI) children. Of those, 211 (68%; 138 mTBI/73 OI), 158 (51%; 102 mTBI/56 OI), and 143 (46%; 97 mTBI/46 OI) had headache data at 10 days, three months, and six months postinjury, respectively; two children without data at 10 days had data at three and six months postinjury. Therefore, the final sample consisted of 213 children (139 mTBI/74 OI) with complete data for premorbid and at least one postinjury assessment. For the final sample of children, longitudinal data were available at all assessments for 129 (61%; 86 mTBI/43 OI) children, at premorbid and two postinjury assessments for 41 (19%; 26 mTBI/15 OI) children, and at premorbid and one postinjury assessment for 43 (20%; 27 mTBI/16 OI) children. Children included in the final sample did not differ from those who were not included in terms of age at injury, sex, socio-economic status (i.e., a standardized composite of maternal education in years, 2010 median family income for the family census tract, and occupational status), mechanism of injury, or injury setting (i.e., sport/recreational play) (35), but differed in distribution of race, with a higher proportion of White children in the final sample relative to those who were not included, χ2(1) = 11.37, p < .001.
Demographic and injury characteristics
Sociodemographic and injury characteristics of the final sample are reported in Table 3. The groups did not differ in age at injury, sex, Full Scale IQ, or injury setting. Significantly more children with mTBI were White compared to the OI group. Additionally, children with mTBI reported higher socio-economic status and different mechanism of injury than children with OI. In univariate comparisons, premorbid headache and PTH at all timepoints were reported more frequently among children with mTBI relative to OI. Proportionately more children with mTBI than OI reported taking headache medications to prevent or treat PTH at all follow-up visits, with the rates of headache medication usage paralleling the rates of headache reported in each group.
Demographic data for children with mTBI or OI.
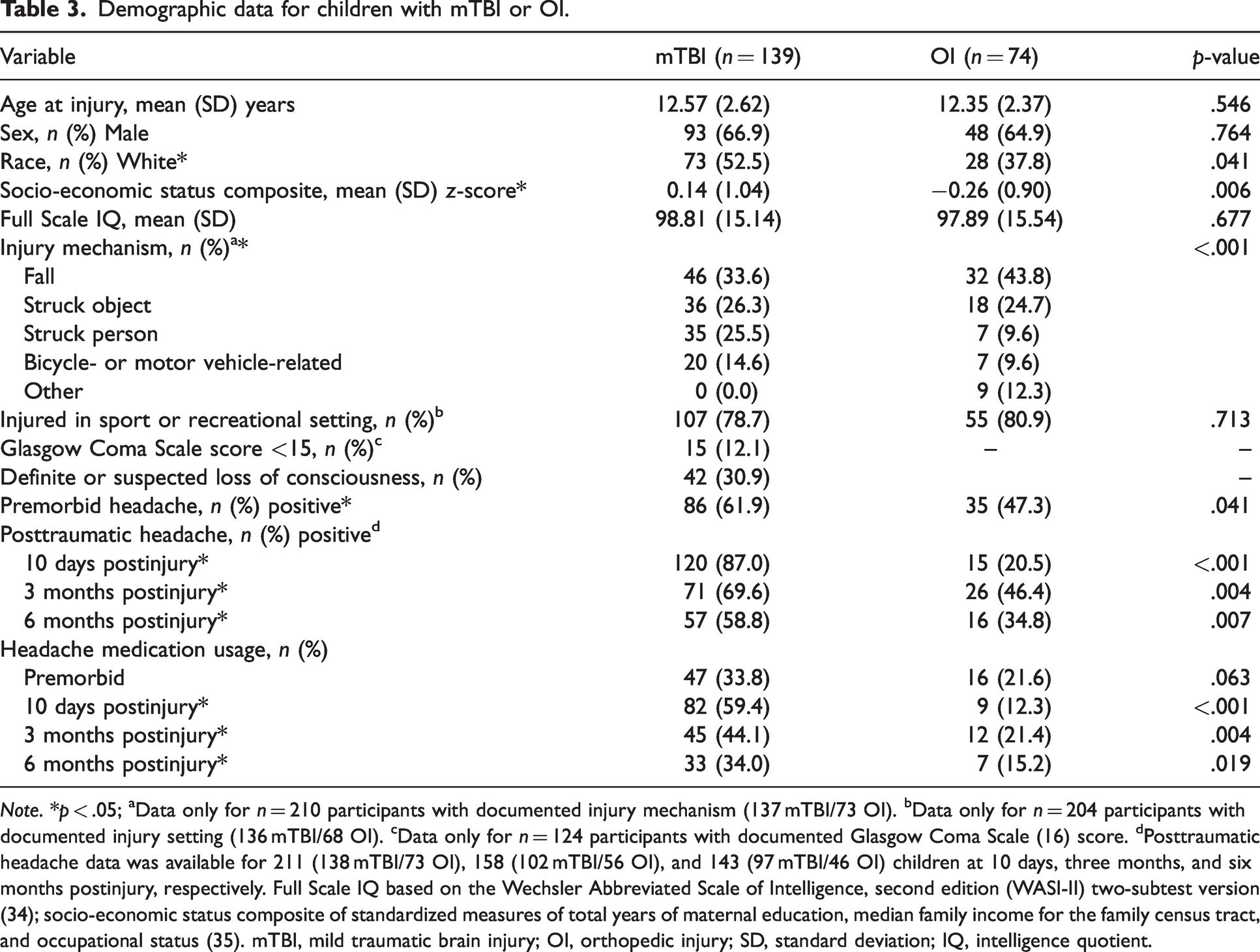
Note. *p < .05; aData only for n = 210 participants with documented injury mechanism (137 mTBI/73 OI). bData only for n = 204 participants with documented injury setting (136 mTBI/68 OI). cData only for n = 124 participants with documented Glasgow Coma Scale (16) score. dPosttraumatic headache data was available for 211 (138 mTBI/73 OI), 158 (102 mTBI/56 OI), and 143 (97 mTBI/46 OI) children at 10 days, three months, and six months postinjury, respectively. Full Scale IQ based on the Wechsler Abbreviated Scale of Intelligence, second edition (WASI-II) two-subtest version (34); socio-economic status composite of standardized measures of total years of maternal education, median family income for the family census tract, and occupational status (35). mTBI, mild traumatic brain injury; OI, orthopedic injury; SD, standard deviation; IQ, intelligence quotient.
