
Abstract
Background or aim
Despite guidelines and the International Classification of Headache Disorders (ICHD-III beta) criteria, the diagnosis of common chronic headache disorders can be challenging for non-expert clinicians. The aim of the review was to identify headache classification tools that could be used by a non-expert clinician to classify common chronic disorders in primary care.
Methods
We conducted a systematic literature review of studies validating diagnostic and classification headache tools published between Jan 1988 and June 2016 from key databases: MEDLINE, ASSIA, Embase, Web of Knowledge and PsycINFO. Quality assessment was assessed using items of the Quality of Diagnostic Accuracy Studies (QUADAS-2).
Results
The search identified 38 papers reporting the validation of 30 tools designed to diagnose, classify or screen for headache disorders; nine for multiple headache types, and 21 for one headache type only. We did not identify a tool validated in a primary care that can be used by a non-expert clinician to classify common chronic headache disorders and screen for primary headaches other than migraine and tension-type headache in primary care.
Conclusions
Despite the availability of many headache classification tools we propose the need for a tool that could support primary care clinicians in diagnosing and managing chronic headache disorders within primary care, and allow more targeted referral to headache specialists.
Introduction
Around 4% of primary care consultations and 30% of neurology outpatient appointments in the UK are due to headache disorders (1,2).
Yet many patients presenting in primary care with headache do not have a formal diagnosis, are misdiagnosed, and can potentially receive inappropriate drug treatment and management (3). A study in the UK found 70% presenting with new onset headache were not formally diagnosed (3) and 88% of patients with a history of sinus headache screened in primary care clinics in the US met International Headache Society criteria for migraine (4).
Despite deceptively simple diagnostic criteria for different headache types such as the comprehensive headache classification of the International Classification of Headache Disorders, 3rd edition (5) and the National Institute for Health and Care Excellence (NICE) headache guidance (6); in reality, it can be challenging for a non-expert clinician to accurately diagnose headache disorders.
The Chronic Headache and Self-management Study (CHESS) is a National Institute for Health Research (NIHR) grant-funded programme (project number RP-PG-1212-20018) with the overall aim of developing and testing a self-management programme for people living with chronic headache. As part of the study we want to be able to classify participant's chronic headache types both for reporting purposes, and as part of the study intervention to allow targeted treatment and advice. Specifically, we need a classification tool that can be used by a non-expert clinician to screen for primary headache disorders other than migraine and tension type headache (TTH), distinguish between chronic migraine and chronic TTH and identify medication overuse headache (MOH) in primary care settings. We anticipate that such a tool could also support primary care clinicians in diagnosing and managing chronic headache disorders within primary care, and allow more targeted referral to headache specialists.
We therefore conducted this systematic review to a) identify any existing tools used to classify chronic headache disorders and b) assess the validation of tools identified.
Methods
We registered this review prospectively with the International Prospective Register of Systematic Reviews. PROSPERO 2015: CRD42015019863 (7) and we followed the PRISMA guidelines for the reporting of systematic reviews (8).
Search strategy and study selection
We included studies that describe the validation of headache tools intended to diagnose, classify or screen for one or more headache types and compare with a reference standard. We only included studies published in English and published from January 1988, the publication date of the first International Classification of Headache Disorders (ICHD) (5). We excluded studies with participants aged below 18 years and any dissertation and conference proceedings, plus those studies where the sole purpose of the study was to report the validation of a tool in a different language.
With the support of an academic support librarian, we searched key databases: MEDLINE, ASSIA, Embase, Web of Knowledge and PsycINFO. The searches were updated in June 2016. We used free text and MeSH terms based on those used for NICE headache guidelines 2012 (9); search words included: ‘Headache’, ‘headache disorders’, ‘headache disorders primary’, ‘headache disorders secondary’, ‘migraine’, ‘migraine disorders’, ‘migraine with aura’, ‘migraine without aura’, ‘tension headache’, ‘cluster headache’, ‘medication overuse headaches’ combined with ‘classification’, ‘diagnostic’, ‘diagnosis’, ‘diagnostic techniques and procedures’, ‘sensitivity’, specificity’, ‘efficacy’, ‘effectiveness’, ‘efficiency’, ‘predictive value of tests’, ‘likelihood function’, ‘diagnostic odds ratio’, and ‘screening,’ ‘questionnaire,’ ‘survey’, ‘interview as topic’ and ‘tools’, ‘instruments’ and ‘ICHD’.
