
Abstract
Background: To examine the prevalence and characteristics of acute posttraumatic headache (APTH) attributed to mild head injury within a prospective, observational study design.
Methods: We recruited 100 patients with acute mild head injury as defined in the International Classification of Headache Disorders, 2nd Edition (ICHD-2) presenting to the department of trauma surgery at the Medical University of Vienna. Patients underwent a detailed telephone interview between days 7 and 10 and between days 90 and 100 after the injury.
Results: The prevalence of APTH was 66%. APTH had occurred within 24 hours after the trauma in 78% and lasted for a median of 3.0 days. Headache was unilateral in 45%. Aggravation by physical activity, nausea and photo-/phonophobia was present in 49%, 42% and 55%, respectively. The prevalence of APTH was related to conditions of chronic pain (excluding headache), pre-existing episodic headache, number of posttraumatic symptoms, anxiety and depression. At follow-up at 90–100 days, posttraumatic headache had abated in all patients.
Conclusions: APTH attributed to mild head injury is a common but self-limiting condition frequently showing migrainous features. Participants with chronic pain other than headache, pre-existing headache and affective disorders are at higher risk of developing APTH. None of the patients developed chronic posttraumatic headache.
Introduction
The yearly incidence of head trauma is 350 per 100,000 in Europe (1). Mild head trauma accounts for the majority of cases (2,3). The symptoms following mild head injury are summarized as posttraumatic syndrome and can be differentiated into three groups: physical (e.g. double vision, blurred vision, headache, nausea, sensitivity to light and noise, sleep disturbance), emotional (e.g. being irritable, feeling frustrated, depressed or restless) and cognitive (e.g. forgetfulness, poor concentration, taking longer to think) (4,5).
Headache is the most frequent symptom of posttraumatic syndrome. Acute posttraumatic headache (APTH) is defined as headache developing within 7 days after head trauma in the International Classification of Headache Disorders, 2nd Edition (ICHD-2) (6). According to previous studies it occurs in nearly half of patients and usually resolves within a few weeks (7,8). Headache persisting for more than 3 months after the trauma, that is, chronic posttraumatic headache (CPTH) according to ICHD-2 (6), was reported in 15–50% of patients (1,7,9,10).
However, scientific evidence regarding the characteristics of posttraumatic headache is poor. APTH has been almost completely neglected. CPTH has drawn at least some attention, partly because its existence has been doubted as its development was found to be related to prospect of financial compensation and wish of retirement (11). The characteristics of APTH vary widely between different surveys (1). This is also reflected in ICHD-2 by defining APTH as ‘headache, no typical characteristics known’ (6). In a study by Haas in the 1990s including 48 patients with CPTH (12), the headache of 75% of patients resembled chronic TTH, 21% resembled migraine without aura and 4% were unclassifiable. To our knowledge there is only one survey applying ICHD-2 criteria (6) and analyzing CPTH with respect to its fulfilment of the criteria of primary headache disorders (13). Among 53 patients, CPTH resembled chronic TTH in 51%, episodic TTH in 11%, migraine without aura in 2%; 8% had coexisting chronic TTH and migraine without aura and 19% chronic TTH with probable migraine without aura. In the remaining 9% of the patients CPTH was unclassifiable. In a few cases, trigeminal-autonomic headaches (cluster headache, paroxysmal hemicrania and short-lasting unilateral neuralgiform headache with cranial autonomic symptoms (SUNA)) and hemicrania continua have been reported as posttraumatic (14–17).
Among patients with acute posttraumatic syndrome, those with headache perform worse in neuropsychological functioning than those without and they report more posttraumatic symptoms (18). This finding led to the hypothesis that headache is probably associated with an incomplete recovery. In another survey, including patients with CPTH, self-reported greater impairment was related to worse performance in neuropsychological testing (4). Within the same study, depressed participants reported more severe cognitive and emotional symptoms than non-depressed participants. A link between post-concussional symptoms and depression was also found in several other studies (19–22).
In summary, APTH can be assumed a frequent disorder, but it has not attracted much scientific attention. We therefore aimed to prospectively characterize APTH in terms of prevalence and clinical features in the context of posttraumatic syndrome, and assess the impact of anxiety and depression in patients with mild head injury. Furthermore, we wanted to assess the percentage of patients with APTH evolving to CPTH.