Premorbid and posttraumatic headache
Statistical results and odds ratios for the final models for PTH rate, frequency, duration, and severity are summarized in Table 4.
Multivariate model results for posttraumatic headache rate, frequency, duration, and severity, with group, time postinjury, premorbid headache, age, sex, and site included as model predictors.

Note. Data on posttraumatic headache rate was available for 211 (138 mTBI/73 OI), 158 (102 mTBI/56 OI), and 143 (97 mTBI/46 OI) children at 10 days, 3 months, and 6 months postinjury, respectively. Data for headache frequency, duration, and severity were available for 121, 114, and 121 children at premorbid; 132, 125, and 135 participants at 10 days postinjury; 94, 97, and 97 participants at 3 months postinjury; and 73, 72, and 73 participants at 6 months postinjury.
Rates
The three-way interaction between group, premorbid headache, and time postinjury was not significant and was excluded from the final model for rate of PTH (Table 4). However, the group by time interaction was significant; the rate of PTH (see Table 3) was higher following mTBI than OI at 10 days and three months postinjury but did not differ between groups at six months postinjury (Figure 1). The rate of PTH was also higher for children with premorbid headache. Although the interaction was not significant, the group difference in the rate of PTH was larger in children without versus with premorbid headache. The rate of PTH was higher in older than younger children.

Group differences in rate of PTH were moderated by time postinjury and premorbid headache. Error bars represent 95% confidence intervals.
Frequency, duration and severity
Only one child in the OI group without premorbid headache reported PTH at 10 days postinjury, precluding inclusion of the interaction between group, premorbid headache, and time postinjury in final models for headache frequency, duration, and severity (Table 4). Headache frequency was greater after mTBI relative to OI, and decreased over time in both groups, but the interaction between group and time was not significant (Figure 2). Headaches were also more frequent for females than males. Groups did not differ in headache duration or severity. Duration was longer for children with premorbid headache, females, and older children in both injury groups. Headache severity was worse for children with premorbid headache and those from the Cleveland site and decreased over time.
