
Abstract
Background: Misdiagnosis of hemicrania continua (HC) is common. It is diagnosed according to the criteria of the International Headache Society (IHS), but in clinical practice, these criteria seem too restrictive and many hemicrania continua-like headaches remain unclassified.
Subjects and methods: We retrospectively studied the patients fulfilling the IHS criteria for HC. In addition, we identified a group of patients who met all criteria minus cranial autonomic features (HC-A) or minus a complete response to indomethacin (HC-I). We compared epidemiological profiles, clinical features and therapeutic responses to drug(s) between the groups. In addition, we reviewed the literature and critically analysed the diagnostic criteria for HC.
Results: Sixty-two patients with a putative diagnosis of HC were identified. Thirty patients (48%) fulfilled the IHS criteria for HC. Thirty-two (52%) patients failed to satisfy one of the features of HC. Thirteen patients (21%) did not show any evidence of cranial autonomic feature during the episodes of the exacerbations (HC-A). Another 19 patients (31%) did not show a complete response to indomethacin (HC-I). Epidemiological and clinical features of all three groups were compared. None of the differences were statistically significant.
In review of the literature, we noted that cranial autonomic features, a sense of restlessness/agitation during exacerbations, and response to indomethacin (marked to complete) are the specific features of HC. However, these features may not all be present in all cases.
Conclusion: Present diagnostic criteria are too restrictive. We suggest adding the site of pain in the criteria, as described for trigeminal autonomic cephalalgias. Cranial autonomic features, a sense of restlessness during exacerbations, and marked to complete response to indomethacin are three characteristics features of HC. We suggest that the presence of any two may be sufficient to diagnose HC.
Introduction
Hemicrania continua (HC) is an uncommon primary headache disorder. Misdiagnosis of HC is common (1,2). The diagnostic criteria for HC have been repeatedly modified and revised over the past 10 years (2,3). A large number of secondary causes have been reported in the recent past (4). The characteristic features of HC are: (A) strictly unilateral continuous pain (moderate, fluctuating); (B) at least one ipsilateral cranial autonomic feature; and (C) complete response to therapeutic doses of indomethacin (5). Strictly unilateral continuous pain is the central feature of HC. All three characteristic features are essential to satisfy the International Headache Society (IHS) criteria for HC. However, a subset of patients with HC may not have both cranial autonomic features and a response to indomethacin (6–8). In this retrospective study we compared HC (fulfilling the IHS criteria) with HC-like headache missing either autonomic features or complete response to indomethacin.
Materials and methods
This study was conducted as a retrospective chart review of all patients with a putative diagnosis of HC seen in neurology department in our institute from July 2006 to September 2011. The patients having a diagnosis of HC or HC like headache and with a minimum follow-up of 3 months duration were included in the study. We reviewed each individual chart with a putative diagnosis of HC. A few patients were interviewed by telephone to complete the follow-up. Exclusion criteria were: (a) a possible secondary HC; (b) patients who were never subjected to neuroimaging, as we did not rule out the possibility of secondary HC in these patients; and (c) a follow-up of <3 months duration. The study did not require approval by the local ethics committee as per the local regulations for retrospective observation. Patients reported earlier from our institute were included to complete the data. We divided the patients into three broad groups: (a) HC fulfilling the IHS criteria (HC); (b) HC-like headache without complete response to indomethacin (HC-I); and (c) HC-like headache with no cranial autonomic feature (HC-A). We compared typical HC with other two groups separately (HC with HC-I and HC with HC-A). In addition, we reviewed the literature and compared our data with other large case series. The majority of patients were seen and examined by a neurologist (SP) who has a special interest in headache disorders. A few patients (three) were initially seen by a physician (internal medicine). The diagnoses of these three patients were later reconfirmed by the neurologist (SP).
Data are presented as percentage or as arithmetic mean with SD. Student’s t-test was used to compare the continuous data. The chi-square test with Yates’s correction was used for categorical data. In addition, the odds ratio (OR) with 95% confidence interval (CI), when deemed necessary, was calculated. All p-values were two-tailed, and a p-value < 0.05 was defined as statistically significant.
Results
Epidemiological profiles and clinical features in HC, HC-A, and HC-I.

HC: hemicrania continua; HC-A: HC-like headache without any cranial autonomic feature; HC-I: HC-like headache without complete response to indomethacin.
Details of exacerbations in HC, HC-A, and HC-I.

HC: hemicrania continua; HC-A: HC-like headache without any cranial autonomic feature; HC-I: HC-like headache without complete response to indomethacin.