Results were managed using the Evidence for Policy and Practice Information and Co-ordinating Centre (EPPI Centre) reviewer 4 software, duplicates removed, and titles checked for relevance by two authors (RP, KP). We sought a full copy of possible relevant papers, which were assessed independently for inclusion by two authors and any disagreement resolved by discussion. We checked reference lists of relevant papers for any additional studies.
Data extraction and quality assessment
Three authors (RP, CB, KP) independently extracted data from papers included in the review using a predetermined pro-forma to capture both study and tool-specific information: Study design, characteristics of study participants, a brief description of the diagnostic or classification tool, test characteristics, diagnostic/classification parameters, validation assessment (sensitivity, specificity), how the tool is used (questionnaire, online, interview) and by whom (expert, non-expert, patient).
The same three authors independently assessed the methodological quality of each study using the Quality of Diagnostic Accuracy Studies (QUADAS-2), a validated tool used for the quality assessment of diagnostic accuracy studies (10).
The QUADAS-2 assesses four domains for risk of bias: Patient selection (sampling and exclusions), index test (conduct and interpretation), reference standard (conduct and interpretation), and flow and timing (interval between index and reference standard, number receiving reference standard and included in the analysis). The sets of signalling questions used for each domain have been tailored to the content of the review as recommended by the authors of the tool.
We assessed risk of bias as low, high or unclear for each domain and calculated an overall risk of bias dependent on the number of domains judged as high risk of bias: 0 domains = low, 1 = low/medium, 2 = medium, 3 = medium/high, 4 = high risk of bias. Where criteria used to judge risk for one of the domains was unclear, the risk was considered “high” and this was denoted in the overall risk of bias.
Results
Study selection
We identified 4348 records from the combined database searches and removed 2459 duplicates. The remaining 1889 records were screened for relevance and 1694 records were excluded because they did not meet the study inclusion criteria. We obtained the full text for 195 records and excluded 157 after reading the full papers, which did not meet the inclusion criteria, resulting in a total of 38 papers included in the review (Figure 1).
PRISMA flow chart of article selection.
Study characteristics
Characteristics of included studies .

ICHD: International Classification of Headache Disorders; TTH: tension type headache; NDPH: new daily persistent headache; MOH: medication overuse headache; CDH: chronic daily headache; TAC: trigeminal autonomic cephalalgia; CH: chronic headache; MA: migraine with aura; MO: migraine without aura.
The number of participants included in the validation studies ranges from 50 to 9346. The majority of the tools are questionnaires, self-completed (n = 17), completed face-to-face with a clinician or researcher (n = 8), and self-completed online questionnaires (n = 2). The three remaining tools are computerised decision support systems designed to assist clinical diagnosis. The number of items in the questionnaires range from short single item migraine screen tests (48) to a longer 76-item questionnaire (11) plus the complex computerised diagnostic tools (14,15,35).
The tools have been validated in headache clinic settings (n = 14) as part of general health or household surveys (n = 6), neurology clinics or departments (n = 5), primary care settings (n = 4), emergency care (n = 3), community (n = 2) and other settings such as ophthalmology departments, temporomandibular joint and orofacial pain clinics, and obstetrics and gynaecology clinics (n = 3), with some tools validated in more than one setting.
In most studies the reference standard used to validate the tool is a face-to-face neurological assessment by a headache specialist doctor based on the ICHD criteria used at the time of validation. Exceptions include where the reference standard is conducted by a headache nurse specialist experienced in headache diagnosis (35), primary care doctors trained to use IHS criteria for migraine (31) and researchers (48). When reported, the time interval between the index test and reference standard is generally short (conducted on the same day, or within four weeks) although the longest interval reported was between two to three years (28).
There is wide variation in the reporting of the psychometric results across studies, with some reporting an overall sensitivity and/or specificity only, others reporting results for particular headache types, and with some studies also reporting positive and negative predictive values. We have reported the psychometric results for each study in Table 1.