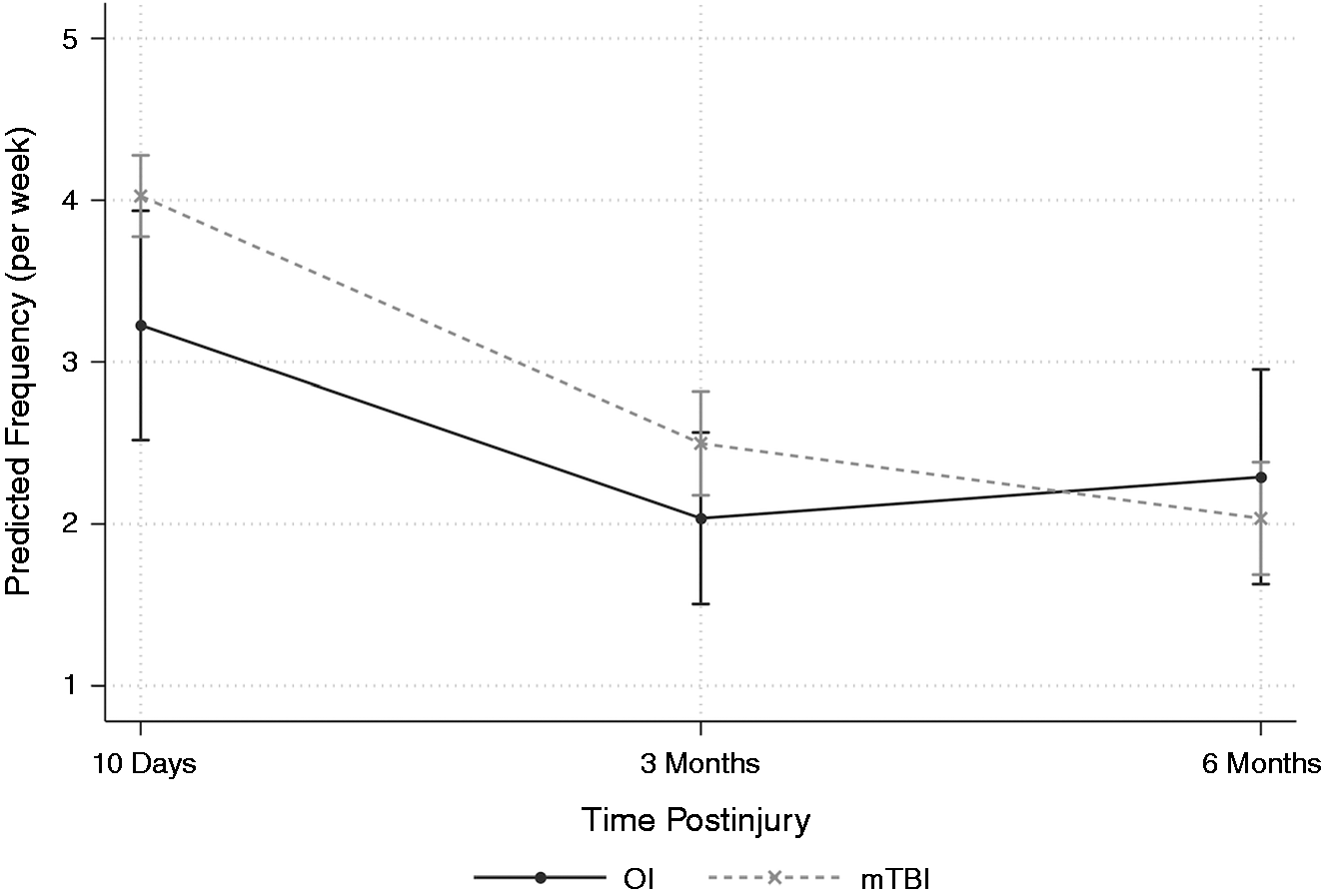
Group differences in PTH frequency across time. Error bars represent 95% confidence intervals.
Worsening
Children with both premorbid headache and PTH, and for whom premorbid headache and PTH frequency or severity data were available (10 days/three months/six months postinjury n = 91/72/54), were examined for worsening headache. Rates of worsening headache did not differ by group at any time postinjury (see Figure 3).

Proportion of children with worsening headache (top) and headache classification by group at each assessment (bottom).
