
Abstract
The utility of the differences between cluster headache (CH) and paroxysmal hemicrania (PH) is limited by the considerable overlap of their clinical characteristics. We compared 54 patients with CH and eight patients with PH in terms of demographic features, characteristics of headache attacks, associated autonomic features, temporal forms of disorders, and response to verapamil. According to our results, clinical features that distinguished CH and PH patients were: maximal pain localization, ocular in CH patients and extra-ocular in PH group; mean attack duration was longer and mean attack frequency was lower in CH patients in comparison with PH patients. Conjuctival injection was the only autonomic sign seen more frequently in CH patients. There were more CH patients with episodic and more PH patients with unremitting form of the disorder in examined groups. Although statistical analysis pointed out a significant difference between these clinical features, there was no clinical characteristic that exclusively belonged to one of these headache entities. Demographic characteristics (age, gender, social background), the other headache attack features (nocturnal attacks, interattack tenderness), the other autonomic signs, as well as the response to verapamil did not differ significantly between two groups.
Introduction
In 1997, Goadsby and Lipton proposed the term ’trigeminal-autonomic cephalalgias’ (TACs) to encompass a variety of short-lasting primary headache syndromes which are associated with autonomic activation (1). This group includes cluster headache (CH), paroxysmal hemicrania (PH), short-lasting unilateral neuralgiform pain with conjuctival injection and tearing syndrome (SUNCT) and painful exacerbation of hemicrania continua. The proposed anatomical basis of these disorders is the trigeminal-autonomic reflex, which consists of a brainstem connection between the trigeminal nerve and facial nerve parasympathetic outflow.
The TACs are relatively rare headache disorders. The prevalence of CH is estimated to be 0.1% (2). The prevalence of PH is not known, but the relative frequency compared with CH is reported to be approximately 1–3% (3). These disorders are poorly recognized in primary care and thus will be referred to neurologists eventually, offering an excellent opportunity to diagnose and treat these patients, as they have excellent but highly selective response to treatment (4).
The difference between PH and CH is important since treatments for CH are generally not effective for PH. The clinical features that distinguish PH from CH include the female preponderance; higher frequency and shorter duration of the attacks; and exquisite response to indomethacin. The utility of gender as well as duration and frequency of attacks to distinguish PH from CH is limited by the considerable overlap of these characteristics in the syndromes (4).
The objective of this study was to find more solid evidence in order to distinguish two TACs, CH and PH, on a clinical basis.
Methods
Sixty-two consecutive patients affected by TACs, followed during 3 years at the Institute of Neurology, Belgrade, Serbia, were included in the study. These headache patients were referred to our Headache Centre under the diagnosis of the resistant headache. Secondary TACs were excluded in all patients by general examination, haematological and biochemical analyses, ophthalmological examination and magnetic resonance imaging. The diagnosis was made on the basis of a clinical history and a detailed neurological examination, according to the International Headache Society (IHS) criteria (5), including indomethacin response in the PH group. Based on diagnosis, two groups of patients were formed: 54 patients with CH and eight with PH. Two PH patients had attack duration shorter than proposed by IHS criteria (5). The PH diagnosis in these two patients was made as they satisfied all the others IHS criteria for the diagnosis. Demographic features were collected, as well as characteristics of headache attacks (side and localization of maximal pain, attack duration, daily frequency, number of patients with nocturnal attacks and presence of tenderness between attacks) and the autonomic features of attacks (conjuctival injection, lacrimation, nasal congestion, rhinorrhoea, and facial/forehead sweating, miosis, and ptosis or eyelid oedema). The temporal pattern of headaches, episodic and chronic for CH and unremitting and remitting for PH, as well as response to verapamil, was recorded.
Independent-samples t-test, χ2 test and Mann–Whitney U-test were used to compare the results in two groups. The significance level for the analysis was set beforehand at 5% (P < 0.05).
Results
No significant difference was found in demographic features between the two groups (Table 1). One patient in each group had a relative with cluster headache.