Study quality
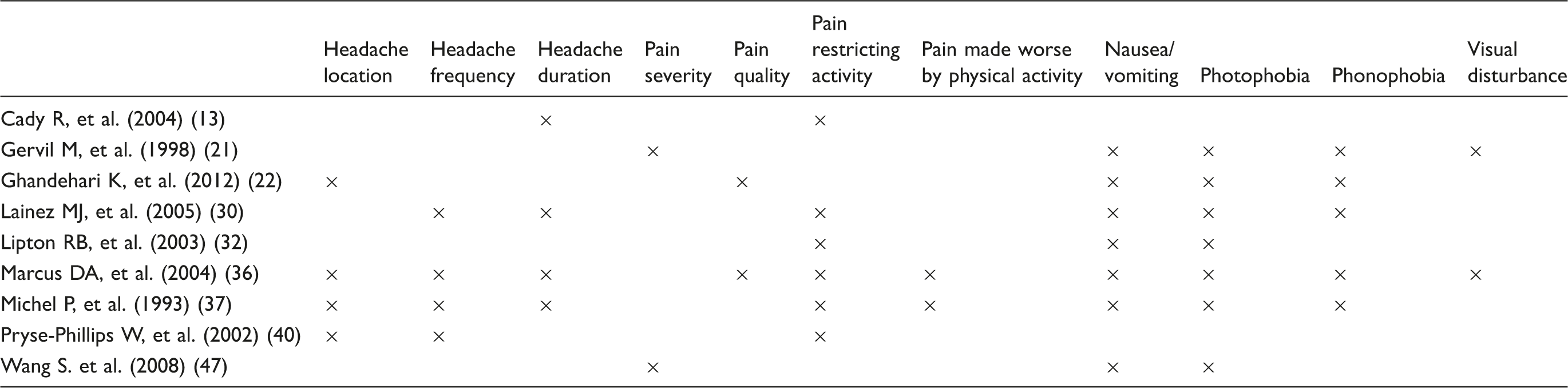
Common questions across migraine screening tools .
Multiple headache types
We identified nine tools that diagnose or classify more than one headache type, three computerised decision support tools, and six questionnaires. The three computerised diagnostic tools support clinical diagnosis of the common episodic and chronic primary headache disorders migraine and TTH, trigeminal autonomic cephalalgia (TAC) and medication overuse headache (MOH) (14,15,35). The sensitivity of the computerised decision support tools appears to be good for most headache types, the authors report lower sensitivity for probable migraine and probable TTH (15) and new daily persistent headache (NDPH) (35). All three tools have been validated in headache clinic populations; overall risk of bias is lowest for the study by Dong et al. (2014) (15).
The six questionnaires all classify the common primary headache disorders, migraine and TTH, plus MOH. The 76-item Italian ICHD-II based questionnaire reports the highest sensitivity and specificity and has low risk of bias (11). The HARDSHIP questionnaire, developed as part of a Global Campaign against Headache initiative, has been the most extensively validated, in different languages and cultures, and is suitable to be administered by trained lay interviewers; examples of studies using the questionnaire are presented in Table 1. Sensitivity ranges from 63–85 and specificity 82–99 for migraine, and sensitivity 51–64 and specificity 51–64 for TTH across the four studies (India, China, Russia and Pakistan) (49).
In addition to the common primary headache disorders, migraine and TTH, one self-completed questionnaire also screens for trigeminal autonomic cephalalgia (20), validated in a headache clinic population; authors report sensitivity 63.3 (52.9–72.7) and specificity 98.8 (96–99.8).
One headache type
Cluster headache
We identified two tools that screen for cluster headache, both self-completed questionnaires validated in headache clinic populations with low/medium risk of bias (17,46). The presence of five of seven features (pain severity and location, duration < 3 to 4 hours, frequency and daily reoccurrence of attacks, rhinorrhoea and restlessness) has high sensitivity, 100, and specificity of 95.1 (46).
Probable medication overuse headache
We found one tool for the screening of probable medication overuse headache (pMOH) (16), validated in a headache clinic setting with low/medium risk of bias. Based on ICHD-II criteria for pMOH, three items were found to have sensitivity of 81 and specificity of 100.
Migraine
We identified 18 tools designed to classify or screen for migraine: Migraine only (n = 10), migraine with and without aura (n = 5), aura only (n = 1), chronic migraine (n = 1) and menstrual migraine (n = 1).