Methods
Diagnostic criteria of acute post-traumatic headache attributed to mild head injury according to ICHD-2

In total, we reviewed the charts of 2571 consecutive patients. According to the charts, 1781 did not fulfil inclusion/exclusion criteria, with age being the leading cause (n = 1359). We called 790 patients, of whom 488 reported exclusion criteria not mentioned in the charts (e.g. previous head trauma or alcohol abuse). Among the remaining 302 patients, 137 could not be reached at three attempts and 65 refused to participate. Accordingly, 100 patients completed the questionnaire.
Eligible patients were called 7–10 days after trauma and, after obtaining oral informed consent, underwent a detailed telephone interview about general demographic features, medical history (with an emphasis on pre-existing headaches), conditions of chronic pain other than headache (defined as pain persisting for at least 3 months) besides headache, trauma history and – if applicable – characteristics of posttraumatic headache. We used an identical set of questions for assessing pre-existing and posttraumatic headaches. Questions about headaches included all items necessary for classification of migraine and TTH according to ICHD-2 (6). We further asked for presence and absence of 14 post-concussional symptoms (including headache) following the Rivermead Post Concussion Symptoms Questionnaire (23). In addition, we performed the Self-rating Depression Scale (SDS) and the Self-rating Anxiety Scale (SAS) by Zung (24,25). The same set of questionnaires was performed at the second call between days 90 and 100 after the trauma.
The Rivermead Post Concussion Symptoms Questionnaire asks for presence and severity of 14 posttraumatic symptoms (including headache), grading each item from 0 (not experienced at all) to 4 (a severe problem) (23). For reasons of practicability during the telephone interview, we asked only for presence (1 point) or absence (0 points) of symptoms, excluding headache, giving a score from 0 to 13.
SDS is a 20-item self-report measure of the symptoms of depression. Participants rate each item according to how they felt during the preceding 7 days. Item responses are ranked from 1 to 4. The sum of the 20 items produces a score ranging between 20 and 80; a value of ≥ 40 suggests clinically relevant depression (24).
SAS measures affective and somatic symptoms of an anxiety disorder. The structure of the SAS is similar to that of the SDS. It also consists of 20 questions, which refer to the past seven days. The result of the SAS is obtained by summing the scores. A value of ≥ 40 suggests the presence of a clinically relevant anxiety disorder (25).
