
Abstract
Many people experience headaches that do not fulfil the International Headache Society's criteria for a specific headache disorder yet behave biologically like that disorder. Others fulfil criteria for one headache disorder and yet have features of another disorder. To explain these observations, we propose that groups of neurones called modules become activated to produce each symptom of a primary headache disorder, and that each module is linked to other modules that together produce an individual's headache. This theory has implications for the classification, research and treatment of primary and secondary headache patients.
Keywords
Introduction
The International Headache Society (IHS) (1) was initially established for research purposes, but it has expanded its classification system so that practitioners can accurately diagnose patients' primary and secondary headaches. However, in clinical practice the criteria often fail to delineate a unique diagnosis, either because a headache fulfils criteria for more than one headache type (for example, it meets criteria for both migraine and tension-type headache) or because a headache does not fulfil any single criteria completely. Furthermore, a person may have one type of headache predominating at one point in his or her life and later manifest another type. A patient who fulfils the criteria for two different disorders may still have one underlying biology.
Patients who have features typical of one primary headache disorder and an additional feature typical of a second disorder have been identified. Examples of this include bilateral cluster headache, cluster headache with aura and cyclic migraine. Disorders that have mixed features of two primary headache disorders that behave and respond medically as an amalgam of two disorders have also been described. Examples of this include cluster-migraine and cluster-tic disorder. Headache patients may fail to exhibit a diagnostically important feature of a primary headache disorder yet in all other ways fulfil criteria for that disorder, for example migrainous disorder and aura without headache. Finally, one disorder may be completely subsumed within another: idiopathic stabbing headache may occur independently but is considered a secondary manifestation of migraine when it is associated with that disorder (Table 1).
The spectrum of atypical primary headaches

One way to analyse this overlap of headache features is to construct a list of diagnostic symptoms that map to the primary headache disorders (Table 2). A diagnostic symptom of one disorder is frequently seen in another disorder. For example, nausea is seen in 87% of migraine patients but is also seen in more than half of cluster, hemicrania continua and chronic tension-type headache patients. Throbbing pain occurs in one-half to one-quarter of the time in hemicrania continua, chronic paroxysmal hemicrania and chronic tension-type headache. Episodic tension-type headache is excluded by definition from having too many features of migraine, and yet unilaterality, throbbing and photophobia or phonophobia are quite common. This suggests that all these headaches, including migraine, share basic mechanisms.
Diagnostic features across various primary headaches

U, unknown; E, excluded by IHS definition of migraine with aura (which calls any headache following an aura a migraine) or by definition of episodic tension-type headache, which excludes nausea. Table of headache symptoms across five primary headache disorders:
1Anthony and Rasmussen (16);
2Marcus, Nash, and Turk (17);
3Leone, d'Amico et al. (18);
4Raskin and Schwartz (19);
5Pfaffenrath and Isler (20);
6Silberstein, Niknam et al. (21);
7Rozen, Niknam et al. (22);
8Inan, Tulunay et al. (23).
Current theories of headache pathogenesis cannot explain the whole spectrum of primary headaches and their variations. The continuum theory (2) addresses the relationship between tension-type headache and migraine but does not explain the other variations that have been described. We have developed a conceptual model to explain these observations. This new model can be tested and may eventually allow for improved treatment based on the clinical features of the headache disorder.
The model
Any primary headache may be described as a group of modules, with one module for each of the main clinical manifestations. Modules are anatomically and functionally linked to one another and become activated in a manner characteristic for the individual.
Modules
A module is a group or network of neurones within the brain, blood vessels, and possibly other organs that produce a feature or symptom of headache (Fig. 1). Several of these groups of neurones (modules) are activated during a primary headache. Table 3 lists suspected modules involved in producing primary headaches.
Modules that may be involved in primary headaches

CPH, chronic paroxysmal hemicrania; EPH, episodic paroxysmal hemicrania; HC, hemicrania continua; HH, hypnic headache; SUNCT, short-lasting unilateral neuralgiform headache with conjunctival injection and tearing; TTH, tension-type headache.