Methodological quality of studies using an adapted version of QUADAS-2 .
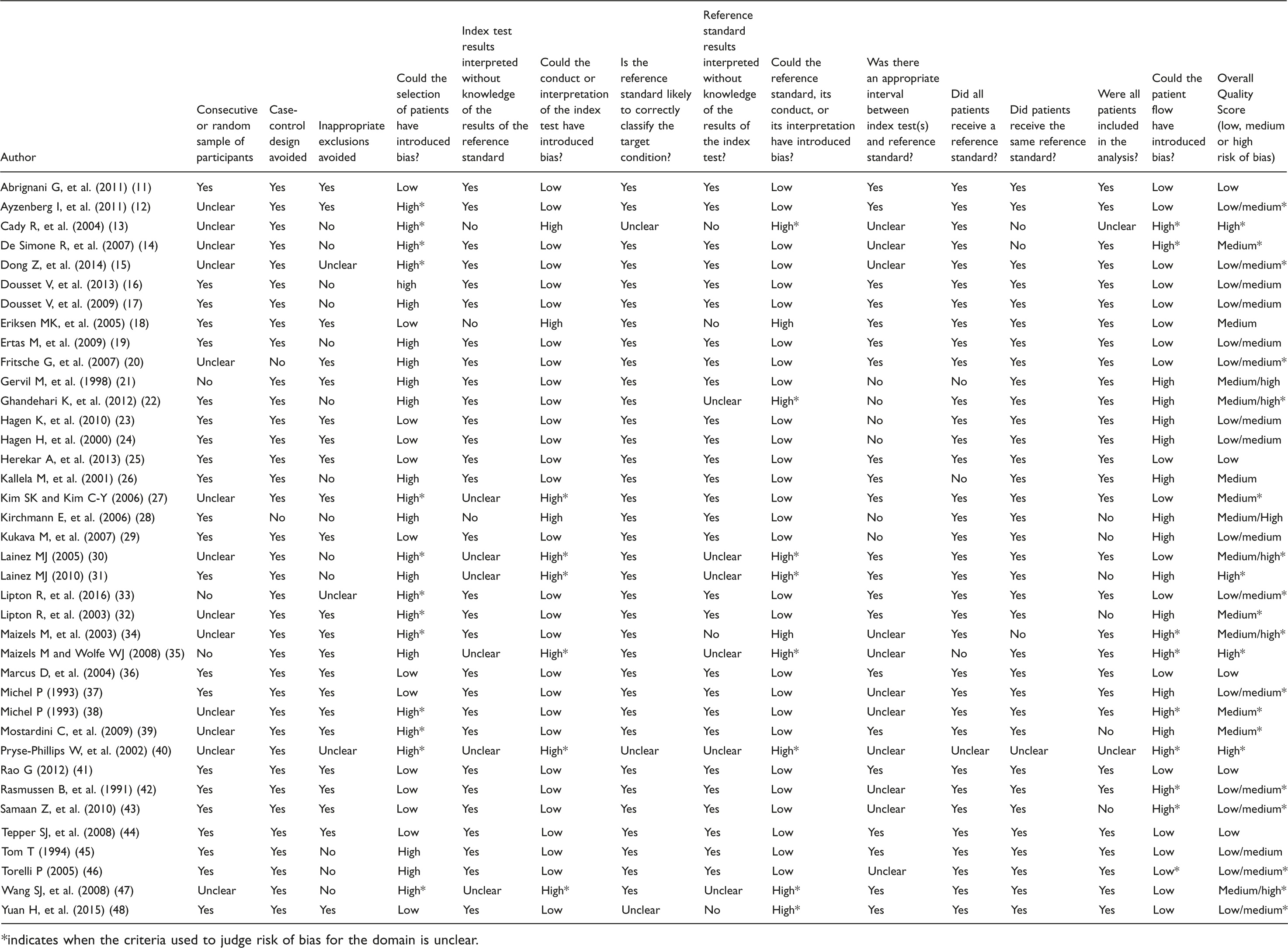
*indicates when the criteria used to judge risk of bias for the domain is unclear.