Classification
To increase cell sizes, probable subtypes were combined with each primary subtype (e.g., migraine and probable migraine). Group comparisons of PTH classification are summarized in Figure 3. Rates of migraine, TTH, and NOC did not differ significantly between groups at any time postinjury.
Discussion
This prospective, longitudinal cohort study examined trajectory, clinical features, and classification of PTH following pediatric mTBI relative to mild OI. We also simultaneously examined age at injury, sex, and premorbid headache as risk factors for PTH in pediatric mTBI. Premorbid headache was reported in over half of the sample overall, with modestly greater occurrence in children with mTBI, consistent with rates of pediatric headache (i.e., ∼60% of children and adolescents) in population-based studies (9). Both premorbid headache and time postinjury moderated group differences in the rate of PTH. PTH was more common after mTBI than OI up to three months postinjury, consistent with previous findings of PTH (6). This suggests that PTH can persist longer than other common post-concussive symptoms, which typically recover to their general premorbid symptom status by one month postinjury in children (2). Although the groups differed at a univariate level on PTH rate at six months postinjury, multivariate models, which were longitudinal and included several covariates (i.e., age, sex, and premorbid headache), yielded no significant group differences at this timepoint. This suggests that the univariate difference might be accounted for by the covariates, and particularly by the group difference in premorbid headache. Overall, children were at particularly higher risk for PTH after mTBI relative to OI, regardless of their premorbid headache histories, and experienced more frequent headaches. However, other headache features, including duration, severity, subtype, and worsening headache, did not differ between groups across time postinjury, suggesting that pediatric mTBI is not clearly associated with a distinct phenotype of PTH.
Risk of PTH was greater up to three months following mTBI and especially for children without premorbid headache, indicating that headache onset immediately after injury could reflect specific and early effects of pediatric mTBI. This is consistent with the reported role of head trauma as a leading cause of PTH in pediatric emergency departments (24). Still, the mechanisms underlying PTH, as well as the neurobiology of both pediatric mTBI and headache, are complex and poorly understood (6,11,25). Pediatric mTBI can alter brain tissue and function through a cascade of neurobiological effects, many of which could lead to PTH (11,26). For instance, a disrupted blood-brain barrier, increased intracranial pressure, and neuronal excitability following mTBI might contribute to headache in children (11,26). Moreover, the pathophysiology of headache differs between diagnostic subtypes (e.g., migraine vs. TTH; for detailed review, see Blume (26)). Further research is needed to determine the neurobiology of PTH after pediatric mTBI.
Increased risk of PTH could also be related to several psychosocial factors both common to mTBI and associated with pediatric headache disorders. For example, psychological distress and impoverished sleep are common post-concussive symptoms and leading triggers of pediatric headache (27). Interestingly, they are implicated in migraine as well as TTH (24), both of which occurred in our mTBI group. Consistent with other studies, we found that older children and females demonstrated higher risk of headache and prolonged headache duration (4–6). Both of these factors are also associated with pediatric headache disorders (24,26). In general, more somatic symptoms are reported in girls (through self- or parent report) after traumatic injury (13), and girls exhibit greater risk of protracted recovery following mTBI (2,6,28). We did not investigate whether sex moderated age-related differences in this study, given limited statistical power.
In our examination of the rates of specific subtypes of PTH and worsening headache symptoms, mTBI resulted in neither a distinct headache subtype nor worse headaches relative to premorbid history. However, while no statistically significant group differences emerged in PTH classification, migraine was more prevalent in the mTBI group early postinjury than TTH. Considering that rates of pediatric migraine (7–10%) are lower than TTH (10–24%) in population-based samples (24,26), these results could indicate important clinical differences that were not significant because of limited statistical power. Previous research has suggested that pediatric mTBI most commonly leads to migraine, although few studies have directly compared headache subtypes (4,7,8). Some studies focus on select subtypes (e.g., migraine) (29), but we examined rates of migraine, TTH, and NOC. Additionally, the measures used in previous studies to classify headache symptoms into discrete subtypes have been nonspecific to headache (e.g., the Post-Concussive Symptom Inventory) (30) or used older classification (e.g., ICHD-II) (8) criteria. In contrast, we employed a standardized headache questionnaire that specifically addressed headache symptoms and allowed us to classify headaches according to the gold standard ICHD-3 criteria.
