
Abstract
Background
Multiple cranial nerve blocks of the greater and lesser occipital, supraorbital, supratrochlear and auriculotemporal nerves are widely used in the treatment of primary headaches. We present efficacy and safety data for these procedures.
Methods
In an uncontrolled open-label prospective study, 119 patients with chronic cluster headache, chronic migraine, short lasting unilateral neuralgiform attack disorders, new daily persistent headaches, hemicrania continua and chronic paroxysmal hemicrania were examined. All had failed to respond to greater occipital nerve blocks. Response was defined as a 50% reduction in either daily attack frequency or moderate-to-severe headache days after 2 weeks.
Results
The response rate of the whole cohort was 55.4%: Chronic cluster headache, 69.2%; chronic migraine, 49.0%; short lasting unilateral neuralgiform attack disorders, 56.3%; new daily persistent headache, 10.0%; hemicrania continua, 83.3%; and chronic paroxysmal hemicrania, 25.0%. Time to benefit was between 0.50 and 33.58 hours. Benefit was maintained for up to 4 weeks in over half of responders in all groups except chronic migraine and paroxysmal hemicrania. Only minor adverse events were recorded.
Conclusion
Multiple cranial nerve blocks may provide an efficacious, well tolerated and reproducible transitional treatment for chronic headache disorders when greater occipital nerve blocks have been unsuccessful.
Keywords
Introduction
Patients with primary headaches often complain of pain involving both the frontal (trigeminal innervation) and posterior (occipital nerves innervation) regions. This is due to the anatomical link between cervical and trigeminal afferents onto neurones within the trigeminocervical complex (TCC) (1). Peripheral nerve blocks targeting the occipital or trigeminal nerve branches of the scalp used in the treatment of headache are believed to exert effects via the TCC (2).
Peripheral nerve blocks provide prompt relief for patients with headache disorders. Their benefit has been shown to last beyond the period of local anaesthesia (3,4). The common target for peripheral nerve blocks is the greater occipital nerve (GON). However, other nerves innervating the scalp including the lesser occipital nerve (LON) and numerous branches of the trigeminal nerve such as the supratrochlear (STN), supraorbital (SON), and auriculotemporal (ATN) nerves can also be targeted.
The outcomes of greater occipital nerve blocks (GONB) have been widely produced in open-label studies in cluster headache (3,5–8), chronic migraine (CM) (3,9), hemicrania continua (HC) (3,10–12), short lasting unilateral neuralgiform headache attacks (3,13,14) and chronic paroxysmal hemicrania (CPH) (3,11). Controlled trials are few but have been performed in cluster headache (15,16) and migraine (17–20).
The use of blocks of multiple occipital and trigeminal nerve branches has not been well explored. We wished to explore the efficacy and safety of multiple cranial nerve blocks (MCNB) consisting of the GON, LON, SON, STN and ATN in patients with chronic headaches.
Methods
Standard protocol approvals, registrations, and patient consents
This study received ethics approval from the Northwick Park Hospital NHS Research Ethics Committee. All patients provided written consent.
Patients
Demographic details by headache phenotype.
