
Abstract
Background
In Norway, as in most other countries, the training program for clinical neurology has no mandatory headache program. Knowledge in headache management must therefore be acquired during everyday clinical training. The objectives of this study were to investigate neurology residents’ knowledge of headache.
Methods
A questionnaire survey was undertaken among neurology residents in Norway.
Results
All 17 neurological departments in Norway participated, and 143 residents responded (86%). Sixty percent were women, mean age was 32.5 years, and the respondents had an average of 28 months clinical training in neurology. Fifty-six percent knew the approximate prevalence of migraine and chronic headache. Thirty-seven percent asked their patients about disability, quality of life, and social functioning at every consultation. Further, 72% would prescribe prophylaxis for chronic tension-type headache and 97% for very frequent migraine. One third wrongly stated that use of the most common headache prophylactics could lead to medication-overuse headache. Headache diaries were used regularly by 63% for diagnostic purposes, and 73% requested an MRI for all long-lasting headaches referred to neurological outpatient clinics.
Conclusion
Although a major public health problem, headache knowledge is moderate at best, and its management clearly varies. There is an unmet need for a better and more structured headache training program in Norway.
Introduction
Migraine and other headaches are the most common cause of disability in people under 50 years of age (1). It has been suggested that headache accounts for 20–30% of all new referrals to neurologists, and all physicians working within neurology should therefore be competent in its management (2). There is limited focus on headache in the curriculum in medical schools both in Norway and throughout the world (3,4). Inadequate medical education has been suggested as a cause of under-diagnosis and under-treatment, leading to low patient satisfaction among headache patients (5,6). Studies suggest that migraine is even under-diagnosed and under-treated in neurologist specialist care, and that very few neurologists pursue headache medicine fellowships (7,8). In Norway, as in most other countries, the national training program in clinical neurology has no mandatory headache program. Therefore, knowledge and expertise in headache management must be acquired during everyday clinical neurology training. Little is known about whether or not these skills are successfully obtained (9). The objectives of this survey were to investigate whether residents acquire the necessary knowledge about headache, and to evaluate experience in, and attitudes towards, headache management among neurology residents in Norway.
Materials and methods
Design and setting
There are 17 hospitals with a department of neurology in Norway, varying from smaller district hospitals (5–6 residents) to larger university hospitals (14–18 residents). In 2016, there was a total of 166 residents at these 17 departments.
The training to become a certified specialist in neurology in Norway includes 1.5 years of internship (usually internal medicine, general surgery, and general practice), followed by five years of training, of which at least 3.5 years must be spent in clinical neurology and six months in neurosurgery. The remaining time can be spent in neurology, research, or another relevant speciality. At least 1.5 years should be at a large (preferably university) hospital. In addition, 220 hours of clinical training courses must be completed, including eight mandatory courses; however, the headache course is optional.
The study was conducted as an anonymous questionnaire survey among neurology residents in Norway in 2016. A contact person at each department was responsible for recruitment.
Questionnaire
The questionnaire was based on available literature and the authors’ experience in headache medicine. It is included as a supplement (Supplement 1). The questionnaire covered background variables including age, gender, education, and neurology training. The participants also answered short multiple-choice or open questions about knowledge, management, experience, use of the national treatment guidelines, the International Classification of Headache Disorders (ICHD), and barriers to optimised treatment for headache.
Outcomes
Knowledge about the prevalence of migraine, chronic headache (headache ≥ 15 days/month for the last 3 months), and comorbid conditions in the general population was tested using multiple-choice questions. In addition, we defined the question about which medication(s) may lead to medication-overuse headache (MOH) as a knowledge question.
Regarding the management of headache patients, the residents were asked how often they used headache diaries, MRI, national treatment guidelines, and the ICHD, with the response options i) every time, ii) two out of three times, iii) half of the time, iv) one out of three times/rarely, or v) never. The categories were reclassified into ≥ 2/3, half of the time, and ≤1/3, due to too few answers in the categories “every time” and “never”.
Three different headache cases: i) Chronic tension-type headache (CTTH), ii) episodic migraine (migraine attack once every 1–2 months), iii) very frequent migraine (1–2 migraine attacks every week) were used to assess the residents’ suggestions for medical treatment for patients with these three variants of the two most common primary headaches.
Self-rated knowledge of four different headaches (migraine, tension-type headache, MOH, and cluster headache/trigeminal autonomic cephalalgias) was scored on a 3-item scale with the options good, moderate, and poor.
