
Abstract
Background
Headache is one of the most common and persistent symptoms following traumatic brain injury (TBI). The current study examines the prevalence and characteristics of headache following mild TBI (mTBI).
Methods
We prospectively enrolled 212 subjects within one week of mTBI who were hospitalized for observation or other system injuries in a single level 1 US trauma center and followed by telephone at three, six, and 12 months after injury for evaluation of headache. Headaches were classified according to ICHD-2 criteria as migraine, probable migraine, tension-type, cervicogenic, or unclassifiable headache.
Results
Subjects were 76% male and 75% white, and 58% were injured in vehicle-related crashes. A follow-up rate of 90% (190/212) occurred at 12 months post-injury. Eighteen percent (38/212) of subjects reported having a problem with headaches pre-injury while 54% (114/210) of subjects reported new or worse headaches compared to pre-injury immediately after injury, 62% (126/203) at three months, 69% (139/201) at six months, and 58% (109/189) at one year. Cumulative incidence was 91% (172/189) over one year. Up to 49% of headaches met criteria for migraine and probable migraine, followed by tension-type headaches (up to 40%). Age (≤ 60) was found to be a risk factor, but no significant difference was found in persistence of new or worse headache compared to pre-injury between males and females. More than one-third of the subjects reported persistent headache across all three follow-up time periods.
Conclusions
Headache after mTBI is very common and persistent across the first year after injury. Assertive, early treatment may be warranted to avoid chronicity and disability. Further research is needed to determine whether post-traumatic headache (PTH) responds to headache treatment used in the primary headache disorders and whether chronic PTH is preventable.
Keywords
Introduction
Approximately 1.7 million traumatic brain injuries (TBI) occur each year in the United States (US), 75% of which are classified as mild TBI (mTBI) (1). Headache is one of the most common and persistent symptoms following TBI (2,3), yet few prospective studies have examined the prevalence or characterized the headaches using descriptive features similar to those used in the characterization of primary headache disorders.
Post-traumatic headache (PTH) as currently defined by the International Classification of Headache Disorders, second edition (ICHD-2) (4), is a secondary headache disorder that must start within seven days of injury or after regaining consciousness following TBI. An acute PTH becomes chronic if headaches persist beyond three months after injury. No defining clinical characteristics of PTH are included in the definition.
Within the literature, the estimated prevalence of PTH has ranged from 30% to 90%,with most studies being retrospective assessments of headache. In a review of prior research, Lew et al. (5) reported that 18%–22% of PTHs lasted longer than one year across TBI severity. In those with mTBI, Dikmen et al. (3) found that 25%–29% of subjects endorsed new or worse headache compared to pre-injury at one year after injury, and Faux and Sheedy (6) showed that while all subjects had headache at time of injury, only 30% did at one month and only 15% at three months. However, other researchers have noted generally high frequencies of headache across the first year after primarily mTBI from 79% at three months after injury to 65% at one year (7–9).
Beyond research conducted with civilian samples, research on active duty military and veteran populations also suggests varied prevalence of headache after TBI from 24% (10) to more than 78% (11) depending on the severity of the TBI and the setting. More recent studies of soldiers returning from combat suggest higher rates of headache, but vary in length of time since injury. For example, Theeler et al. (12) reported that 78% of soldiers returning from combat with deployment-related concussion endorsed episodic headache and 20% met criteria for chronic daily headache.
In addition to the wide variation of prevalence, prior studies have also reported that prevalence in civilian TBIs is higher following mTBI than moderate to severe TBI (13–16). However, it is difficult to determine whether such a finding is due to actual differences in severity of TBI or is related to subject selection bias (e.g. selection from representative samples vs those seen in headache clinics). The goal of the present study was to prospectively study headaches in a representative sample of cases with mTBI. We sought to describe the incidence and prevalence of headache over the first year following mTBI, characterize the headache using primary headache disorder criteria, and examine potential risk factors for the development of PTH.