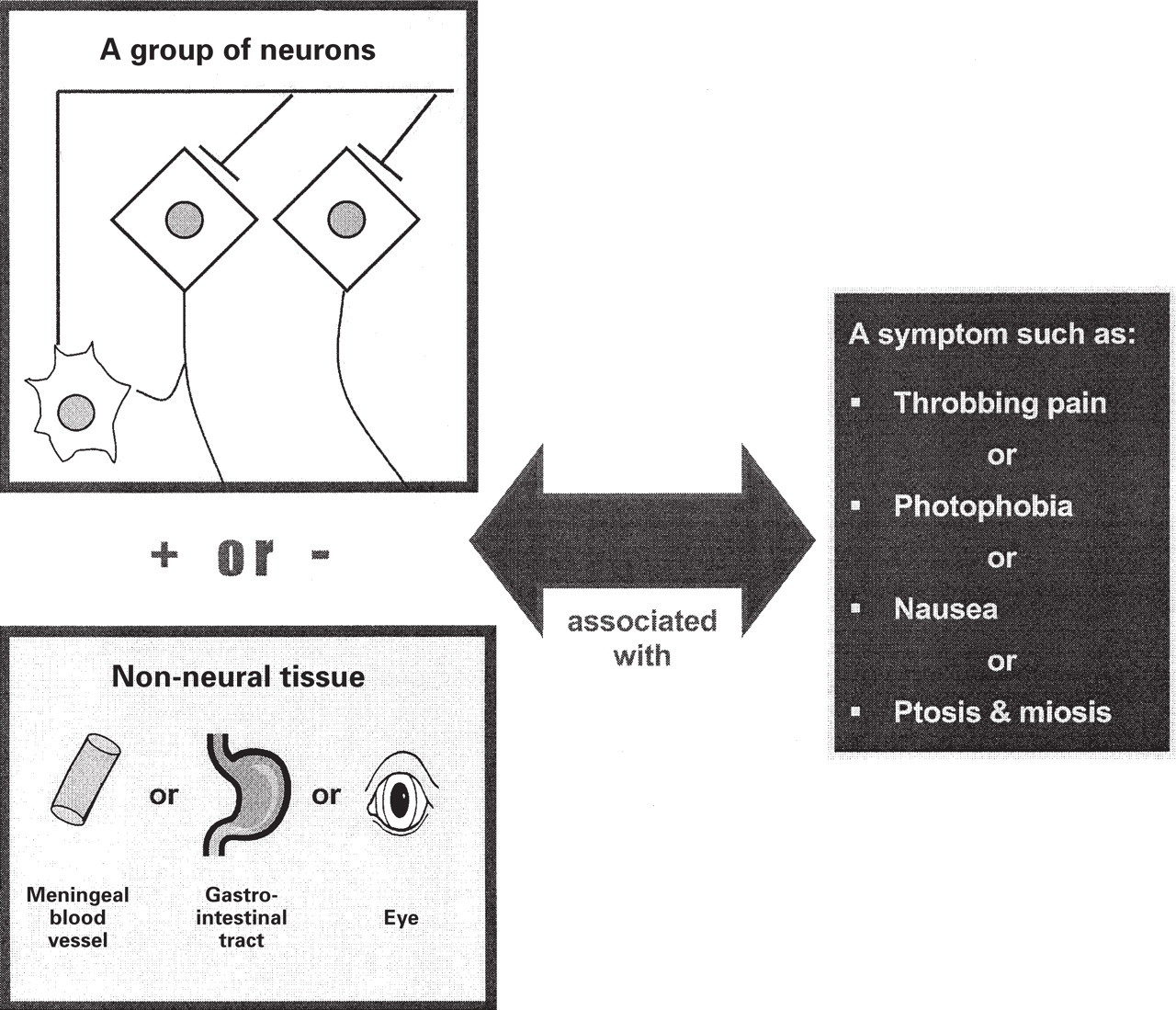
A module is when the neurons in a module are activated a specific symptom of headache is produced. Some modules may have associated non-neural tissue, but most are entirely neural entities.
Migraine without aura may involve at least three modules. One module is associated with throbbing pain. The anatomical correlate is probably the meningeal blood vessels and the nerves that surround them. The physiological correlate is neurogenic inflammation. A biochemical marker for activation of this module is the release of calcitonin gene-related peptide into the jugular venous blood. Another module is associated with nausea. Its anatomical location is the nucleus tractus solitarius. Its physiology is not well characterized but dopamine and serotonin influence its activity. Another module is associated with photophobia and phonophobia. It most likely involves cortical structures and possibly also subcortical structures that are either overly activated by normal light and sound intensities or are not normally suppressed.
Modules may be composed of smaller units that may be combined into a larger module. For example, each type of aura (visual, sensory, aphasic or motor) is a module subunit. One subunit may be activated after another, i.e. a typical visual aura is followed by a sensory aura and then an aphasic aura as different units of the module are activated. Another example is pain location, with pain spreading from a localized area to involve an entire side of the head as the headache worsens. This corresponds to expanding topographic activation until the entire module is involved. It may be that photophobia, phonophobia and osmophobia similarly may act as parts of a single module or ‘module cluster.’