SDS and SAS were chosen as questionnaires because they allow a quick and valid screening for the corresponding affective disorders. Answers are structured similarly to a 4-point Likert scale in which patients should indicate how much each statement applies to them (‘a little of the time’, ‘some of the time’, ‘good part of the time’ and ‘most of the time’) – which allows simply reading the questions to the patient without repeating the answers to each of the questions, thereby saving time. Previous studies also evaluated depression and anxiety via telephone interviews (26,27).
The term APTH will be used throughout the paper for all headaches experienced by the patients after the trauma, regardless of whether they had pre-existing headache or not. The issue will be further discussed later.
Characteristics of headache were described as frequencies or mean values ± standard deviation (SD), as applicable. Multivariate logistic regression analysis was used for comparing patients with and without APTH. For calculating correlations Spearman’s correlation coefficients were used. Alpha level of significance was set at 5%. All analyses were carried out using SPSS 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Baseline characteristics of 100 consecutive patients with mild head trauma
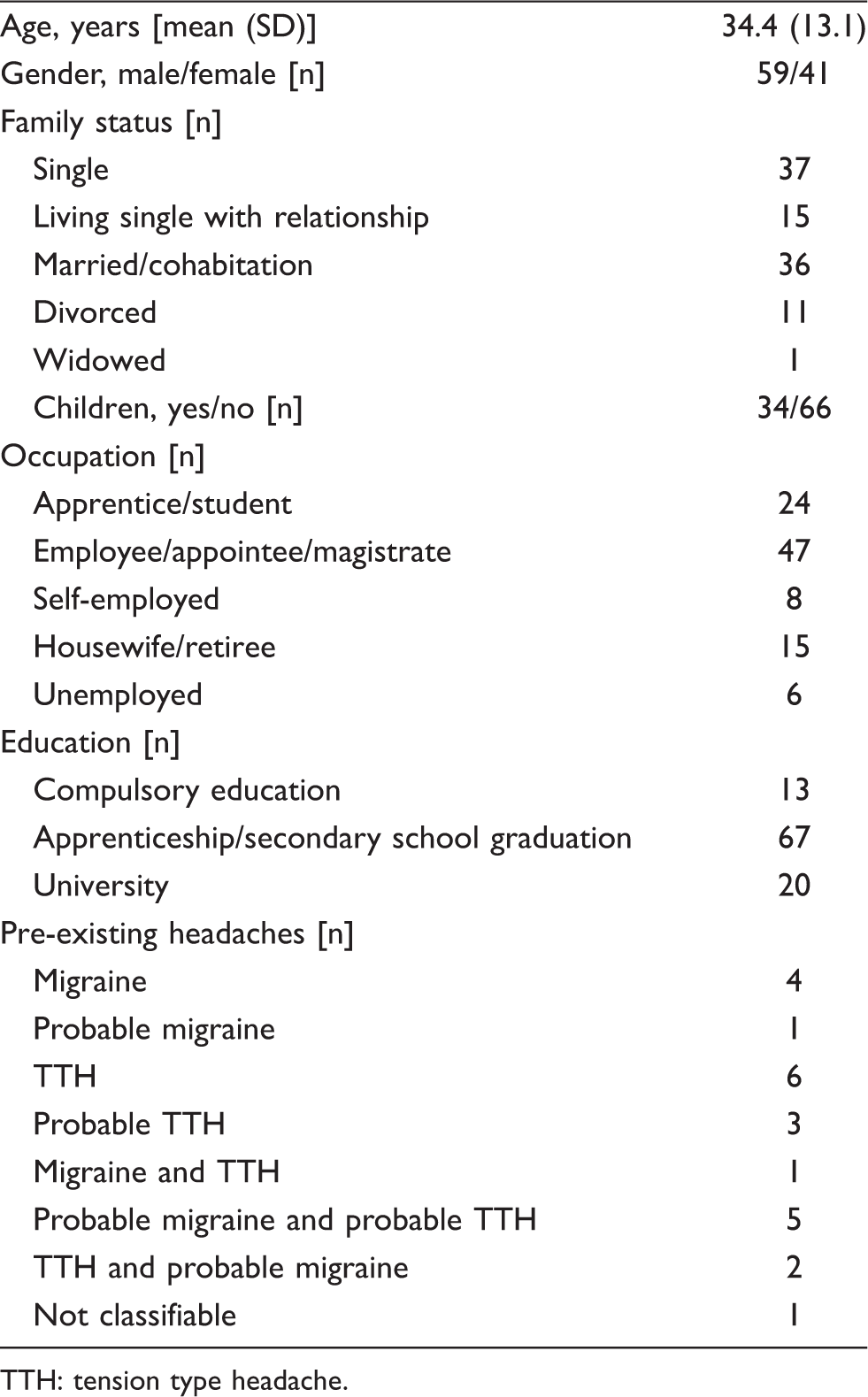
TTH: tension type headache.
Causes of the trauma were falls in 45 patients, assault in 25, traffic accidents in 13 and other in 17. Thirty-six patients lost consciousness for less than 30 minutes and 27 had amnesia. Twenty-six had consumed alcohol before the accident. Thirty-eight were admitted to hospital and 57% were on sick leave after the trauma (for a mean of 5.3 days, SD 3.0 days).
Headache after the trauma was experienced by 66 patients. Headache developed immediately after the injury or within 24 hours in the majority (79%) and occurred intermittently in almost half of the affected patients (48%). Headache was unilateral in 44%, mild in 41%, moderate in 39% and severe in 20%. The mean score on a verbal numeric rating scale (VNRS, no pain = 0, maximum pain = 10) was 4.2 ± 1.8. Quality was pressing in 69%, pulsating in 34% and stabbing in 42% of the patients. Aggravation by physical activity, nausea and/or vomiting and photo- and/or phonophobia were reported by 49%, 42% and 55%, respectively. For further details see Figure 1.