Methods
Study participants
Two hundred and twelve participants with mTBI were enrolled within one week of injury. Recruitment of consecutive admissions fulfilling eligibility criteria occurred at Harborview Medical Center, a level 1 trauma center in Seattle, Washington, between January 2010 and April 2011. Study research assistants (RAs) identified subjects by review of electronic medical records for daily admissions by screening for mechanism of injury or admission diagnosis codes related to head injury or concussion. RAs approached subjects and confirmed diagnosis of mTBI by interview and review of medical records. All data were entered into a database kept on a secure server with data checks incorporated to prevent erroneous data entry. Subjects provided consent during hospitalization and initial data were collected within one week of injury, usually while hospitalized for observation or other body system injuries. Follow-up assessments were completed by telephone at three, six and 12 months after injury by trained RAs. A minimum of five attempts were made to contact subjects by phone at different times of the day and different days (including evenings and weekends) to maximize follow-up.
Inclusion criteria were age ≥ 18 years, an acute mTBI during the current admission based on Centers for Disease Control (CDC) criteria (Glasgow Coma Scale 13–15 on emergency department evaluation, any period of loss of consciousness not exceeding 30 minutes, any period of alteration of consciousness or post-traumatic amnesia that did not exceed 24 hours), ability to give consent, speak English and have access to a telephone. Exclusion criteria were prior or current diagnosis of other central nervous system or major psychiatric disorders, intoxication on admission sufficient enough to cloud the diagnosis of mTBI, and current alcohol dependence. Subjects were also excluded if they were homeless or incarcerated, which would preclude follow-up. Informed consent was obtained as approved by the University of Washington Institutional Review Board. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (17).
See Figure 1 for details on the number of individuals screened and followed throughout the study. Individuals who were followed at 12 months (N = 190) post-injury were significantly older than those who were lost to follow-up (N = 22) (p < .05). No other differences were found between those who were and were not followed at 12 months (see Table 1).
Subject enrollment and follow-up throughout the study. Demographics and headache prevalence. Am.: American; TBI: traumatic brain injury; GCS: Glasgow Coma Scale.

Measures
Basic demographic data were collected from participants during hospitalization, including age at injury, sex, race (white, black, Asian/Pacific Islander, American Indian, Hispanic, and other), education (completed high school or more/did not complete high school), and cause of injury (vehicle, fall, violence, sports, hit by an object or other).
A headache survey, used successfully in a previous study of post-traumatic headache (18,19), included questions about current headache (yes/no), history of a problem with headache pre-injury, and characteristics of the current headache assessed within seven days of injury. Follow-up telephone interviews assessed for ongoing headache and characteristics of those headaches (See Appendix for full questionnaire).
We defined PTH and classified headaches using the same criteria as in our prior study on those with moderate to severe TBI (18,19). Briefly, we did not follow ICHD-2 (4) PTH criteria of headache within seven days of injury or regaining consciousness, but defined PTH as any headache occurring after injury. Subjects were asked whether they had a problem with headache prior to injury (yes/no) and whether they had a current headache that was new or worse than their pre-injury headache at baseline (within one week of injury). On subsequent evaluations at three, six, and 12 months, subjects were asked whether they had new or worse headache (compared to pre-injury headache only) in the preceding three months. At all follow-ups, subjects were asked about frequency of headache (categories included less than once per month, once a week to once a month, several times a week to daily, and no headache in the past three months) and, if they had headaches pre-injury, whether the headache they experienced was the same, better, or worse than their pre-injury headache. Only headaches that occurred after injury or were worse than pre-injury are included in the paper. Persistent headache was defined based on report of headache at all three follow-up timepoints (three, six, and 12 months), headaches at some timepoints, and finally, no headaches at any follow-up timepoint. Only participants who had data at all three timepoints were included.