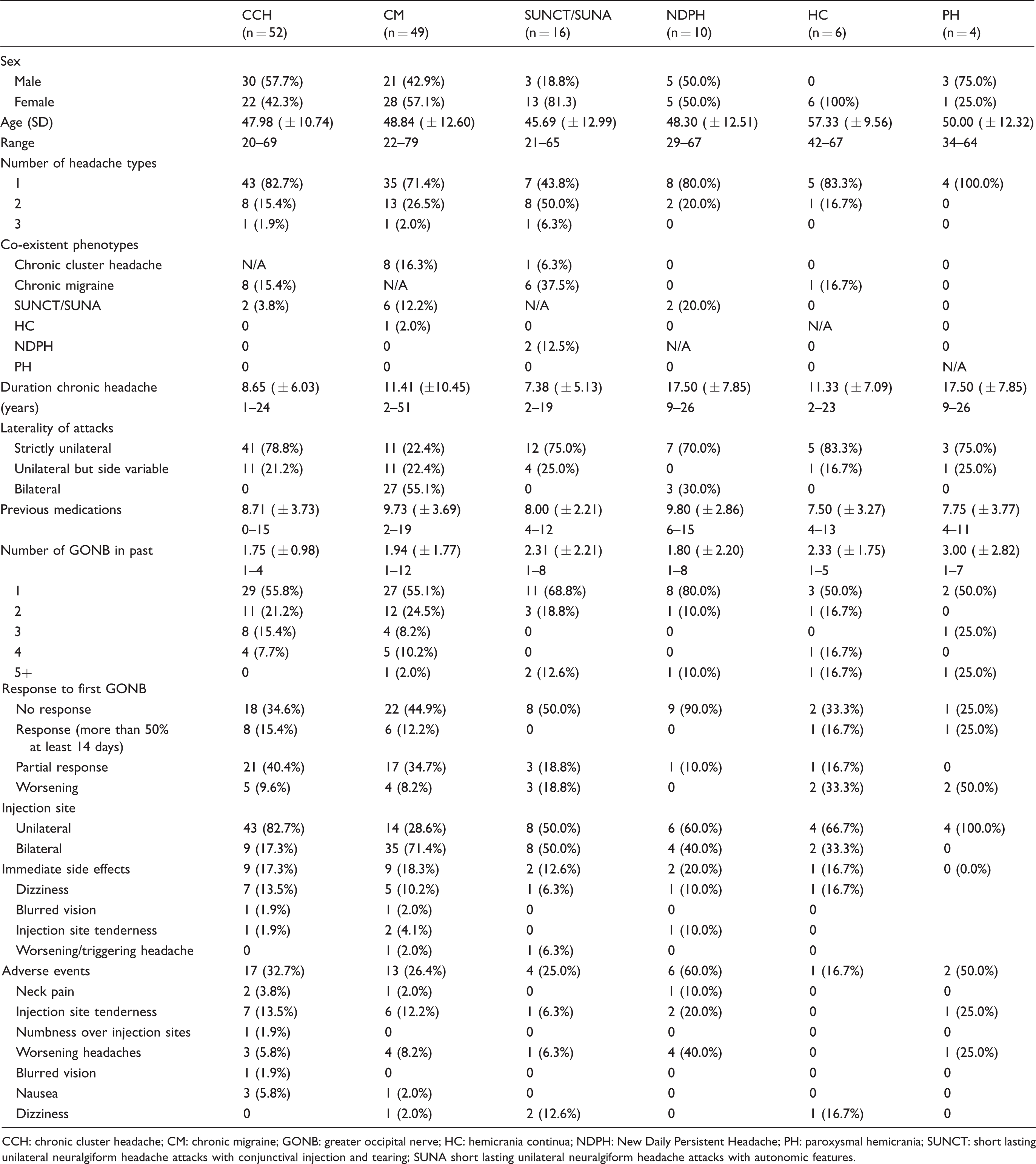
CCH: chronic cluster headache; CM: chronic migraine; GONB: greater occipital nerve; HC: hemicrania continua; NDPH: New Daily Persistent Headache; PH: paroxysmal hemicrania; SUNCT: short lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA short lasting unilateral neuralgiform headache attacks with autonomic features.
Multiple cranial nerve block procedure
Multiple cranial nerve block injection protocol.