Clinical characteristics of posttraumatic headache in 66 patients with mild head injury. (Note: the duration of headache was not determined in two patients because of medication intake shortly after headache onset.).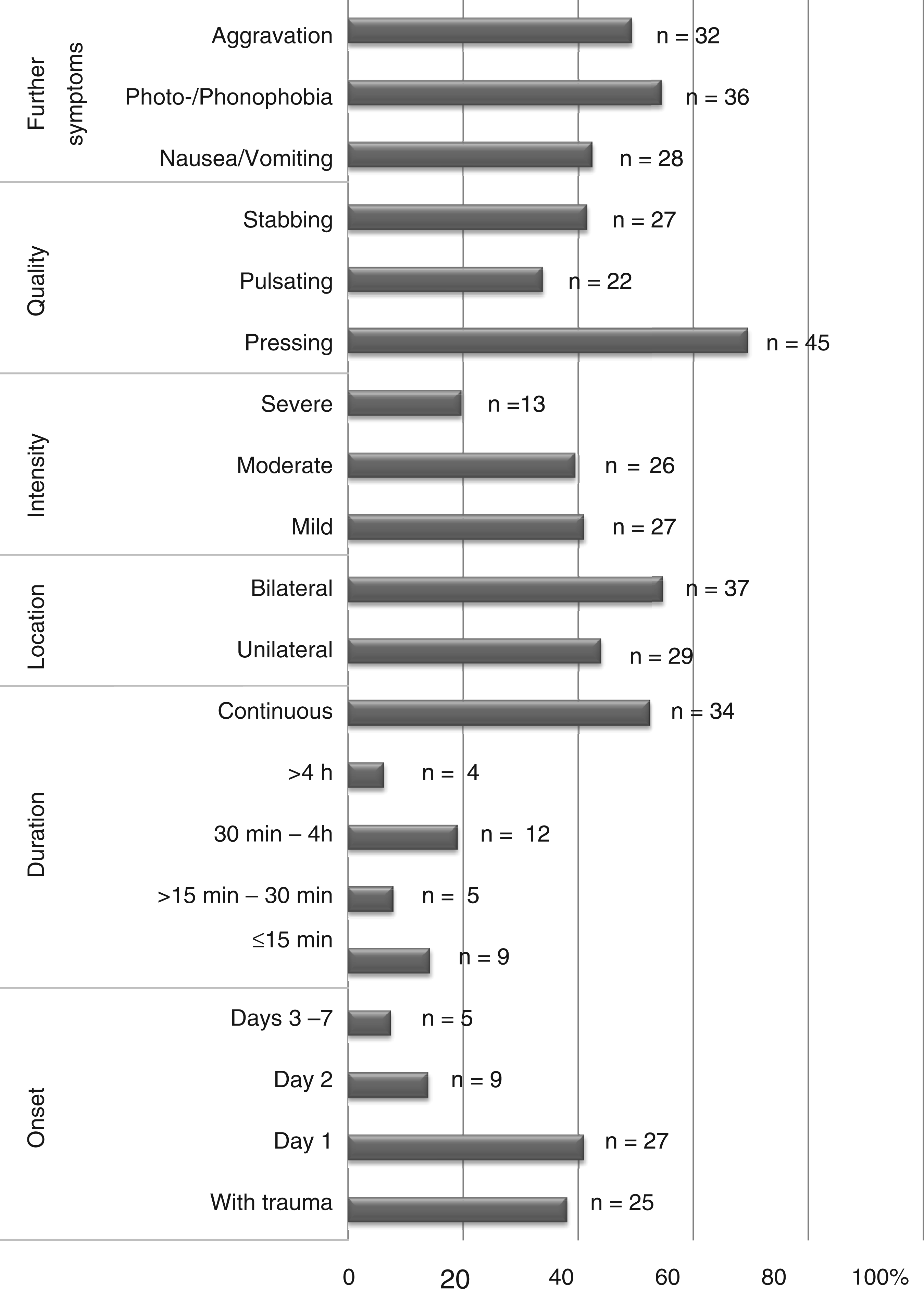
Classification of APTH by clinical appearance according to ICHD-2 criteria of migraine and tension-type headache (excluding criterion A)

Comparison of patients with (n = 66) and without (n = 34) APTH

n.s.: not significant, SDS: Self-rating depression scale, SAS: Self-rating anxiety scale.
At follow-up at least 90 days after trauma, 71 patients (71%) could be reached. APTH had been present in 41 patients and absent in 30. None of the patients who did not have APTH at the first interview had developed it at the second interview. In all patients initially reporting APTH, this headache had abated and therefore did not lead to a diagnosis of chronic posttraumatic headache. Among these patients were 11 who reported episodic headache before the trauma. They denied change of their pre-existing headache since the trauma. Headache lasted a median of 3.0 days, with a minimum of half a day and a maximum of 35 days.