Prevalence of headache was calculated for new or worse headache (compared always to their pre-injury state) at each assessment point divided by the total number of responders at each assessment. Incidence and cumulative incidence were calculated using subjects available at each assessment point, beginning with baseline assessment, with incidence assessing the new cases that occurred at each follow-up relative to the number who had not reported a new or worse headache (compared to pre-injury) at prior evaluations, and cumulative incidence being a sum of all participants who ever endorsed new or worse headache compared to pre-injury over time.
Decisions for classification of headache were based on answers to the headache questionnaire developed to follow ICHD-2 criteria for the primary headache disorders (see Appendix for questionnaire). The method used for categorization was the same as found in Lucas et al. (19). To review, headaches were classified into one of five categories: 1) migraine, 2) probable migraine, 3) tension-type headache and 4) cervicogenic headache (a symptom-defined secondary headache), and 5) if the headaches did not fit into one of the first four categories at a given timepoint, they were called unclassifiable. Migraine headache was defined based on a pain rating of moderate to severe with a pain intensity of greater than or equal to 4 on a scale of 0 “no pain” to 10 “worst pain possible” and two or more of the following: 1) self-report of the headache having a significant disabling impact; 2) headache was unilateral; 3) throbbing/pulsating; and/or 4) worsened by movement or physical activity. In addition, to be considered a migraine the participant had to endorse either nausea and/or vomiting or sensitivity to light and sound. Probable migraine was classified if the participant endorsed moderate to severe pain, but met one of the other criteria for migraine. Tension-type was classified if it was bilateral, vise-like, squeezing or tight and the pain was rated as mild to moderate. Cervicogenic was classified if it was unilateral, neck pain was endorsed, and the headache did not meet criteria for migraine, probable migraine or tension-type headache. All headaches that did not fit into the four classifications were considered unclassifiable. Classification of headache within the week after injury was not possible as we did not collect information on headache disability with the baseline questionnaire.
The classification was ordered such that precedence was given to migraine headache with or without aura at a given time point if criteria were met. Only if criteria were not met for migraine would a headache be classified as probable migraine, followed by tension-type, or cervicogenic to be the primary headache for a participant.
Statistical analysis
Descriptive statistics, including means (SD), percentages, and counts, are used to describe the natural history of headache in our subjects. Fisher’s exact analyses were used to compare persistence of headache over time between males and females and by age.
Results
Prevalence, incidence, and persistence of new or worse headache compared to pre-injury over time.

This sensitivity analysis is a calculated value assuming that those subjects lost to follow-up were followed and were headache free.
New or worse headaches compared to pre-injury were also found to be persistent in those (N = 184) who responded at all three follow-up time periods, with 41% of subjects reporting headaches across all three follow-up timepoints. Only 15% reported having no headache at three, six, or 12 months post-injury (Table 2).
Incidence and cumulative incidence
Table 2 and Figure 2 present incidence and cumulative incidence of headache for those followed as well as a calculated value from all 212 subjects, assuming those who were not followed were headache free. In the first year after injury the cumulative incidence of new or worse headache compared to pre-injury was 91% (89% in a sensitivity analysis of all N = 212 assuming those not assessed had no headache). The highest incidence occurred during the three-month follow-up period, when 59% of those subjects who had not reported headache at baseline reported having new or worse headache compared to pre-injury. An additional 44% of those who had not had headache at baseline or three months reported developing a new or worse headache compared to pre-injury for the first time at six months, and finally 15% reported new or worse headache compared to pre-injury for the first time at 12 months post-injury.