To assess the main barriers to optimised management of headache patients, we asked the participants to rank seven statements from 1 to 7 (1 was the most important and 7 the least important barrier): i) “your own insufficient knowledge of headache medicine”, ii) “headache patients are difficult and demanding”, iii) “lack of supervision from senior neurologists”, iv) “lack of opportunity for follow-up appointments at the outpatient clinic”, v) “lack of a multidisciplinary team at the outpatient clinic”, vi) “no effective treatment options for many patients”, and vii) “not enough collaboration with the general practitioners”.
Statistical analyses
For descriptive data, proportions, means, and standard deviations (SD), or 95% confidence intervals (CI) are given. Groups were compared using the t-test (continuous data) or the χ2 test (categorical data). The results of barriers to optimised management were presented and analysed as means due to readability and interpretation although median (and Wilcoxon test) would be the correct statistical choice. There were no differences in the results between these two approaches.
We used multivariable logistic regression to evaluate the effect of age, gender, the number of months in neurology training, hospital status (university hospital or non-university hospital), and whether the resident had attended the headache course during residency on i) knowledge about the prevalence of migraine (yes/no, as the dependent variable), ii) the knowledge that prophylactic headache medications (antiepileptic drugs, anti-hypertensive drugs, antidepressant drugs, and botulinum toxin A) do not induce MOH (yes/no, as the dependent variable), iii) regular use of MRI for all new headache patients (yes/no as the dependent variable), and iv) self-reported lack of headache knowledge as one of the two main barriers towards optimized headache treatment (yes/no as the dependent variable). Results are presented as odds ratios (ORs) with 95% CIs.
Statistical significance was defined by p < 0.05, using a two-sided test. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 25.00 (SPSS Inc, Chicago, IL, USA).
Ethics
The Regional Committee for Medical Research Ethics reviewed the study and the Norwegian Social Science Data Services approved the study. Informed consent was obtained from all participants.
Results
Descriptive data of the participants (n = 143).

Residents’ answers to five questions about migraine and chronic headache. All figures are numbers (%).

Residents’ use of headache diary, imaging and the international classification of headache disorders for diagnosis and follow-up of headache patients at the out-patient clinic. All figures are numbers (%).

Seventy-one percent (n = 102) used MRI in ≥ 2/3 consultations with patients referred with new-onset (non-acute) headache, and 73% (n = 104) requested an MRI for all long-lasting headaches referred to neurological outpatient clinics. Significantly more female than male residents used MRI for all new-onset (non-acute) headache (p = 0.025).
The ICHD was used regularly (i.e. in ≥ 2/3 consultations) by 50% (n = 71), with no significant difference between women and men (49% vs. 51%, p = 0.8) or early versus late residency (47% vs. 55%, p = 0.3). The national treatment guidelines for headache were used in ≥ 67% of consultations by 90% of participants (n = 127), with no significant gender difference (women 86% vs. men 93%, p = 0.2).
Figure 1(a)–(c) shows the proportion of respondents who would treat patients with CTTH, episodic migraine (migraine attack once every 1–2 months), and very frequent migraine (1–2 migraine attacks every week) with acute headache medication, prophylactic headache medication, and physical therapy, respectively. Simple analgesics were the most commonly suggested acute medications for CTTH (84%), and only three residents suggested opioids as an acute treatment for CTTH. Among the 72% (103/143) that suggested prophylactic medication for CTTH, amitriptyline was the most common, suggested by almost 90% (91/103). Triptans (87%), ibuprofen/NSAIDs/acetylsalicylic acid (62%), and paracetamol (37%) were all commonly suggested for the acute treatment of episodic migraine. Only 10 residents (7%) suggested anti-emetics as part of this acute treatment. Beta-blockers (69%), followed by candesartan (46%), and topiramate (25%) were the three most commonly suggested prophylactic medications for people with migraine.
Percentage of respondents who would (white bars) or would not (black bars) use different types of treatments for patients with (a) chronic tension-type headache, (b) episodic migraine, and (c) very frequent migraine.
Eighty-eight percent (n = 126) of residents reported MOH as a clinical challenge in their daily headache practice. Knowledge of which medications may lead to MOH is reported in Figure 2. Forty percent answered all questions correctly, but almost 1/3 wrongly stated that the most commonly used headache prophylactics (23% for anti-hypertensives, 26% for anti-epileptics, and 28% for antidepressant drugs) could lead to MOH. Furthermore, 15% wrongly stated that highly potent opioids, and 13% that triptans, cannot lead to MOH.