Details of indomethacin and other drugs used in HC, HC-A, and HC-I.*
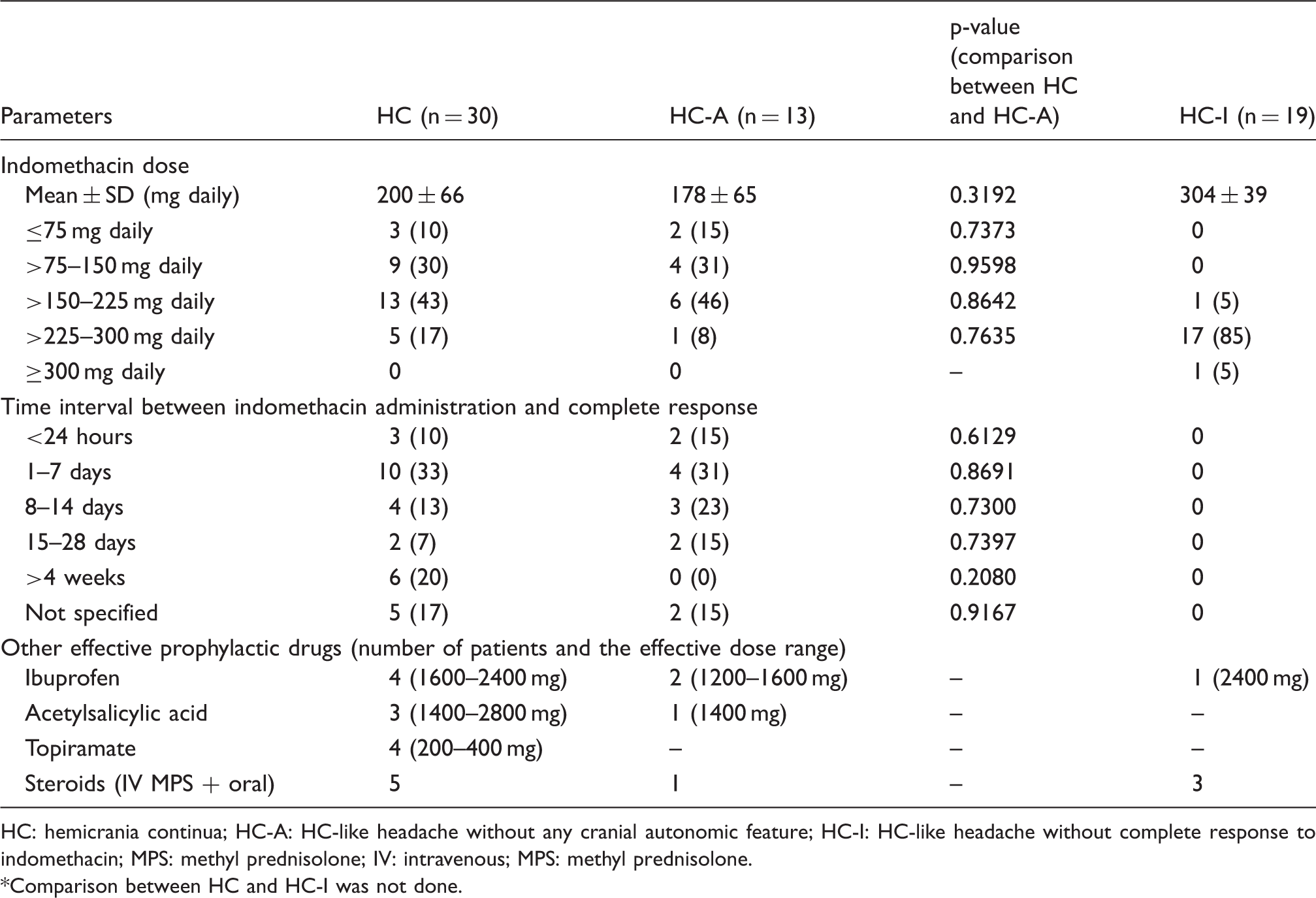
HC: hemicrania continua; HC-A: HC-like headache without any cranial autonomic feature; HC-I: HC-like headache without complete response to indomethacin; MPS: methyl prednisolone; IV: intravenous; MPS: methyl prednisolone.
Comparison between HC and HC-I was not done.
Epidemiological and clinical features
There were no statistically significant differences in any parameter between the groups (Table 1). Orbital/retro-orbital was the most common site of pain in all three groups. Frontal and temporal regions were the two other common sites of pain.