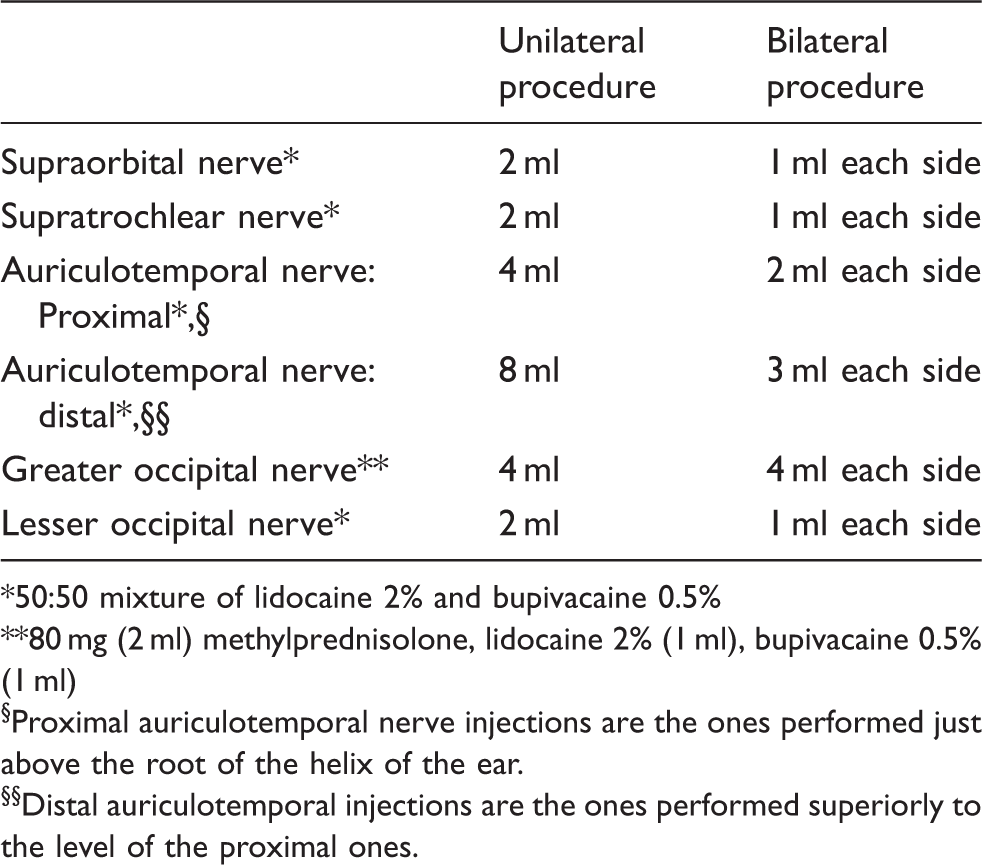
50:50 mixture of lidocaine 2% and bupivacaine 0.5%
80 mg (2 ml) methylprednisolone, lidocaine 2% (1 ml), bupivacaine 0.5% (1 ml)
Proximal auriculotemporal nerve injections are the ones performed just above the root of the helix of the ear.
Distal auriculotemporal injections are the ones performed superiorly to the level of the proximal ones.
Figure 1 illustrates the injection sites. Localisation of the nerves was as follows:
Greater occipital nerve: at a point lying on the medial third of a line drawn between the occipital protuberance and mastoid process; Lesser occipital nerve: At a point lying two-thirds of the way on the line drawn between the occipital protuberance and mastoid process; Supratrochlear nerve: At a point just above the superomedial aspect of the orbit; Supraorbital nerve: At a point just above the supraorbital notch (mid-pupillary line);
Sites of peripheral nerve blocks.

Auriculotemporal nerve: First injection at a point 1–1.5 cm above the root of the helix of the ear; second injection 1–1.5 cm in front of the first injection site; third injection 2–3 cm above the upper tip of the ear; fourth injection 2–3 cm anterior to the third; fifth injection 2–3 cm anterior to the fourth. If the procedure is unilateral, then a sixth injection is placed 2–3 cm above the fourth.
The procedure took approximately 10 minutes to complete. As this procedure was offered as part of a patient's routine clinical care, changes in preventative medication were allowed, as was use of acute medication.
The maximum safe dose for infiltration or subcutaneous injections of lidocaine is 4.5 mg/kg per dose. A 70 kg adult can therefore have lidocaine 315 mg infiltrated. In this study, we infiltrated a total lidocaine dose of 220–240 mg. The maximum safe dose for infiltration or subcutaneous injection of bupivacaine is 175 mg per dose. In this study, we infiltrated a total bupivacaine dose of 40–45 mg (22).