Demographic features of patients with cluster headache (CH) and paroxysmal hemicrania (PH)

The pain was localized in ocular (34 patients, 63%), temporal (13 patients, 24.1%), frontal (five patients, 9.3%) and parietal region (two patients, 3.7%) in the CH group. The pain had ocular localization in only one patient (12.5%) in the PH group. Three patients (37.5%) had temporal, two (25%) had frontal and two parietal localization of maximal pain intensity in the PH group. The difference in pain localization was highly significant between groups, with predominance of ocular pain localization in CH patients (Table 2). Right and left sides were nearly equally distributed in both groups; side shifts from one side to the other were noted in one patient with CH and two patients with PH.
Features of headache attacks in patients with cluster headache (CH) and paroxysmal hemicrania (PH)
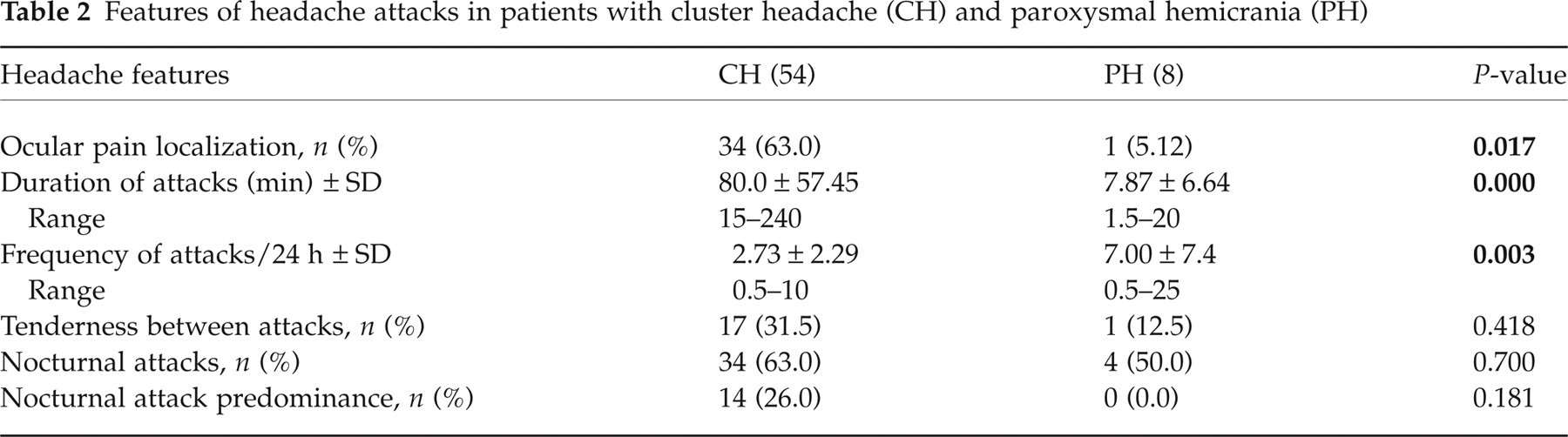
Mean attack duration was longer (80.0 ± 57.44 min) in the CH group than in the PH group (7.87 ± 6.64 min, P < 0.0001). There were no patients in the CH group with attack duration < 15 min and there were no patients in the PH group with attack duration > 20 min. However, 18.5% of patients in the CH group and 25% of patients in the PH group had attack duration of 15–20 min (Fig. 1).