Conjunctival injection and tearing were the two most common cranial autonomic features. Nine patients (30%) in HC group and six (32%) in HC-I group had a history of only one autonomic feature. Nine patients (30%) of HC group did not give a history of autonomic feature at the time of first visit. Autonomic features were noted in a few patients (five patients, 17%) by us during a few episodes of exacerbations. The patients were unaware of these features. A few patients noted autonomic features after the first visit. Four HC (13%) and five HC-I (26%) patients reported autonomic features during the follow-up. We did not find any relation between response to indomethacin and presence of cranial autonomic features.
Ten HC patients (33%), seven HC-I patients (37%) and five (38%) HC-A patients fulfilled the criteria for migraine during the exacerbations.
Exacerbations
There was marked variability in the duration of the exacerbations (Table 2). Exacerbation of > 60 minutes to < 1 day were noted by 90% of patients with HC, 77% of patients with HC-A, and 82% of patients with HC-I. Exacerbations of 5–60 minutes’ duration were noted in about 60% of patients in all three groups. Forty-seven percent of the patients with HC noted exacerbations of even less than 5 minutes. However, only two patients (7%) with HC had exacerbations exclusively for <5 minutes (paroxysmal hemicrania with interictal pain was ruled out because of the presence of moderate background pain). Twenty-seven percent of patients with HC noted headache exacerbations lasting for more than 1 day. However, none of the patients had headache exacerbations exclusive for more than 1 day. None of the patients in any group showed any circadian periodicity.
Response to indomethacin
Details of response to indomethacin in HC-I.

HC-I: hemicrania continua-like headache without complete response to indomethacin.
The data about other medications were not complete (especially for the drugs that were used before reporting to our institute). We included only those drugs with which patients noted complete improvement. Ibuprofen, acetylsalicylic acid, topiramate, and steroids were effective in a few patients in both the HC and HC-A groups (Table 3). Prospectively, we gave topiramate to eight patients in the HC group. Topiramate was started because of the development of side effects of indomethacin. Four patients showed a complete response to the drug.
Twenty patients with HC (67%) and seven with HC-I (54%) were subjected to tapering off indomethacin. None of the patients were successfully weaned off indomethacin. Sudden withdrawal of indomethacin (because of the side effects of indomethacin or poor compliance) was noted in 22 patients with HC and 8 patients with HC-A. The headaches reappeared within 6–48 hours in the patients. Thirteen patients with HC-I had at least 50% response in the headaches. Nine of these patients also had a history of sudden withdrawal of indomethacin. Even in these patients, sudden withdrawal of the drug led to the reappearance/aggravation of the headaches to the previous level within 6–24 hours. We did not find any relation between response to indomethacin and the presence of any clinical features. The response to indomethacin was independent of cranial autonomic features, restlessness/agitation, site and character of pain, and duration/frequency of exacerbations.
Discussion
We identified 62 patients with a putative diagnosis of HC. Thirty patients (48%) fulfilled the IHS criteria for HC. In the literature, we noted four case series with more than 20 patients with a putative diagnosis of HC. Peres et al. (6) reported 34 patients with HC, 25 patients having cranial autonomic features. Marmura et al. (7) reported 43 patients with HC-like headaches responsive to indomethacin. However, only 24 patients reported autonomic features. Rossi et al. (1) reported 25 patients fulfilling the IHS criteria for HC. Recently, Cittadini and Goadsby (3) reported 39 patients with hemicranial headache, with 33 patients fulfilling the IHS criteria for HC. With 30 patients, our case series is probably the second largest case series. In addition, we reported 32 additional patients in whom one of the features of IHS criteria for HC was missing.
Strictly unilateral continuous head pain is the central feature of HC. Strictly unilateral continuous aches with some resemblance to HC are: strictly unilateral migraine, strictly unilateral tension headache, indomethacin-responsive cluster headache with interictal pain, paroxysmal hemicrania (PH) with interictal pain, cervicogenic headache, atypical facial pain, and temporomandibular joint disorders (9).
Migraine was less likely in our patients because of the presence of: continuous background pain, no history of episodic migraine, presence of restlessness in a few patients, and a response to indomethacin.
In HC group, strictly unilateral tension headache, cervicogenic headache, atypical facial pain, and temporomandibular joint disorders were less likely because of pain in the orbital/supra-orbital/temporal areas, presence of autonomic features, and response to indomethacin.
Interictal pain is a well-known feature in patients with PH and cluster headache (CH) (10–14). Marmura et al. (10) reported 27 patients with CH having interictal pain. Only ten had some degree of pain all the time and ten reported interictal pain for less than half of the time. From these observations, it can be said that the presence of mild and intermittent interictal pain favor the diagnosis of either PH or CH. Moreover, frequency and duration of exacerbations may also help in differentiating these primary headache disorders (discussed below in details). A wide variation in duration and frequency of the exacerbations (a few minutes to a few days) (1,6,15) in a patient with continuous baseline headache may be suggestive of HC.