Data collection
Data was collected prospectively using headache diaries and entered onto a clinical database (Microsoft Excel, Microsoft Corporation, Redmond, WA, USA.). Patients kept prospective headache diaries for one month before and after MCNB. Where multiple phenotypes existed, patients were asked to keep separate diaries for each pain type. Average values of all headache measures were calculated for the 2 weeks prior to and after MCNB as well as weeks 3–4. Collected data included patient demographics, headache phenotype, headache days (any day on which pain was recorded (23)), moderate-to-severe headache days (days on which verbal rating scale of pain was four or more, lasting at least four hours (23)), daily attack frequency, average daily pain/attack severity, average daily pain/attack duration and adverse events.
Primary outcome measure was the number of patients responding to treatment. Response was defined as a 50% or more reduction in mean moderate-to-severe headache days (for CM, NDPH and HC) or attack frequency (for CCH, SUNCT/SUNA and CPH) over the first 2 weeks. Secondary outcomes included changes in headache days, pain/attack duration, daily pain/attack intensity, pain-free days over the first 2 weeks and the same measurements after weeks 3 and 4. Total duration of effect and total pain-free days were collated, as was information on repeated procedures. Information on these longer-term outcomes was obtained and recorded during routine follow-up clinics.
Statistics
Continuous variables are summarised using mean, standard deviation and range, while categorical variables are summarised with percentages. Mean values pre- and post-treatment were compared using paired t-tests. Statistical significance level was set at the 95% level (p = 0.05). Data was processed using IBM SPSS Statistics version 22 (IBM Corp. Int.)
Results
Demographics
A total of 119 patients receiving initial MCNB were analysed, with 137 headache phenotypes treated (17 patients documenting multiple phenotypes on separate diaries). The mean age of the whole group was 48.51 years ( ± 12.13) and 55 patients (46.2%) were male. Phenotypes included CCH (43.7%), CM (41.2%), short lasting unilateral neuralgiform attack disorders (13.4%), NDPH with migrainous features (8.4%), HC (5.0%) and CPH (3.4%). Patients were complex, and many had failed multiple medications prior to MCNB. The breakdowns of headache diagnosis and demographics are shown in Table 1.
Efficacy