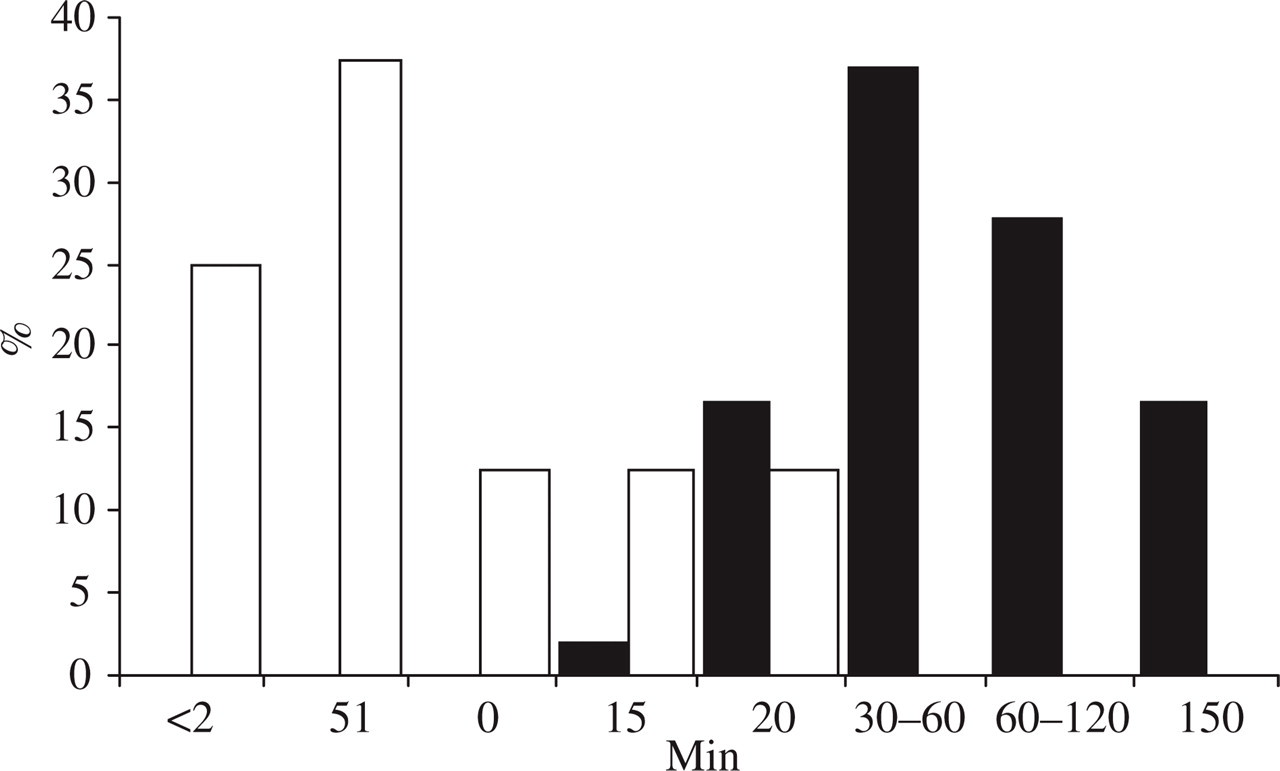
Duration of attacks (%). ▪, CH; □, PH.
Mean attack frequency was higher (7.00 ± 7.43) in the PH group than in the CH group (2.73 ± 2.29, P = 0.003) (Table 2). Thirty-nine percent of patients in the CH group and 75% of those in the PH group had three to six attacks per day (Fig. 2). There was a significant negative correlation between duration and frequency of attacks in the CH (Spearman’s ρ=−0.296, P = 0.030), but not in the PH group (Spearman's ρ=−0.573, P = 0.170).