The diagnostic criteria of HC have been revised on many occasions in the past. Below we review the various diagnostic criteria with our case series and other large series published in the literature.
Unilaterality and site of pain
Three patients (8%) of the Cittadini and Goadsby (3) case series had side-alternating attacks. We noted eight more cases in the literature in which side-shifting hemicranial attacks were reported (16–22). None of the patients in our case series reported side-alternating attacks. As side shifting is very rare, a diagnosis of HC should be considered only with strictly unilateral headache.
Sites of pain in HC, CH and PH (in %).

HC: hemicrania continua, CH: cluster headache, PH: paroxysmal hemicrania.
Orbital and retro-orbital are described separately.
These three were the most common sites; details not available.
Parietal and occipital regions are described separately.
Cranial autonomic features
The usefulness of cranial autonomic features for making the diagnosis of HC has been debated over the years. On this issue Marmura et al. write (7) ‘Perhaps autonomic symptoms in HC are more subtle and underreported … the ICHD-II classification is wrong, or subsets of HC exist.’ We agree with these authors. In fact, nine patients of our HC group (30%) did not give a history of autonomic features at the time of first visit. In five patients (17%), autonomic features were noted by us during a few exacerbations of the headaches, and the patients were unaware about these features. Four patients (13%) reported autonomic symptoms during the follow-up.
The discrepancy between objective and subjective data has also been noted in patients with CH (25). Barón et al. (25) studied conjunctival injection during CH attacks. Eight out of the nine patients mentioned having only ipsilateral conjunctival injection during the attacks. However, during objective assessment, the authors noted bilateral conjunctival injection in all the patients. This observation indicates that objective assessment of autonomic feature is important before labeling the patients as not having autonomic features.
The presence of autonomic features is related to the intensity of the headaches. Three to seven percent of patients with CH may never have autonomic features during CH attacks (26). Martins et al. (26) suggested that autonomic features are less likely to occur in patients with moderate to severe rather than excruciating attacks of pain. The intensity of exacerbations in HC is much less than attacks of CH. Therefore, absence of autonomic feature is more plausible in HC than CH. ICHD-II acknowledges the diagnosis of CH in the absence of cranial autonomic features. Therefore, we suggest that IHS should acknowledge the diagnosis of HC in the absence of autonomic symptoms.
Response to indomethacin
A response to indomethacin as ‘sine qua non’ for making a diagnosis of HC has been debated in the past (8,27–29), and various authors suggested a possibility of indomethacin-resistant HC (7,8). HC-like headaches unresponsive to indomethacin were three times more common than typical HC in Marmura et al.’s case series. In our case series, complete response to indomethacin was not present in 19 patients (31% of total patients with hemicranial headache). Thirteen of these 19 patients showed marked or >50% improvement in the baseline headaches, and these patients categorically said ‘they never got such an improvement in their headaches by any other drug in the past’. The headaches reappeared when these patients skipped or withdrew the drug (indomethacin). This suggests that indomethacin was pivotal in relieving/reducing the headache intensity.
About Marmura et al.’s case series (7), the authors write (29), ‘Among our non-responsive patients, many reported significant improvement on follow-up after an extended trial of high-dose indomethacin …’. Besides, there are many other case series/reports in which response to indomethacin was either incomplete or not present in HC-like headache (8). These observations suggest that a subset of patients with HC may not show complete response to indomethacin. Moreover, a few patients may show delayed response to indomethacin. Six patients (20%) took >4 weeks to show complete response to indomethacin. Three of these cases were reported earlier in detail elsewhere (30).
A complete or absolute response to any drug in any disease seems to be an overstatement. Besides, all chronic painful conditions, including chronic daily headache, are known for their refractoriness (31). Therefore, a possibility of HC unresponsive or partially responsive to treatment (indomethacin) exists.
A response to treatment as an essential feature is well acknowledged by IHS in a few other headache disorders (giant cell arteritis, Tolosa–Hunt syndrome, and retropharyngeal tendonitis) (5). In the criteria for giant cell arteritis, response to treatment is read as ‘headache resolves or greatly improves within 3 days of high dose steroid treatment’. We suggest similar therapeutic response for HC in the diagnostic criteria and suggest a change in the sentence ‘Complete response to therapeutic doses of indomethacin’ to ‘Headache resolves or greatly improves to therapeutic doses of indomethacin.’
Recent observations suggest that many other drugs may produce complete and persistent effects on HC headaches (32). These again suggest that response to indomethacin should not be an essential feature for making the diagnosis of HC. This prevents one from making a diagnosis of HC if a patient shows a response to another drug before a trial to indomethacin. This also prevents one from making a diagnosis of HC for a patient who cannot take a trial of indomethacin because of coexisting contraindication for the use of indomethacin.