The efficacy of response was determined on the basis of the average attack frequency (for cluster headache, short lasting unilateral neuralgiform attack disorders and paroxysmal hemicrania) or moderate-to-severe headache days over the first 2 weeks. Of the 137 headaches treated, 76 (55.4%) showed a positive response. The breakdown of response rates by phenotype is shown in Figure 2(a).
Response rates of MCNB by headache phenotypes. (a) Response rates after first MCNB by headache phenotype; (b) response rates of repeated MCNB by headache phenotype. The average number of MCNB per phenotype was as follows: CCH 2.44 blocks (range 1–8); CM 2.67 blocks (range 1–8); SUNCT/SUNA 3.56 blocks (range 1–8); NDPH 1 block; PH 1 block. The number of patients undergoing repeated blocks was as follows: CCH 27; CM 17; SUNCT/SUNA 9; NDPH 0; HC 4; PH 0.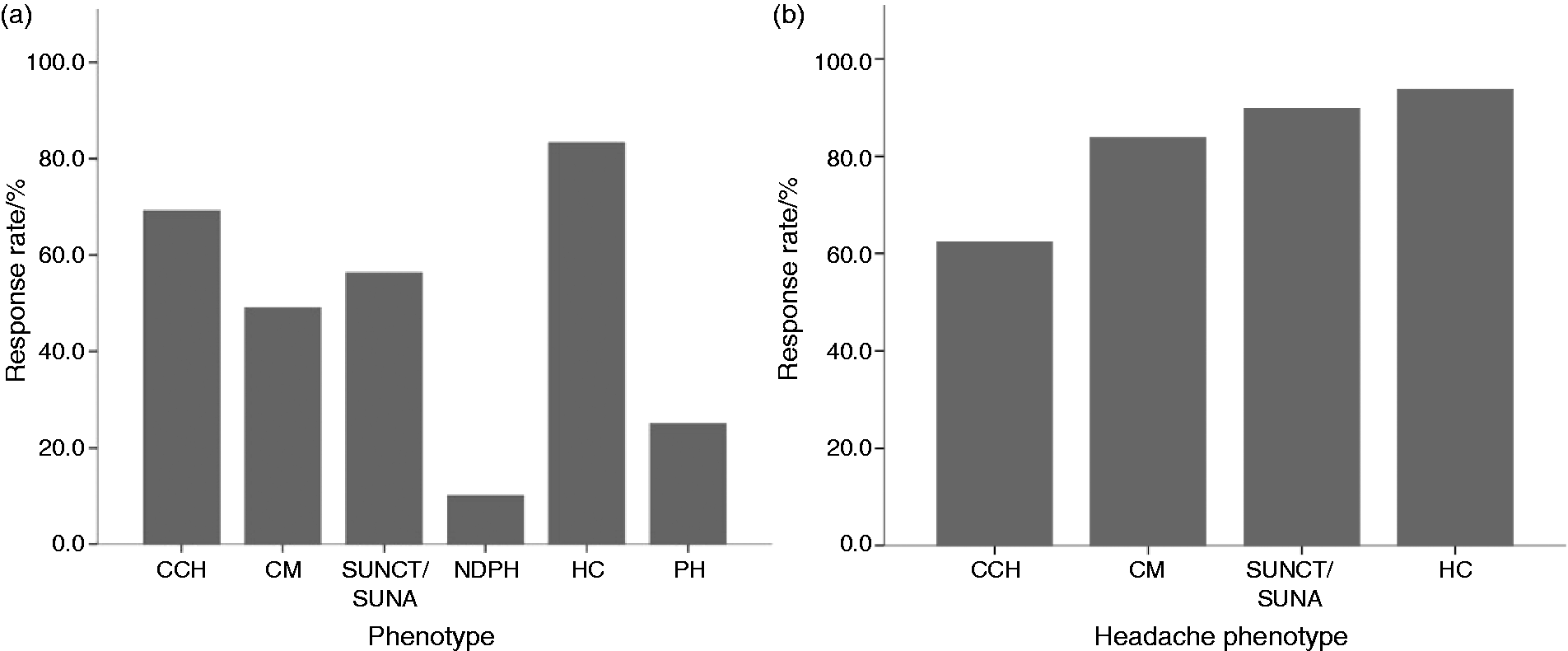
Chronic cluster headache (see Table 3 and Table 4)
Outcome at 2 weeks for all headache types.

CCH: chronic cluster headache; CI: confidence interval; CM: chronic migraine; HC: hemicrania continua; MCNB: multiple cranial nerve block; N/A: data not available due to single responder; NDPH: new daily persistent headache; PH: paroxysmal hemicrania; SUNCT: short lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA: short lasting unilateral neuralgiform headache attacks with autonomic features; VRS: verbal response scale.
Outcomes after 4 weeks for all headache types.

CCH: chronic cluster headache; CI: confidence interval; CM: chronic migraine; HC: hemicrania continua; MCNB: multiple cranial nerve block; N/A: data not available due to single responder; NDPH: new daily persistent headache; PH: paroxysmal hemicrania; SUNCT: short lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA: short lasting unilateral neuralgiform headache attacks with autonomic features; VRS: verbal response scale.
Chronic migraine (see Table 3 and Table 4)
The response rate in CM at 2 weeks was 49.0% (24/49). In responders (n = 24), moderate-to-severe headache days reduced by 10.04 (95% CI 8.61, 11.46) (p < 0.001). Average number of pain-free days over the first 2 weeks was 4.74 ( ± 5.33) (p < 0.001). Significant improvements were seen in the other measures. After the final 2 weeks, 54.2% (13 patients) were still recording a response. Time to response was 33.58 hours ( ± 41.15), reported duration of benefit was 47.12 days ( ± 23.69) and total reported number of pain-free days after the procedure was 6.33 ( ± 9.00). Mean subjective benefit in responders was 59.95% ( ± 35.44). Results at 4 weeks are shown in Table 4.