Incidence and cumulative incidence of headache.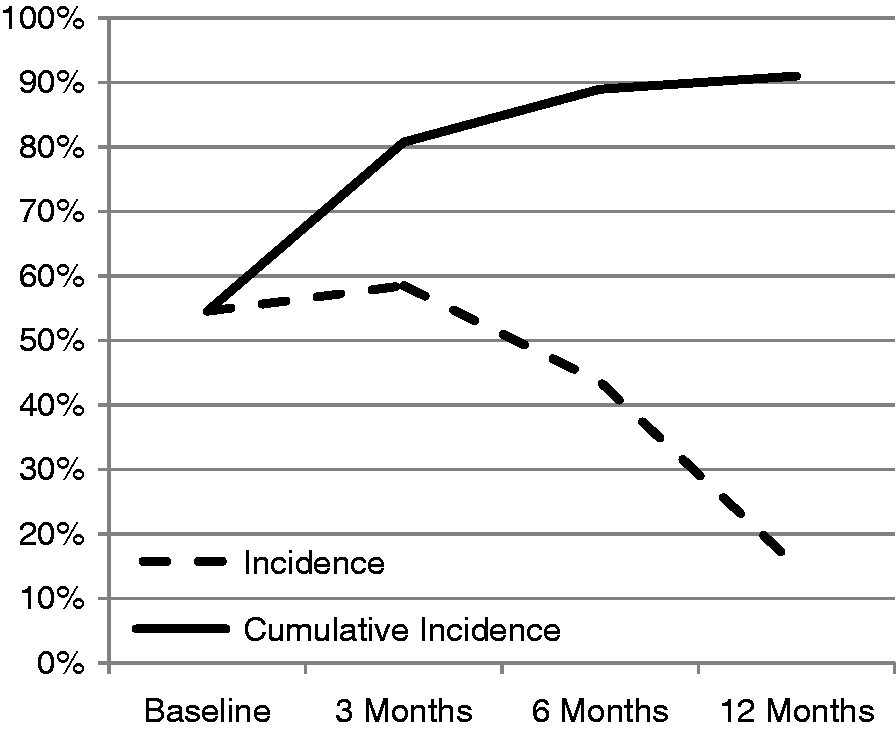
Headache characterization
Distribution of headache characterization at each timepoint.
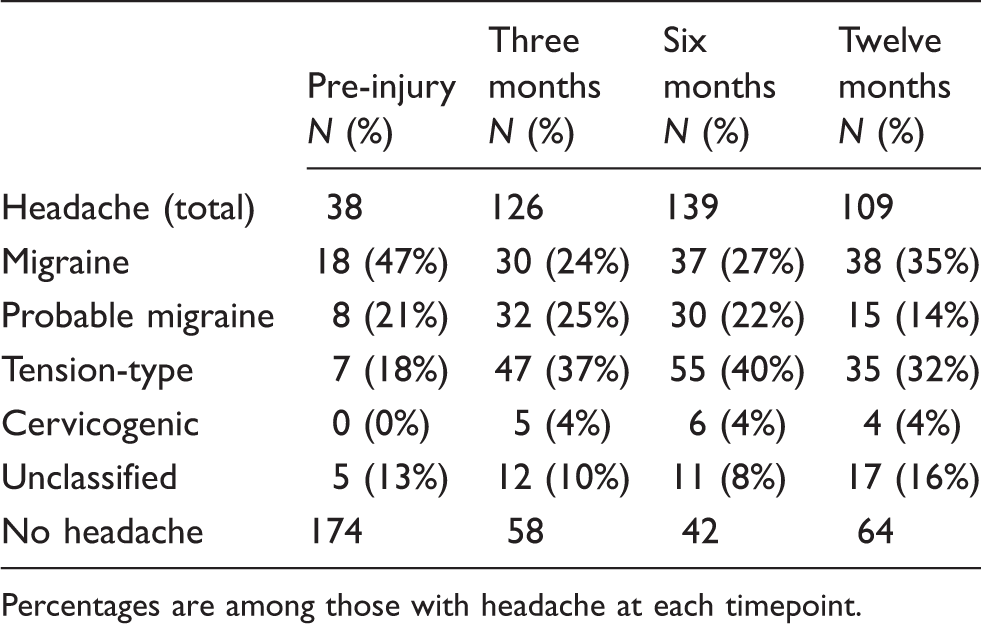
Percentages are among those with headache at each timepoint.
Table 3 also shows the characterization for those who endorsed pre-injury headache. Migraine and probable migraine were the most common type of pre-injury headache in this group and few headaches were unclassifiable.