Agitation/restlessness during exacerbations
Recently, Cittadini and Goadsby (3) suggested that agitation or restlessness should be included in the criteria. They noted restlessness/agitation in 69% of their cases. In our observation, agitation or restlessness was noted in 60% of patients with HC. It was present in more than 50% of patients in both HC-A and HC-I. Therefore, it can be said that agitation or restlessness may be an important feature of HC. Restlessness or agitation is classically described in CH attacks and it is noted 60–95% of patients with CH. The presence of restlessness/agitation in 60–70% of patients with HC suggests that it should be the part of the diagnostic criteria. Inclusion of this would serve two purposes: (1) It would provide an alternative to the presence of autonomic feature (as provided in the diagnostic criteria for CH) and to response to indomethacin; and (2) its inclusion would help in differentiating HC from other continuous hemicranial headaches (such as side-locked chronic migraine, unilateral tension-type headache, unilateral new daily persistent headache, and cervicogenic headache), as other continuous hemicranial headaches are not known to have restlessness or agitation.
Other clinical features and their role in diagnosing HC
The literature is almost silent about the frequency and duration of the exacerbations. In Newman et al.’s (24) case series (10 patients), the duration of the exacerbations was between 20 minutes and 12 hours. Our observations suggest that marked variability in the duration and frequency of exacerbations exist (Table 2). In Peres et al.’s (6) case series, 71% of patients met the IHS criteria for migraine during the exacerbation periods. In Rossi et al.’s (1) case series, 32% fulfilled the diagnostic criteria for CH in the exacerbation period. These observations indirectly suggest that duration and frequency usually vary between 30 minutes and > 1 day. The three closest differential diagnoses to HC (side-locked chronic migraine, PH, and CH with interictal pain) could be differentiated with the help of the frequency and duration of the exacerbations. The frequency and duration of the exacerbations are well defined in the diagnostic criteria of these primary headache disorders (5–30 min for PH, 15–180 min for CH, and 4–72 hours for migraine) (5). Marked variability in the duration and frequency of the exacerbations in a patient (not exactly fitting in migraine or CH or PH) may be suggestive of HC.
Proposal to modify diagnostic criteria
Proposed diagnostic criteria for hemicrania continua.

We further suggest including the presence of restlessness or agitation during exacerbations in the diagnostic criteria, as this is noted in two-third of patients with HC. The presence of restlessness will not help in differentiating HC from PH and CH, but it will help in differentiating HC from other headache disorders (including migraine).
We suggest a change of the sentence ‘Complete response to therapeutic doses of indomethacin’ to ‘Headache resolves or greatly improves to therapeutic doses of indomethacin’, as indomethacin may reduce headache intensity markedly and dramatically but not completely. Moreover, HC unresponsive (or mildly responsive) to indomethacin and HC responsive to other drugs also exist. Therefore, even a marked response to indomethacin should not be a mandatory feature.
Our review of the literature suggests that autonomic features may not be present in each patient or may go unnoticed by patients. If CH can be diagnosed without the presence of autonomic features, it should not be an essential feature for HC.
Our review of the literature further suggests that although autonomic features, restlessness or agitation during exacerbations, and response to indomethacin are specific features of HC, none of these features should be mandatory for making the diagnosis of HC. Therefore, we suggest that presence of any two of these should be sufficient for making the diagnosis of HC.
The current IHS criteria for HC are too restrictive (at least for clinical purpose) and because of this there is underreporting or a lack of reporting of HC-like headaches (8). Broader criteria will inspire to study such type of headaches and would provide broader view of HC and HC-like headaches. We suggest large prospective or retrospective studies from multiple centers to validate the different criteria proposed for HC. However, until the underlying pathophysiology of HC is understood or criteria are validated, it will be better to use more accommodating criteria for clinical purposes (as suggested by others) (33–35). We suggest including such broader criteria, at least in the ‘Appendix’ section of the IHS classification.
Limitations of our observations
This is a retrospective study and the possibility of unrecognized selection bias exists. As it is retrospective, we cannot rule out other primary headache disorders. We did not have the facilities to do “indo-test”. Although we included only those patients who had normal neuroimaging, we cannot rule out other secondary headaches, as full evaluation for secondary headache was not performed. Our sample size was not large enough to uncover the true differences between HC and HC-like headaches. In addition, our observations cannot be generalized as our sample of patients may not truly represent patients with hemicranial headaches owing to referral and other biases.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
None declared.