Modules may be activated by degrees, the level of symptoms correlating with the degree of activation. Above a certain threshold of activation a module will recruit other modules and thus produce new symptoms. For example, a headache that is mild but throbbing may not be associated with nausea, but if that module becomes more strongly activated (more intense, throbbing pain), the nausea module may then be recruited. In fact, triptans are effective in all tension-type headaches in migraineurs (3). This may mean that these tension-type headaches are migraines with incomplete symptom expression. The fact that CGRP is elevated in pulsatile chronic tension-type headache (4) is consistent with the activation of a module associated with vasodilation and, in essence, corroborates the concept of modular units.
Headache features that are shared by different headache types presumably share the same module (i.e. nausea in migraine is produced by the same neurones as nausea in cluster headache or in hemicrania continua). However, this may not always be the case. Young and Rozen (5) proposed that an active process occurs in cluster headache that suppresses the development of cluster headache symptoms on the non-headache side. According to this theory, this process would be accomplished by a unilaterality module that is tightly linked to other modules that are involved in cluster headache. The existence of unilaterality as a feature of other headache types suggests that a suppressor is also involved in these other conditions. There may be a single suppressor module, with the cluster suppressor a different module than the suppressor for migraine, hemicrania continua or any of the headaches that are typically unilateral.
Modular brain organization may be an intrinsic design feature that applies to functions other than producing headache. For example, schizophrenics with auditory hallucinations do not activate the monitoring module that is activated during the imagination of spoken phrases by non-schizophrenic individuals (6). Many other regions of the brain that could function as modules are activated during normal brain activity, as demonstrated in the expanding functional neuroimaging literature.
Links
Links, too, have a neuroanatomical basis and coordinate the sequential or concurrent activation of modules (Fig. 2). The physiological result of the links between modules may be neuronal windup or a similar process. Windup is known to occur in non-headache pain models (7). Long-term potentiation or other forms of ‘learning’ could explain how patients develop relatively stable headache symptoms. Modules become sensitive to future activation or their links are strengthened by repeated headaches.

Simplified model of migraine without aura. Migraine without aura may involve at least three modules, one each for throbbing pain, photo/phonophobia and nausea. Through anatomical links, one activated module may cause neuronal windup and thus activate another module.
Some links occur more commonly than others; there may be a greater likelihood for a particular module to be linked to one module rather than another. For example, aura is more likely to be linked to a throbbing head pain module than to pain that would otherwise be part of a cluster or tension-type headache. We propose that a migrainous headache is more likely to reinforce or activate the aura module than the modules involved in cluster headache. A bidirectional process of reinforcement may govern the interaction between two modules. Thus, aura without headache does not reinforce itself by interacting with a headache module and is proportionately less common than aura with headache (although there is a gradient of preference among the headache types). Strong links between throbbing headache and nausea may be due to neuroanatomical proximity or to specific neuroanatomical connections between the trigeminal nucleus caudalis and nucleus tractus solitarius.
Complete migraine (8), in which a migraine prodrome is followed by an aura, then a headache, then a resolution phase, and finally a postdrome, could represent a sequential linkage of modules (Fig. 3A). The prodrome module becomes active and initiates the aura module, which then initiates the migraine-without-aura group of modules, etc. Alternatively, another module, which could be termed a generator or sequencer, orchestrates the activation of modules. For example, activating a cortical sensory module with bright light and a limbic module with stress may activate the other modules in a person's migraine (Fig. 3B). Finally, modules might be recruited in a ‘herd’ fashion to create a migraine headache. One module may not suffice to activate a self-reinforcing process involving many modules, but the simultaneous activation of several modules creates the necessary critical mass and all modules become activated (Fig. 3C). The ‘herd’ mechanism may not apply to complete migraine with its mandatory sequence of activation, but may apply to other types of primary headache, including migraine without aura.

Simplified model for complete migraine. (a) Sequential assumption. According to the sequential assumption, the prodrome is the first activated module that subsequently activates the aura module, then the migraine headache module complex. These activate a terminator mechanism (lysis module) that suppresses the headache. In the above scheme, the terminator mechanism activates the postdrome module. Alternatively the postdrome module might be activated by any previously activated module (or in some cases represent persistence of activity of the prodrome).(b) Sequencer module assumption. The sequencer module orchestrates the sequential activation of modules in a headache disorder, in this case complete migraine. (c) ‘Herd’ modular activation: example ‘Herd’ type of modular activation. If enough modules are activated spontaneously or by triggers, or if one is very strongly activated, all other modules are secondarily activated and headache with full symptom expression develops. If the modules are insufficiently triggered, the headache syndrome does not develop.