Frequency of headache
Up to 27% of subjects reported having headaches several times per week to daily (Table 4). However, the most common headache frequency described was from one per week to one per month. For those who had the highest headache frequency of several per week to daily, 62% of the headache types were migraine in this highest frequency group at one year (see Figure 3 for 12 months after injury data). Infrequent headache (less than one/month) was most likely to be tension-type headache (59%). The pattern of findings was similar across all follow-up time periods (not shown).
Frequency of headache by characterization at 12 months. Frequency of headache over time.

Potential risk factors in development of PTH
There was no difference in the persistence of headache between males and females (p = .61). However, individuals over age 60 were significantly more likely to report no headaches over time and significantly less likely to have headaches at all timepoints (p < .001, see Figure 4).
Risk factors: sex and age.
Discussion
We found that the prevalence of new or worse headache compared to pre-injury headache after mTBI was 54% or greater at all timepoints over the first year following mTBI. This finding suggests that PTH is not only common but persistent. These high rates of PTH are similar to other studies that have also noted high rates of headache across the first year after mTBI (7–9). It is not clear why rates are so much higher in these studies than those reporting lower rates (3,5,6), but may be because of how the questions about headache were asked, the population studied, or the time frame that was covered. For example, we asked about headache over the prior three-month period, while others may have focused on headache only at the time of assessment. Indeed, in the Dikmen et al. (3) study, the subjects were asked whether they had new or worse headache compared to pre-injury over the preceding couple of weeks.
In our study, headaches following mTBI appeared to occur early after injury, within the first three months, and were likely to persist up to at least 12 months following injury. We found that 36% of participants reported headache at every follow-up timepoint queried. Given that 1.4 million mTBI injuries occur each year in the US, the burden of PTH is high. This is far longer than previously suggested in some prospective civilian populations (3,9). However, some studies did not follow patients for longer than three months post-injury (6,20). In still others, the potential problem of pre-existing headache and whether the PTH is new or worse clouds the prevalence interpretation.
Based on the civilian data reported in this study, early headache after TBI identifies people at high risk of developing frequent, chronic headache who may benefit from headache identification, assessment, and management. Further studies are needed to know whether aggressive, early management could prevent acute PTH from becoming chronic. We found that the majority of new or worse headaches after injury occurred within the first three months after mTBI, adding additional support for a change in the ICHD-2 criteria for PTH (18,21). These studies would suggest that the criterion for latency for PTH to occur after injury be changed from seven days to a longer time period. Further studies are needed to determine an optimal timepoint to identify the temporal relationship of a headache to the head trauma. In addition, a limiting timepoint should be viewed as a guideline for diagnostic and treatment purposes as clinical judgment is also necessary to define the relationship.
In our study, an additional 59% of subjects reported new or worse headache (compared to pre-injury) at three months who had not previously reported headache within the first seven days after injury (baseline assessment). Prior studies in moderate to severe TBI found 23% additional headaches occurred at the three-month assessment (18), and Theeler et al. found that 19% of a large cohort of US Army soldiers had onset of headache between one week and one month after concussion (11). A longer interval could minimize under-diagnosis of PTH and have a positive impact on treatment decisions and medico-legal issues in ongoing management of TBI. Although lengthening the latency included in the criteria for PTH might affect the homogeneity of research populations, it may more accurately reflect the clinical nature of these headaches.
The most frequent headache phenotypes found in this study of new or worse headache compared to pre-injury after mTBI were migraine and probable migraine. These two types of headache were found in 49% of individuals with headache at three, six, and 12 months after injury. In addition, those subjects with migraine reported higher headache frequency, suggesting that headache chronicity and potential disablement are a concern for those with headache following mTBI. In contrast, only 4%–5% of the general population report chronic daily headache (> 15 days per month, > 4 hours per day) (22–24), spotlighting a significant effect of mTBI on headache development and persistence. These results should encourage more consistent monitoring of headaches and response to treatment recommendations after mTBI, as persistent pain may complicate recovery from cognitive or behavioral issues that accompany mTBI (25).