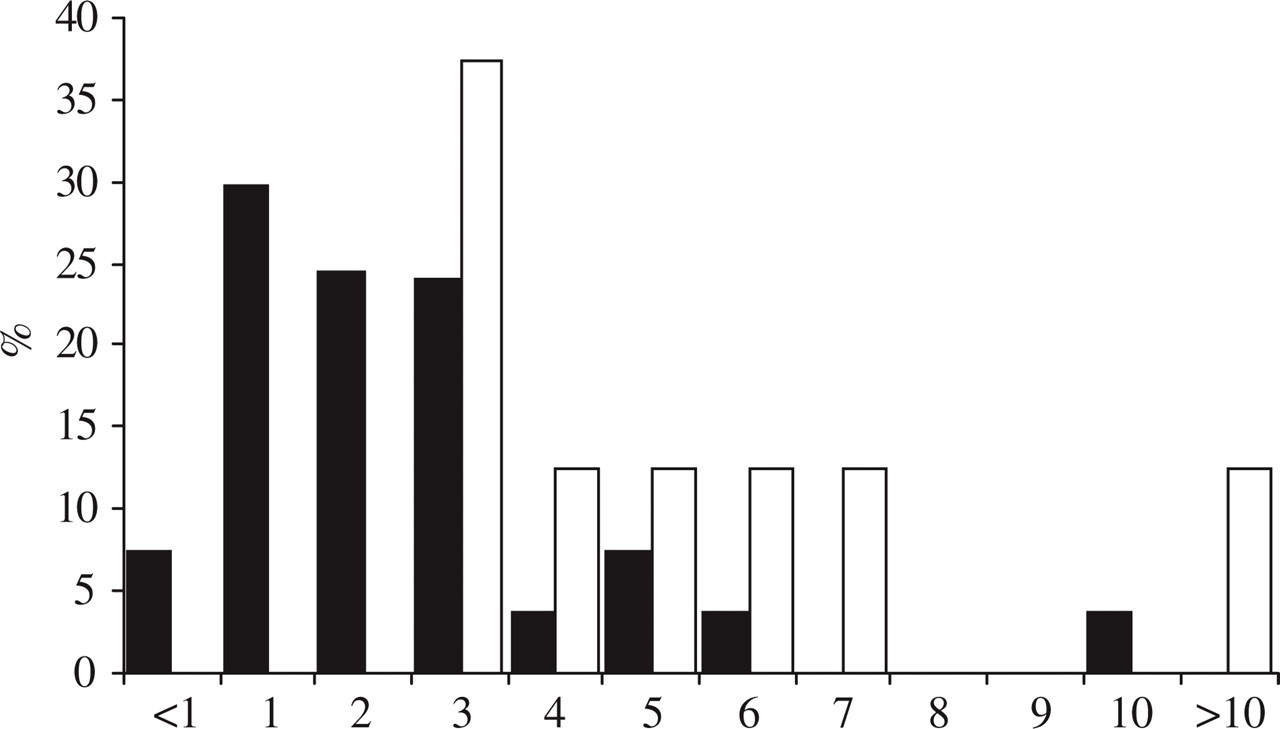
Frequency of attacks. ▪, CH; □, PH.
The most frequent autonomic features were lacrimation, conjuctival injection and nasal congestion in the CH group and lacrimation and nasal congestion in PH patients. Conjuctival injection was the only autonomic sign significantly different between groups (Table 3). The mean number of autonomic signs associated with headache was three in the CH group and two in the PH group.
Autonomic features of patients with cluster headache (CH) and paroxysmal hemicrania (PH)

Nausea was present in 14 patients (26%) in the CH group and absent in the PH group, without significant difference between groups (P = 0.112). Restlessness during attack was noted in 31 (57.4%) patients in the CH group and five (62.5%) in the PH group (P = 0.550).
In the CH group 10 patients (18.5%) had the chronic form; one had the chronic form transformed from a previous episodic form, so the episodic : chronic ratio was 4.4 : 1. In the PH group two patients (25%) had remitting and six patients (75%) unremitting form of the headache disorder, with a remitting : unremitting ratio of 1 : 3. This difference was highly significant (P = 0.001).
All patients in the PH group responded to indomethacin at a daily dosage of 75–150 mg, that was the obligatory diagnostic criterion. Efficacy of verapamil was estimated in 48 patients with CH and six with PH. The treatment was succsessful for 39 patients (81.3%) in the CH and three (50%) in the PH group, without significant difference between groups (P = 0.083). In the PH group two patients experienced a decrease in both frequency and intensity of attacks and one patient had complete relief with verapamil monotherapy. The verapamil efficacy at a daily dosage of 240 mg was archived in six consecutive days and maintained during 4 weeks of treatment. Pain relapsed to the previous temporal pattern in all three PH patients 2 days after cessation of verapamil therapy.