Short lasting unilateral neuralgiform headache attack disorders (see Table 3 and Table 4)
Response rate at 2 weeks in SUNCT/SUNA was 56.3% (9/16). In responders (n = 9), attack frequency reduced by 95.7% ( ± 7.36) to 0.33 ( ± 0.50) (p = 0.003). Pain-free days were 8.78 ( ± 6.18) at 2 weeks compared to zero at baseline (p = 0.003). Significant improvements were observed in attack severity (p < 0.001) but not duration (p = 0.068). At week 4, all nine patients were still exhibiting response. Time to benefit was 29.89 hours ( ± 28.22), total reported benefit was 68.33 days ( ± 70.22) and the total number of pain-free days reported was 11.89 ( ± 14.36). Mean estimated improvement in responders was 67.7% ( ± 39.22). Results at 4 weeks are shown in Table 4.
New daily persistent headache with migrainous features (NDPH) (see Table 3 and Table 4)
In the NDPH group, only one patient from 10 (10.0%) showed response after 2 weeks. This patient reported a 50.0% reduction in moderate-to-severe headache days from 14.00 to 7.00 but still had daily headaches. They did not report meaningful change in daily pain duration or severity. At week 4, the patient had returned to baseline. Time to response was 24.00 hours, duration of benefit was 14.00 days, and the patient did not report any pain-free days post-MCNB. Results at 4 weeks are shown in Table 4.
Hemicrania continua (see Table 3 and Table 4)
Response rate in the HC group was 83.3% (5/6) after 2 weeks. Responders (n = 5) showed a mean reduction of 11.20 (95% CI 6.35, 16.04) moderate-to-severe headache days (p = 0.003). Mean pain-free days after 2 weeks was 11.00 ( ± 2.82) compared to 0.2 ( ± 0.45) (p = 0.001). Significant improvements were seen in all other outcome measures. At week 4, 80.0% (n = 4) still showed a clinical response. Time to benefit was 24.80 hours ( ± 15.59), duration of benefit was 61.80 days ( ± 33.41) and total number of pain-free days post-procedure was 41.80 days ( ± 45.49). Estimated benefit in responders was 96.0% ( ± 8.94). Results after 4 weeks are shown in Table 4.
Chronic paroxysmal hemicrania (see Table 3 and Table 4)
The response rate in CPH was 25.0% (1/4). In the single responder, the average daily attack frequency reduced to zero and the patient reported nine pain-free days. After week 4, the patient still showed a positive response. Estimated improvement in responders was 95.0%. Time to benefit was 0.50 hours, total duration of benefit was 40.00 days, and total number of pain-free days in this time was 20.00. Results after 4 weeks are shown in Table 4.
Reproducibility of MCNB response
The mean number of procedures undertaken and the response rate of repeated MCNB in each headache group are shown in Figure 2(b). Of the 76 patients with an initial response, 45 (56.3%) went on to have at least one further MCNB. The average time between procedures was 6.27 months ( ± 7.42). The average duration of successful repeated procedures was not significantly different from the first MCNB in CCH (52.88 vs. 50.54 days, p = 0.480), CM (37.82 vs. 40.82 days, p = 0.582), SUNCT/SUNA (37.50 vs. 37.00, p = 0.944) or HC (70.25 vs. 52.50, p = 0.229). Repeated MCNBs were not conducted for any PH or NDPH patients.
Adverse events (see Table 1)
In the 24 hours post procedure, nine patients (7.5%) reported side effects: Dizziness in seven (5.8%), blurred vision in one (0.8%) and injection site tenderness in one (0.8%). Adverse events were reported up to one month in 17 (14.2%) patients: Injection site tenderness in seven (5.8%), transient worsening of headaches in three (2.5%), nausea in three (2.5%), neck pain in two (1.6%) and one each of blurred vision (0.8%) and numbness over injection sites (0.8%). All adverse events were transient and resolved fully without treatment.