Percentage of the participants who stated that each of the given medications can lead to medication-overuse headache. Green bars represent those medications that are known to cause medication-overuse headache, while red bars represent those that do not.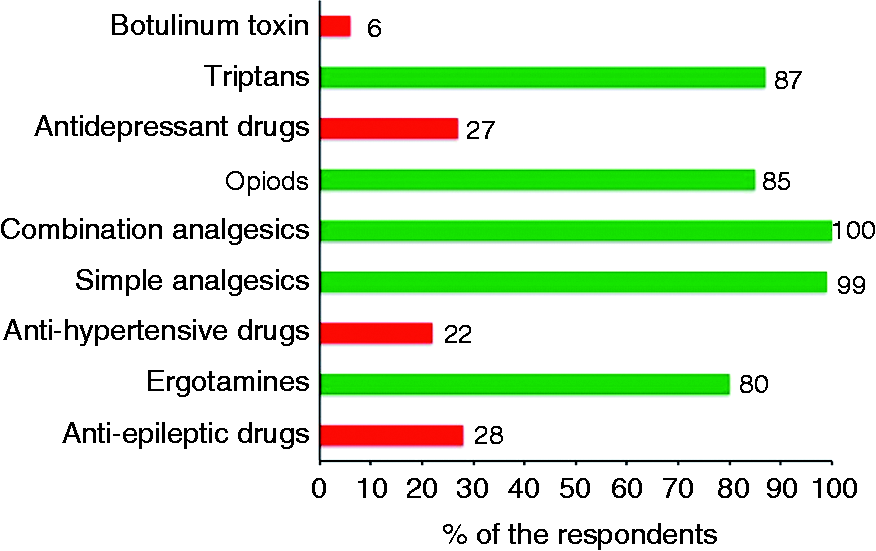
Ninety-eight percent (n = 140) used withdrawal as part of their treatment of MOH. Fifty-nine percent (n = 84) recommended initial withdrawal only, whereas 39% (n = 56) of residents used withdrawal combined with initial prophylactic medication. Nine percent (n = 13) used prednisone and 7% (n = 10) recommended rescue medication as a part of the withdrawal strategy. Furthermore, approximately 40% recommended in-patient withdrawal for patients with MOH.
Figure 3 shows that few residents felt they had good general knowledge about cluster headache, trigeminal autonomic cephalalgias and MOH, whereas 1/3 reported good knowledge about migraine.
Percentage of the participants responding good (green), medium (yellow), or poor (red) to the question “How do you rate your own knowledge of migraine, tension-type headache, cluster headache/trigeminal autonomic cephalalgias, and medication-overuse headache?”.
Thirty-seven percent (n = 51) of participants responded that they asked patients about disability, social functioning, and sick leave in every consultation, and an additional 27% (n = 37) asked about these factors in ≥ 2/3 consultations. Only 13% (n = 18) asked these questions in 1/3 of consultations or fewer.
Thirty-three percent (n = 47) of respondents scored “lack of opportunity for follow-up appointments at the outpatient clinic” as the main barrier to more optimised treatment of headache patients, with a mean score of 2.8 (where 1 was the most important and 7 the least important barrier) (Figure 4). Finding “headache patients difficult and demanding” and having “too little knowledge of headache medicine” were the next two most important barriers. However, only 14% (n = 19) regarded their own insufficient knowledge to be the most important barrier. “Lack of supervision from senior neurologists” was among the barriers given lowest importance. Gender and years of residency influenced the ranking of certain barriers. “Lack of opportunity for follow-up appointments” was seen as the most important barrier by both men and women, but with women seeing it as even more important than men did (mean score 2.4 vs. 3.5, p < 0.001). Men scored “no effective treatment options for headache patients” as a more important barrier than women did (mean score 3.1 vs. 4.1, p = 0.005) and, on average, they scored this as the second most important barrier. The more experienced residents ( > 2.5 years neurology training) ranked “lack of opportunity for follow-up appointments” and “lack of a multidisciplinary team” as more important than less-experienced residents did (mean score 2.4 vs. 3.1 and 3.7 vs. 4.5, p < 0.01).
Residents’ ranking of main barriers to optimised treatment and management of headache patients, scored on a scale of 1–7. Lower values indicate more important barriers.
Electronic dialogue/direct messages (within the electronic patient record) between neurologists and GPs was suggested by 36% of respondents as a key element for even better future collaboration concerning headache patients.
Multivariate logistic regression analysis.

Ninety-two percent (n = 132) of the respondents thought that a three-day headache course should be mandatory in order to become a certified specialist in neurology, with no differences between gender, years in neurology training, those who had attended a previous course, or those who reported lack of knowledge as a treatment barrier. Headache as a subspecialty had low prestige among residents in neurology, with a mean score of 4.7 (SD 1.2) and median of 5 ranked on a 1–6 scale where 1 indicated the highest prestige. Headache was not more prestigious among those who had attended the headache course than among those who had not (mean score 4.6 vs. 4.8, p = 0.3).