Discussion
The patient group was recruited from those referred to our Headache Centre for resistant headaches. The high relative frequency of PH (14.8%) compared with CH reflects the selection bias, because our Centre is a tertian referral centre in Serbia.
Clinical features that distinguished CH and PH patients were maximal pain localization, duration and daily frequency of attacks, presence of conjuctival injection and form of the disease. Although statistical analysis showed significant differences between the groups, there was no clinical characteristic that exclusively belonged to one of these headache entities.
Beside SUNCT, CH represents the form of primary headache that prevails among males, with a male : female ratio 5 : 1 (6). Regarding paroxysmal hemicrania, originally considered to be a disease of women, a review of 84 patients in 1989 (7) reported a female : male ratio of 2.3 : 1. The clear male prepoderance in CH and female in PH was observed in our patients.
The pain had ocular localization in most CH patients and in just one PH patient. Manzoni (6) described ocular, temporal and frontal location of pain almost equally distributed among his CH patients. The ocular and temporal areas were prevalent sites of maximal pain in patients with PH (8).
Duration and frequency of attacks are different in CH and PH, as proposed by IHS criteria (5). In the present study the significant overlap between two groups (Figs 2), particularly regarding the frequency of attacks, was noticed. Nearly one-fifth of patients in both groups had attacks that lasted 15–20 min and about a half of patients in both groups had three to seven attacks daily.
In both disorders coexisting autonomic phenomena of decreased sympathetic activity and vasodilation: intraocular pressure increase, conjuctival injection, increased sweating and decreased salivation (9, 10) and parasympathetic stimulation: tearing, nasal secretion and miosis (9, 10) form the clinical picture that does not fit with any classic sympathetic or parasympathetic syndrome (11). Lacrimation and nasal congestion were the most frequent autonomic features in both our groups. Conjuctival injection was the only autonomic sign more frequently observed in CH than in the PH group. Increased facial/forehead sweating was not seen in our PH patients. Conjuctival injection and increased sweating were the only markers of decreased sympathetic activity noted in our patients and both were rarely seen in our PH group.
A typical pattern of restlessness described in CH (12) was reported in more than half of patients from both groups.
According to this study, CH was of episodic form in most patients, while the chronic (unremitting) form was prevalent in the PH group. According to the literature, some 80–90% of patients have episodic CH and the remaining 10–20% have chronic headache form (4). Sjaastad coined the term ‘chronic paroxysmal hemicrania’ based on the first two patients, who had lasting, daily, solitary attacks of hemicrania (13). It later became clear that before the development of chronic symptoms, 42% of the patients had passed through a non-chronic stage (3).
Response to indomethacin was, according to IHS criteria, obligatory to establish the diagnosis of PH. However, there were six patients in the PH group also treated with verapamil, prior to indomethacin therapy. The observed verapamil efficacy is in concordance with reports in the literature (14, 15).
There are reports of the concomitant existence of the two disorders (16), as well as of PH and CH continuum, in the same patient (17). Only four of 11 patients in Fuad and Jones’ study (18) met criteria for the diagnosis of PH, while the others had clinical features that could better fit the diagnosis of CH. Based on literature data and the results obtained in our patients, similarities in pathophysiology and clinical features between the two TACs outbalance the differences. At present, in spite of promising results of recent functional (19, 20) and biochemical (21, 22) studies, a reliable biological marker of these headache disorders is not avaliable. The diagnosis is based on clinical presentation, where the overlap of attack periodicity and response to verapamil treatment creates a special difficulty in establishing a proper diagnosis based on clinical features. At present, the therapeutic response to indomethacin remains the most reliable differential diagnostic criterion for CH and PH.