Discussion
This is the first large series to examine the potential use of MCNB as a transitional treatment for chronic headache. Patients had a protracted history and had failed to benefit from or had reducing efficacy from GONB. In such a group, the choice of alternative transitional treatments is limited. Oral steroids can be considered in CCH but have potentially serious adverse events, intravenous (IV) dihydroergotamine (DHE) may be useful but is increasingly difficult to source in the UK, and both IV DHE and IV lidocaine require a hospital admission. Multiple cranial nerve blocks appear to offer a valuable and potentially efficacious treatment option in such patients. Of the 137 headaches treated, 55.4% showed a positive response after 2 weeks. The response rates by phenotype were: CCH 69.2%, CM 49.0%, SUNCT/SUNA 56.3%, NDPH 25.0%, HC 83.3% and CPH 10.0%. The benefit was maintained at 4 weeks in over half of original responders in CCH, SUNCT and HC. Significant improvements were seen in pain-free days, attack frequency, moderate-to-severe headache days, pain duration and severity. Benefit seemed to be sustained for weeks in those that showed response, except for NDPH where benefit lasted only 2 weeks in a single patient.
As this was a study conducted in a real-life clinical setting, patients could have had concurrent changes to their preventative medications while receiving an MCNB. At the time of MCNB, 60 patients (50.4%) had medication doses changed. However, we would argue that given that there is a considerable delay in the time to effect of preventatitve medication and that drugs being reduced had proved to be ineffective, allowing medication alterations was unlikely to have influenced the data collected within 4 weeks of any medication change. The MCNB are used as a transition treatment, often while waiting for a preventative to take effect, and we therefore think the settings and findings of the study are clinically relevant.
It is difficult to compare our findings to previously published data due to the injection regime being so different. It is even difficult to directly compare studies on GONB in headache, as although widely used there is no set consensus on injection site, constituents and doses of the block, whether the steroids should be used, the injection regime (single shot vs. repeated injections over a short period), the definitions of response and what headaches to treat (24). Similarly, it seems inappropriate to simply compare GONB response to MCNB response, given that all our patients had failed to show sustained response to routine GONB. However, as of yet, there is no other report on outcomes of multiple cranial nerve block injections given in both greater and lesser occipital and trigeminal nerve territories and so we can only discuss in the context of GONB data, which is not ideal, as acknowledged above.
In CCH, our group reported a 57% response to single GONB with median duration benefit of 21 days (5). Placebo-controlled trials of GONB in CCH conducted by Ambrosini et al. (15) and Leroux et al. (16) reported 57% of those treated with steroids being pain free at 4 weeks compared to zero with placebo and 86% of cluster headache patients (14 CCH) receiving steroid showing a more than 50% reduction in attack frequency after 2 weeks versus 59% of placebo (a non-significant difference), respectively.
Two placebo-controlled trials on purely CM patients have been conducted to date. One found no difference in mean duration of headache freedom between local anaesthetic (3.7 days) versus local anaesthetic and steroid injections (1.0 days) in 37 patients (20); yet another found that the active group had significantly greater reductions in headache days (around 9 days) compared to placebo (around 4 days) after one month (19). Open-label studies of GONB in CM recorded response rates of 52% from Weibelt et al. (9) and 48% by Afridi et al. (3).
For other phenotypes, there is very little data and no controlled trials. In SUNCT/SUNA, Pareja et al. found no responders to multiple nerve blocks (13) (including SON, GON, stellate ganglion and retrobulbar targets) in seven patients, whereas a case study from Porta-Etessam et al. described a positive outcome (14). Hemicrania continua responded to GONB in 85% of patients in the Afridi et al. cohort (3). In HC cohorts undergoing combinations of GON, LON and SON, Guerrero et al. reported all nine patients responding for between 2 and 10 months (12). In a study examining the outcome of GON, LON and SON blocks in HC, Antonaci et al. found that 57% responded to SON blocks but zero to either GON or LON blocks (11). The evidence for peripheral nerve blocks in CPH consists of one small open-label series of six patients, none of whom responded to either GON, LON or SON blocks (11).