Discussion
This is the first study prospectively assessing the characteristics of APTH as defined in ICHD-2 (6) in a strictly defined group of patients. In adults aged 18–65 diagnosed with mild head injury and without evidence of (concomitant) whiplash injury, substance abuse and chronic headache, two-thirds experienced headache following the trauma. APTH was usually self-limiting and frequently characterized by migrainous features. It was not related to demographic factors, such as age or gender, but was related to premorbid conditions: chronic pain, pre-existing headache, other symptoms experienced within the posttraumatic syndrome and affective disorders.
Ninety-two percent of all patients with APTH reported headache onset within the first 48 hours after trauma. Notably, APTH appeared intermittently in nearly half of the cases, and it was unilateral in 44% and moderate or severe in 59%. Together with the high number of symptoms that appeared in association with headache, this led to a diagnosis of migraine or probable migraine according to ICHD-2 (6) in 35% of the patients. We are aware that there is an overlap between APTH and post-concussional symptoms; however, these were distinguished within the questionnaire by asking patients to distinguish between symptoms that were generally present since trauma and symptoms that appeared only in association with headache.
In patients with pre-existing headache, the unanswered question is whether headache occurring after a mild head trauma is a new headache (APTH) or represents an aggravation or a change of the pre-existing headache. In our patients, one third claimed that the headache which occurred after the trauma resembled their usual, pre-existing headache. ICHD-2 criteria (6) leave the decision open to the judgment of the treating physician. When a pre-existing headache is made worse in close temporal relation to a trauma, the patient can either be given only the diagnosis of the pre-existing primary headache or the diagnosis of both the pre-existing primary headache and the headache attributed to the trauma. A marked worsening of pre-existing headache is mentioned as a supportive factor for the latter. This does not seem to apply for our patients, as there was no clear pattern of worsening in terms of more severe intensity or increased duration of posttraumatic headache.
Chronic pain conditions beside headache and pre-existing headache were more frequent in patients with APTH. A similar finding was described by Stovner and Obelieniene (28) for patients with whiplash-headache: previous headache as a major risk factor for the acute and chronic stage. This supports a hypothesis of Saper (29), who said that it may not be so much what happens to the head, but whose head it happens to. A brain that is already sensitized or dysfunctional because of a pre-existing headache disorder may react more easily with headache after a mild head trauma.
The finding that the number of posttraumatic symptoms was significantly higher in patients with APTH than in those without confirms a study by Collins and co-workers (18). Within a group of athletes with sports-related concussion, those reporting headache as a symptom reported significantly more other post-concussional symptoms than those without. In addition, they performed worse in neuropsychological testing one week after trauma. Accordingly, headache – as a somatic symptom – might indicate a more ‘severe’ form of ‘mild’ head injury.
We believe that Criterion A of the existing ICHD-2 criteria for APTH (6) cannot be specified more accurately. Within our population we found about one third of headaches resembling migraine or probable migraine, one third resembling TTH or probable TTH and one third that could not be classified according to ICHD-2. The great variability of head traumas and the participants’ individual physical and psychological reactions results in a great variety of headaches with no typical characteristics. Criterion B characterizes mild head trauma and was applicable to all eligible patients. Regarding criterion C, 92% of our patients developed headache within 48 hours after trauma. None of the patients reported a headache onset at seven or more days at the time of the second call. Hence, headache onset more than 48 hours after the trauma therefore seems to be rare. Another – although retrospective – survey described headache onset within a maximum of 3 days in 53 patients with CPTH (13). The time interval between head trauma and headache onset could thus be shortened in the criteria. Criterion D was applicable at the first call on day 7–10 and is not questioned by our study as in all patients headache remitted within 3 months.
Previous studies have suggested that affective disorders augment pain intensity (30,31) by enhancing attention to pain, and pain in turn generates anxiety and depression. This cascade, well known in chronic pain, could start within the first days after trauma. In addition, affective disorders such as depression and anxiety are well known comorbidities of primary headache disorders and they add up to disease-related disability (32,33). Our study suggests that they also have a role in APTH. Patients with APTH showed higher levels of anxious and depressive symptoms than patients without.