Further examples
Migraine without aura may involve activating many more modules than those previously described. Some individuals may have a unilaterality module that suppresses head pain on the non-headache side. Others may have activation of a non-throbbing pain module, producing a tension-like pain feature, or an allodynia module. A module that generates stabbing pain may be recruited in many migraine patients (jabs and jolts pain, idiopathic stabbing headache pain).
Goadsby and Lipton have postulated that cluster headache, chronic and episodic paroxysmal hemicrania, hemicrania continua and SUNCT may be grouped together into the trigeminal autonomic cephalgias (9). Their model fits well with a modular headache theory (Fig. 4). The autonomic module and the unilaterality module are presumably the same in all these conditions. The generator of the autonomic symptoms must be very strongly associated with the module that assures the unilaterality of the pain and autonomic symptoms, as simultaneous bilaterality of these disorders is so unusual. The pain module differs either anatomically or physiologically in the three disorders. Alternatively, a timer or termination module may differentiate cluster headache and the paroxysmal hemicranias.

Simplified representation of trigeminal autonomic cephalgias (TACs).
Disorders such as cluster-tic syndrome can be viewed in the context of the modular headache theory. Modules that are typically expressed during cluster headache become linked to modules that produce the lancinating pains of trigeminal neuralgia. The fact that medications effective for either trigeminal neuralgia or cluster headache may work, and that many patients require both types of treatments to control their cluster-tic symptoms, suggests that the ‘herd’ mechanism of module recruitment operates in this disorder.
Secondary headaches can also be explained by the modular headache theory. Concussion, carotid dissection, subarachnoid haemorrhage and meningitis appear to activate the modules involved in migraine with or without aura. The biological underpinnings of chronic post-traumatic headache that can resemble many primary headaches, can be understood as the release or activation of headache modules due to the brain injury or the expectation of headache.
The modular theory may also help to explain the frequent comorbid association of various brain disorders, such as depression and anxiety, with headache. One or more of the headache modules could be linked to the brain regions involved in generating these disorders. Depression may have a bidirectional link with migraine, which would explain why either disorder may precede the other or why more severe migraines are associated with depression (8).
So what?
In a sense this theory does little more than state the obvious: migraine symptoms have a neurological basis and therefore represent the functional activation of physical regions or groups of cells within the brain, and because headache symptoms occur together, they are, of course, ‘linked’. We believe this very simplicity is the strength of the modular headache theory, providing an inherently logical language that describes the disordered brain function that is present during headache. We believe that the modular headache theory provides a useful framework for understanding and treating headaches.
Modern functional imaging techniques may provide a means to identify the locations of modules and perhaps explain how they are linked. The so-called ‘migraine generator’ in the upper pons and midbrain may be one of the first modules to be imaged (10). The function of this putative module is not yet known. More recently, a possible hypothalamic module has been imaged in cluster headache (11). In fact, the entire methodology of functional neuroimaging is based on subtracting out everything but an area of interest, i.e. a module. Besides neuroimaging, markers of cellular activation such as c-fos expression and cellular recording may help isolate modules in animal models of migraine.
Modular headache theory re-frames the questions asked by researchers and allows scientists to more accurately determine the patients to whom their findings apply. Researchers must fully characterize their patients to understand their data. For example, characterizing patients entered into a functional imaging study according to specific symptoms rather than by diagnosis alone will lead to considerably more information.
Modular headache theory has treatment implications. Treatments aimed at only one module may not work, as other modules remain active and reinforce the whole. Thus, therapy that works on several modules may be more effective than monomodular therapy. Abortive or preventive medications may work by deactivating modules, desensitizing them, or weakening the links between them. As modules become precisely defined and their links identified, treatments that are specific to certain modules or that suppress the formation of links will become available. Refining our understanding of the anatomy and physiology of modules and links can help clinicians individualize headache care. Identifying a patient's active modules and how they are linked requires a careful history and relevant physical examination. Modular headache theory links the physician to the individuality of the patient, because the details of the headache history demonstrate the activities and linkages of the modules that the physician and patient are working to suppress.
Finally, modular headache theory, if valid, demonstrates that the IHS classification system is, in effect, an attempt to describe statistically valid associations between modules across a population. Therefore, the best method of deriving a valid headache classification system is to assess headache symptoms (modules) across a population without imposing pre-existing biases. While the associations discovered in this manner will have real biological underpinnings, they will fail to fully describe the true richness of brain symptom expression. Further description of the biological processes that allow modules to become activated, and of the anatomy and physiology of their links, will lead to a more meaningful understanding of the primary and many of the secondary headaches.