In this study of headache following mTBI, females were not more likely than males to have new or worse headaches after injury compared to pre-injury, at odds with a gender difference found in the general headache population (26) and in other studies of more severe TBI (18). Interestingly, we also found that older age (> 60) was related to a lower prevalence of PTH, which was also reported by Dikmen et al. (3) in a population that included all levels of TBI severity.
The current study was based on a large prospectively enrolled, representative sample of subjects with mTBI presenting to a hospital for injury evaluation, and may reflect a more accurate estimate of prevalence of PTH compared to selected subject samples that present to specialty clinics. However, this study has several limitations. First, information on headache was all collected via self-report and no physician examination was completed. However, all information was collected by trained examiners using a standardized questionnaire with in-person initial assessment and by telephone follow-up at three, six, and 12 months after injury. The headache questionnaire itself was designed to collect data similar to a structured headache interview conducted by a provider in a headache specialty clinic. The use of electronic headache diaries in future studies may improve our ability to obtain more detailed information on headache closer to headache onset, and an evaluation by a physician may also assist in more specific classification in future studies.
As this was a study of subjects with mTBI, it is important that cognitive difficulties secondary to the injury not affect a subject’s ability to accurately report on health data. However, the literature suggests that cognitive impairments following mTBI are no longer detectable as compared to those with no mTBI by three months after injury (27). It may be that the population of those with mTBI admitted to the hospital differs from those not admitted or not evaluated in emergency departments and generalizability could be limited. Another limitation of our study was the report of only one headache type at each time period. Though we were able to assess whether subjects experienced more than one type of headache, we asked them to rate only their most severe headache and categorized the headache based on whether symptoms met classification criteria for the most severe type (migraine) at each time period. We did not assess whether more than one headache type could be classified at each time period as we prioritized the most severe headache that would be most clinically relevant to a treating practitioner.
Our data show that the majority of headaches experienced following mTBI may be classified using symptom-based primary headache criteria. Migraine and probable migraine described the majority of headaches at all timepoints up to one year after injury. For those who had frequent headache (several times per week to daily), the most common phenotype was migraine, suggesting that the majority of PTH is moderate to severe in intensity and frequent in a mild head injury population. This is even more striking given that our population was predominantly male and older than expected when compared to age- and sex-specific incidence rates of migraine in a general population(28).
Clinical trials are necessary to determine the inciting mechanisms and the most effective treatments for PTH. With many studies now supporting the use of primary headache disorder phenotyping for PTH, clinically meaningful headache characteristics may have relevance not only for development of a new, useful, and informative classification scheme for PTH, but also provide us with a framework on which to include common subject populations for future clinical trials and for management of this common, frequent, and persistent disorder following TBI.
Clinical implications
Headache after mild traumatic brain injury (mTBI) is very common and persistent across the first year after injury. Assertive, early treatment may be warranted to avoid chronicity and disability. Given the high frequency of migraine and probable migraine in this population, monitoring of headaches as well as response to treatment recommendations after mild TBI is warranted, since persistent pain may complicate recovery from cognitive or behavioral issues that may accompany mTBI. Further research is needed to determine whether post-traumatic headache (PTH) responds to headache treatment used in the primary headache disorders and whether chronic PTH is preventable.
Footnotes
Funding
This study was funded by the Department of Education, National Institute on Disability and Rehabilitation Research, grant number H133G090022.
Conflicts of interest
Dr Lucas receives funding from the National Institute on Disability and Rehabilitation Research (NIDRR), Department of Defense, the Wadsworth Foundation, St. Jude Medical Inc and Biogen Idec. She has received consulting fees or honoraria from Zogenix, MAP, Allergan, Biogen Idec, Genzyme, and Novartis.
Dr Hoffman and Dr Bell receive research funding from NIDRR and Department of Defense.
Dr Dikmen receives research funding from NIDRR, Department of Defense and National Institutes of Health (NIH).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.