When discussing the relationships between APTH, post-concussional syndrome and affective disorders, one must point out that post-concussional syndrome is controversial as a disease entity. Symptoms required for diagnosing it according to ICD-10 (6) are frequently found in the general population (29). Furthermore, 90% of patients with depression were found to meet self-report criteria for a post-concussional syndrome and more than half of patients met conservative criteria for its diagnosis (21). Therefore it seems likely that patients with major depression suffering a mild head injury are misdiagnosed with post-concussional syndrome. Finally, it was shown that presence or absence of a head injury had no effect on self-reported post-concussional symptoms in patients with a known premorbid affective disturbance (34). Our study contributes another aspect to this issue. High levels of depression and anxiety in posttraumatic patients increase the risk of APTH, and they are associated with a larger number of posttraumatic symptoms. This may suggest that APTH goes along with affective disorders or at least with a depressive or anxious reaction to a trauma.
Although APTH as a headache entity is broadly accepted, its chronic counterpart causes much more controversy. Available literature varies between no difference in headache 3 months after trauma compared with controls (35,36) to an incidence of CPTH of 15–50% (7,9,10,37). So theoretically up to 33 patients with APTH within our patient population could have been expected to develop CPTH.
Comparing our patient population with other studies that found patients developing CPTH shows the following differences. In the survey by Faux and Sheedy (9) with 15% incidence of CPTH, all patients had headache at the beginning, which might, as noted above, point towards a more ‘severe’ form of ‘mild’ head injury and raise the probability of CPTH. Furthermore, Faux and Sheedy did not exclude patients with previous headache, nor did they give any information about it, which could also raise the probability of CPTH. Mickeviciene et al. (35) included patients with loss of consciousness, regardless of age, and excluded patients for similar reasons to ours, for example alcohol or drug abuse or previous concussion. Stovner et al. (36) included patients with loss of consciousness for less than 15 minutes, aged between 18 and 60 within the prospective part of their survey, without other obvious exclusion criteria. As both studies come to the same conclusion as ours regarding CPTH, selection of patients does not seem to have a major effect. Other studies were retrospective in design (7,37), therefore bearing the risk of recall bias, performed before establishment of ICHD-2 criteria (7,37) or included patients with moderate and severe head trauma (10,37).
The prospect of financial compensation has been claimed to be a reason for persistence of posttraumatic symptoms (11). Lack of litigation in the vast majority of our study population could be suspected to be a reason for lack of CPTH. At the time of our interview, 74% of patients already knew that there would be no litigation following the trauma, 17% were not sure and only 9% claimed that there would be litigation. The percentage of possible or definite litigation did not differ in patients with and without APTH. In Lithuania, a country where the expectation of financial compensation is low, there was no difference in headache prevalence after 3 months and 1 year in patients and controls (35,36). The present study therefore supports the concerns about the validity of CPTH as an disease entity.
Moreover, patients did not know that our interview served the purpose of assessing posttraumatic headache, as the study was presented to them as a general follow-up after a visit to the Department of Trauma Surgery. Comparable studies do not describe their method of presentation to eligible patients, but this might also make a difference.
Our study has several strengths and limitations. Strengths are strict inclusion/exclusion criteria, use of ICHD-2 criteria (6), prospective study design and the detailed assessment of pre-existing headaches allowing a clear characterization of acute posttraumatic headache. The strict inclusion/exclusion criteria are also the most important limitation considering that 2269 of the 2571 patients screened were not included, mostly because of age and alcohol abuse. Reasons for excluding these groups of patients were mostly avoidance of patients with repetitive falls and multimorbidity and therefore doubt about the origin of the headache. Sixty-five patients refused to participate in the study. It could be speculated that those with fewer symptoms had less interest in participating. As this study is hospital-based, selection bias cannot be excluded, but it is likely to be limited because the Austrian health care system allows free access to the ER. We aimed to avoid further selection within the patient population by presenting the study as a general follow-up of the visit to the emergency department, not stating our specific interest in headache. Although headache should not have influenced the decision to participate, having fewer other symptoms could have done so. Further limitations are the lack of headache diaries and face-to face interviews. The size of the study group appears too small to allow generalizability. This should rather be seen as first step towards better understanding of a fairly common headache entity.
In conclusion, APTH attributed to mild head injury is a common but self-limiting condition frequently showing migrainous features. Participants with chronic pain other than headache, pre-existing headache and affective disorders are at higher risk of developing APTH.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
C.W. has received honoraria and travel funding from Allergan, AstraZeneca (Austria), Hermes Arzneimittel GmbH, Linde Gas (Austria), A. Menarini Pharma GmbH (Austria) and Pfizer (Austria). The other authors declare that they have no conflict of interest.