Discussion
The main finding in this questionnaire-based study among neurology residents in Norway was that there was a generally poor knowledge of headache medicine, relative to what must be considered minimum basic knowledge. We would have expected more residents to know about the epidemiology of headache and what kind of medications may lead to MOH. The results also showed large variations in the management of headaches among participants. The findings suggest that there is an unmet need for better headache education as part of neurology training. Although 12–16% of the adult population has migraine and 3–4% has chronic headache (10), there is limited focus on headache in medical schools both in Norway and throughout the world. A WHO report found that just 4 hours of undergraduate training (in the course of 4–6 years in medical school) are dedicated to headache (4). The same report suggested that lack of headache education may lead to ineffective management, and that better education may improve outcomes and lower overall costs (4). Residency is a fundamental step on the path to becoming a neurologist, but little formal, systematic, or continuous education is given on headache disorders (5,11). A cross-sectional study from the U.S. revealed that only 26% of neurology training programs for residents featured mandatory outpatient headache clinic experience (12). With little exposure to headache medicine through medical schools and residency, it may not be surprising that two studies reported that only 3.7% (Europe) and 8.3% (U.S.) of neurology residents plan to go into the headache field (13,14). Furthermore, headache has a low perceived prestige compared to other neurological disorders such as stroke, multiple scleroses, and epilepsy (9).
The European training requirements for neurology recommended by the European Union of Medical Specialities include four levels of applied clinical knowledge and skills (15). For the headache subspecialty, levels 3 and 4 are recommended in the initial (within the first 2 years) and advanced training phase (the remaining years), respectively. Level 4 applies to specific and broad knowledge and the ability to make a complete diagnosis and to treat as well as is possible. Thus, expectations for the knowledge of headache management among specialists in neurology are high, in contrast to the lack of attention given to the subject during clinical training and practice.
Between 40 and 50% of respondents did not know the approximate prevalence of migraine and chronic headaches and their co-morbidities. While prevalence estimates may not be of direct clinical use, it is likely that this indicates a more general lack of headache knowledge. It should be noted that the co-occurrence of anxiety and depression in migraine varies from 4–50% in different studies and settings, so there are no precise answers to questions on these two factors (16,17).
Headache diaries, which are recommended for diagnosis and follow-up, were used regularly by most participants. However, only 1/3 reported that their patients regularly returned the headache diary to their physician. This finding is in accordance with our clinical experience.
Imaging in headache is a controversial issue as most intracranial findings are incidental (18). Therefore, most physicians agree that only patients with unusual presentations or red flag symptoms should be referred to imaging (19,20). However, several studies have shown that neuroimaging is often routinely ordered, including for patients where guidelines specifically recommend against it (21,22). In the present study, 3/4 used MRI for all long-lasting headaches and all new headaches referred to the outpatient clinic. This is clearly a greater use of imaging than is recommended, and may, in addition to its economic ramifications, lead to unnecessary worry and the follow-up of incidental findings. In one other study, neurologist visits, when compared to GP visits, were associated with an increased chance of imaging (OR 1.7, 95% CI 0.99–2.9) (21). Why female physicians refer patients to imaging more often is unknown, but this finding is consistent with that of another study (23).
Knowledge of which medications may lead to MOH was modest, with only 40% answering every question correctly. As with primary care physicians in the US, many residents did not know that opioids may lead to MOH (24). Perhaps even more worryingly, one-third wrongly stated that the most commonly used headache prophylactics could lead to MOH. This misunderstanding can lead directly to the poor management of headache patients and may be one explanation for why so few headache patients use prophylactics (8,25). In accordance with guidelines, almost all the respondents used withdrawal therapy in MOH (26,27).
As no diagnostic test has been developed for headaches, and diagnoses are purely based on good history taking and clinical examination, the ICHD is essential for all physicians treating headache (28). The classification is easily accessible and free of charge. Thus, it may be surprising that only half of the residents used the diagnostic criteria of the ICHD regularly (9). We do not know how a diagnosis was reached for the other half of patients. Due to the increasing role of health registries in research, as well as their use as the basis for decision-making in health policies, an accurate diagnosis is essential. However, other studies have shown that many physicians do not use diagnostic classifications as they find them impractical for use in daily practice (29,30).