Pediatric mTBI was associated with increased headache frequency, which decreased in both groups by three months postinjury, but was not differentially associated with increased headache duration or severity relative to OI. The reasons for increased headache frequency after mTBI are uncertain. Neurophysiological changes associated with cortical spreading depression and/or trigeminal activation changes could contribute to increased headache frequency (31). Growing evidence also suggests that somatic pain is associated with disrupted brain function after mTBI (25). Other pathophysiological processes may also increase headache frequency. Future research is needed to delineate the effects of pain and associated neurophysiological changes on PTH symptoms in mTBI.
This study has several limitations. Although attrition rates were similar to those of other studies of pediatric mTBI (12,23), the absence of a group difference in the prevalence of PTH at six months postinjury in our multivariate models might have reflected reduced statistical power at that timepoint. Additionally, participants recruited from pediatric emergency departments may not be representative of children in other clinical settings or those who do not seek care (32). We also examined headache based on parent report; while parent and child reports typically correlate, prior studies show that they provide different information about children’s symptoms (33). Moreover, this approach could yield imprecise estimates of headache features and symptoms. Further, some studies suggest that familial history of headache or migraine (4,8) contributes to PTH. However, a detailed family headache history was not collected in our study. Future research incorporating both parent and child reports, as well as family headache history, would be informative. Finally, we did not specifically examine the effect of headache medications on rates of PTH, as this was outside the scope of our study. Nevertheless, rates of medication use mirrored headache rate in both groups, suggesting that the current results are not influenced by medication use.
Conclusions
PTH appears specific to the early effects of pediatric mTBI, with risk increasing relative to OI within the initial weeks and up to three months postinjury. Pediatric mTBI is also associated with increased headache frequency compared to more general traumatic injury. Headache classification did not distinguish children with mTBI from those with OI, suggesting that pediatric mTBI may not result in a distinct phenotype of PTH. However, rates of migraine in children with mTBI seem to be greater than that of the general population. The results highlight the need to identify specific neurobiological mechanisms that influence PTH after pediatric mTBI and to develop interventions to help affected children manage PTH. Future investigations into the relationship between PTH and other outcomes of pediatric mTBI could improve prognostication and help guide clinical management.
Article highlights
PTH appears specific to the early effects of mTBI. Risk of PTH increases in children with mTBI relative to children with OI for up to three months postinjury; however, there are no significant group differences by six months postinjury. No distinct phenotype was found to be clearly associated with PTH after mTBI.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024231161740 - Supplemental material for Longitudinal trajectories of posttraumatic headache after pediatric mild traumatic brain injury
Supplemental material, sj-pdf-1-cep-10.1177_03331024231161740 for Longitudinal trajectories of posttraumatic headache after pediatric mild traumatic brain injury by Mica Gabrielle Marbil, Ashley L Ware, Jean-Michel Galarneau, Nori Mercuri Minich, Andrew D Hershey, Serena L Orr, Dana M Defta, H Gerry Taylor, Erin D Bigler, Daniel M Cohen, Leslie K Mihalov, Ann Bacevice, Barbara A Bangert and Keith Owen Yeates in Cephalalgia
Footnotes
Acknowledgments
We acknowledge Rainbow Babies & Children’s Hospital, University Hospitals Cleveland Medical Center, Nationwide Children’s Hospital, and Case Western Reserve University for the assistance provided with recruitment. We acknowledge the contributions of Emma Lissemore, Anne Birnbaum, Elizabeth Roth, and Taylor Wong from Case Western Reserve University and Rainbow Babies & Children’s Hospital, as well as Melissa Ginn and Cindy Lin from Nationwide Children’s Hospital. We also acknowledge all the collaborators on the MIOS project and all families who participated in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KOY is supported by the National Institutes of Health, Eunice Kennedy Shriver National Institute of Child Health and Human Development (Predicting Outcomes in Children with Mild Traumatic Brain Injury; R01HD076885) and the Ronald and Irene Ward Chair in Pediatric Brain Injury; ALW is supported by the Harley N. Hotchkiss-Samuel Weiss and Killam Postdoctoral Fellowship; MGM is supported by a Mitacs Research Training Award.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.