Given that our response rates to MCNB in patients already having failed to respond to GONB are similar to those quoted for the occipital blocks themselves, this suggests that MCNB have an efficacy in a more resistant patient group than that studied in the GONB literature. It would perhaps be a step too far to suggest that they may have greater efficacy than GONB alone in nerve block naive patients, but it would be interesting to compare the procedures directly to ascertain if this is why they still have similar response rates to GONB despite their use in more refractory patient groups.
The issue of the placebo effect in injectable treatments must be considered when assessing the effect of MCNB and similar procedures. Although it is widely assumed that invasive treatments have a higher placebo rate than oral medication, the studies in headache on the placebo effect of injectable treatments is still lacking. In the studies mentioned above, different injection protocols and the use of lidocaine as a placebo all mean the placebo response even to GONB is unknown. In a meta-analysis of GONB in migraine, pooled results show that in terms of pain reduction GONB is significantly better than placebo, suggesting they do have a real treatment effect. However, the use of multiple injections may increase the placebo effect, and this has to be considered when looking at the efficacy of treatments such as MCNB. Clinically, what is important for the patient, especially in complex and refractory groups, is if patients exhibit a useful benefit even if the placebo effect cannot be quantified. When the procedure does appear to be safe and well tolerated, a pragmatic approach should surely be applied to help highly disabled patients.
The adverse event profile of GONB in headache patients has been favourable with most cohorts reporting only minor adverse events of injection site pain, dizziness and neck pain being most common. Our cohort found a very similar adverse event profile to those published in GONB despite the increase in injection sites.
It is important that transitional treatments work quickly, and that is why we examined the effect of MCNB after 2 weeks. It is also important that any benefit is sustained, and this study shows that this is the case. Equally essential is a favourable adverse event profile and, again, our data shows this. Furthermore, we show a reproducible effect in responders, which may allow significant periods of relief from chronic headaches in patients failing to respond to standard GONB. As with GONB, the repeated use of MCNB avoids the cost and side effects of oral steroids, IV DHE or IV lidocaine.
In conclusion, our study suggests that MCNB can be rapidly efficacious in chronic headache, providing reproducible benefit for a number of weeks even in those failing GONB. Our injection protocol appears to offer side effects comparable to GONB. We suggest that MCNB could be a useful addition to the transitional treatments already used for chronic headache.
Footnotes
Clinical implications
Peripheral nerve blocks are widely employed in the transitional treatment of a wide variety of headache disorders.
Multiple cranial nerve blocks of the greater and lesser occipital nerves, auriculotemporal, supraorbital and supratrochlear nerves can be effective even in patients who have failed to respond to greater occipital nerve blocks alone.
The effects of multiple cranial nerve blocks can be rapid in onset and can last a number of weeks.
Side effects appear to be comparable to greater occipital nerve blocks.
Acknowledgements
We would like to thank our headache specialist nurses for their help with completion of the clinical database and management of the patients. We also thank the patients and their families for help with this project.
Contributors
Sarah Miller: Author. Analysed and interpreted data; drafted and revised the manuscript for intellectual content; Susie Lagrata: Author. Major role in acquisition of data; revised the manuscript for intellectual content; Manjit Matharu: Author. Design and conceptualised study, revised the manuscript for intellectual content.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SM has received educational and travel grants and payment for the development of educational presentations from St Jude Medical, Medtronic and Allergan. SL has received honoraria from Allergan and Novartis for attending advisory meetings and preparing educational material. MSM serves on the advisory board for Allergan, St Jude Medical, Medtronic and Eli Lilly and has received payment for the development of educational presentations from Abbott, Medtronic, Allergan and electroCore.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.