There is an international trend towards shorter consultations and less time for follow-ups. More than 1/3 of residents scored “lack of opportunity for follow-up appointments at the outpatient clinic” as the main barrier to more optimised treatment of headache patients. This may reflect the fact that many headache disorders are chronic conditions with a need for continuous follow-up. In addition to suboptimal management for the patients, lack of necessary follow-up appointments can lead to doctors feeling incapable of doing their job, that their work lacks meaning, and that opportunities for professional development are few. These factors have been associated with an increased risk of detachment, reduced career satisfaction, and an increased risk of burnout among residents in neurology in both Europe and the US (31–33).
Our results showed that many residents found headache patients difficult and demanding. This may be related to the low status and the stigma assigned to many chronic pain patients. Hopefully, with the emerging improvements in the understanding and treatment of headache disorders, this will change (34).
Although the literature reports better outcomes with a multidisciplinary approach for many difficult-to-treat patients (35), no headache clinics in Norway had a structured multidisciplinary approach at the time of this survey. The lack of multidisciplinary treatment as a treatment barrier became more evident among the more experienced residents.
So, what can be done to increase the prestige, knowledge, and experience of headache medicine during neurology residency? As many as 92% in the present study believed that an existent three-day headache course arranged by the Norwegian Advisory Unit on Headache should be made mandatory in order to become a certified specialist in neurology. Three days may seem rather brief, but it is still much better than the current requirements in Norway. Such courses will expose all residents to the basics of headache medicine, but they should also aim to become an important recruitment area for future headache researchers. A study among the New Investigators and Trainees Section (NITS) members of the American Headache Society highlighted mentorship and exposure to a headache centre as key factors in becoming interested in headache medicine (7). Medical students and residents should be invited into headache research early in their careers. Increased availability of headache courses, educational webpages, opportunities to participate in the larger general neurology societies, and juniors teaching congresses (e.g. Headache Summer School and International Headache Academy) may help to recruit more physicians into headache medicine. Furthermore, it is important that all physicians working with and teaching headache medicine to students and residents encourage them to enter into this field. Political awareness is also needed to spread the knowledge that headache is the most common neurological disorder, and that it is associated with a high degree of morbidity in the young and middle aged, leading to sick leave and inability to work. These issues must be reflected in the curriculum at medical schools and during residency in the future.
Methodological considerations
The high responder rate among departments (100%) and residents (86%) in neurology in Norway should ensure good representativity. Moreover, 50% of all residents in Norway are educated abroad, most commonly in European countries (mainly Denmark, Germany, the UK, Sweden, Hungary, Poland, and the Czech Republic), and our results may, to a certain extent, reflect the status in Europe more generally. Further studies among residents and research fellows worldwide are warranted and may give new and broader insight into these subjects. Furthermore, such surveys should be repeated to evaluate time trends and whether specific educational or administrative interventions affect the residents’ knowledge. Questions about red flags and their relation to the use of imagining could also be of interest.
Questionnaire studies such as this may introduce recall bias. However, there is no reason to suspect systematic bias.
In conclusion, headache knowledge among residents in Norway is moderate at best. Headache is one of the most frequent reasons for referral to neurologists, and we believe that a better knowledge level is needed. Headache medicine should therefore be a mandatory part of neurology training worldwide.
Clinical implications
Although a major public health problem, headache knowledge among residents is moderate at best. The vast majority of residents believed that a headache course should be mandatory in order to become a certified specialist in neurology. Headache had a low status among residents in neurology.
Supplemental Material
Supplemental material for Neurology residents’ knowledge of the management of headache
Supplemental Material for Neurology residents’ knowledge of the management of headache by Espen Saxhaug Kristoffersen, Kashif Waqar Faiz and Bendik Slagsvold Winsvold in Cephalalgia
Footnotes
Acknowledgments
The authors want to express their sincere gratitude to the participating residents and hospitals; without them the study would not have been possible. And thank you to Marte Helene Bjørk, Hilde Karen Ofte, Åslaug Rudjord Lorentzen, Espen Finnesand, Nikola Braatan, Guttrom Eldøen, Kaja Nyquist, Elin Dahl, Mette Bergum, Tore Wergeland, Kai Ivar Müller, Gro Owren Nygaard, Axel Meyer Simonsen, Håkon Sætre, Sanpreet Kaur Grewal, Brit Andenes Blauuw and the research administration at Akershus University Hospital for their logistical assistance.
Authors’ contributions
ESK had the original idea for the study and planned the overall design with KWF and BSW. ESK prepared the initial draft and was the main author of the present manuscript. All authors planned the statistics methodology and were involved in all analyses. All authors have read, revised, and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by grants from the University of Oslo, Akershus University Hospital, and Oslo University Hospital. The funding sources had no role in the design of the study, the collection, analysis, and interpretation of the data, preparation of the manuscript, or the decision to submit the manuscript for publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.