The most widely used and validated of the migraine tools is the ID Migraine, with three questions on headache-related disability, nausea and photophobia (32). A previous meta-analysis of 13 studies reports sensitivity of 84 (95% CI, 75–90) and specificity of 76 (95% CI 69–83) (50). ID Migraine has been validated in different languages (not reported here) and different settings, including ENT and ophthalmology, and temporomandibular joint and orofacial pain clinics. (19,27).
The seven item Asian Migraine Criteria (AMC) reports the highest sensitivity and specificity (99.3 and 84.4), but medium/high* risk of bias (22). The eight item Migraine Assessment Tool (MAT) reports good sensitivity and specificity (89 and 79) and low risk of bias.
Not surprisingly, the tools developed to identify migraine with or without aura, all self-completed questionnaires, tend to be longer, ranging from 10 questions to 56 questions. The shortest of these, the University of California-San Diego (UCSD) Migraine Questionnaire (45) reports sensitivity and specificity for migraine with aura (71–81 and 100), migraine without aura (100 and 91–94) with low/medium risk of bias. A longer questionnaire where participants are asked to describe aura in their own words (26) reports higher sensitivity and specificity for migraine without aura (93–100 and 100) and migraine with aura (88–89 and 95–97) but has medium risk of bias (26).
The Visual Aura Rating Scale (VARS) (18) is intended to supplement the ICHD-II and captures visual aura symptoms and characteristics (e.g. location, scotoma, ziz-zag lines, duration, and gradual development). Validated in a population already diagnosed with migraine with aura, sensitivity and specificity are high (91 and 96) and methodological quality, medium* risk of bias.
Identify Chronic Migraine (ID-CM) (51) is an online tool to help clinicians identify patients likely to have migraine and, in particular, chronic migraine. The authors report sensitivity and specificity for migraine (83.5 and 88.5) and for chronic migraine (80.6 and 88.6); risk of bias is low/medium.
Discussion
The review identified many papers validating headache diagnostic classification tools. The large number of tools identified indicates the demand for tools that can be used to support the diagnosis of headache disorders clinically and/or allow the classification of headache disorders in research.
More than half of the papers (n = 21) were judged to have low or low/medium risk of bias for overall quality. The risk of bias was judged high most frequently for the QUADAS-2 domain “flow and timing”, which assesses the interval between collecting the index and reference standard, the number of participants receiving the same reference standard, and whether all participants were included in the analysis. The criterion used to judge the risk of bias was unclear for at least one domain in 23 papers and recorded as “high risk”, indicating that quality assessment often reflects bias in reporting rather than bias in the conduct of the study. Most of the tools identified in the review have been tested in one setting only, predominantly in headache clinic populations. Exceptions include the Hardship tool, which has been validated in different languages and cultures, and the ID-migraine, which has been validated extensively in different languages and settings.
The overriding purpose of the review was driven by our own research requirements; that is, to identify existing headache classification tools that can be used by a non-expert clinician in primary care to classify chronic headache disorders, and specifically to identify tools that allow the user to screen for primary headache disorders other than migraine and TTH, distinguish between chronic migraine and chronic TTH and identify MOH. We anticipated that such a tool could also support primary care clinicians in diagnosing and managing chronic headache disorders within primary care more effectively.
We identified six tools that allow the user to screen for primary headache disorders other than migraine and TTH; four to identify trigeminal autonomic cephalalgias (TACs) and two specifically for cluster headache. The three computerised diagnostic tools appear to perform well for identification of TACs, as does the longer of the cluster headache-specific questionnaires (46). Only one of the computerised diagnostic tools was designed and validated for use by a non-expert clinician, but to date has not been validated in primary care (15).
The HARDSHIP questionnaire is the most extensively validated of the tools that allows the distinction between chronic migraine and chronic TTH by a non-expert clinician; the questionnaire was not designed to identify other primary headache types. The Identify Chronic Migraine (ID-CM) tool helps clinicians to identify patients likely to have migraine and, in particular, chronic migraine, but does not allow the classification of other chronic headache types. More commonly, the tools identified in the review classify episodic rather than chronic headache, with 17 screening for episodic migraine. It is interesting to note that, where authors have published the tool, no question is common to all tools.
The review also identified a number of tools that classify medication overuse headache including a brief self-complete questionnaire adapted from ICHD-II for MOH with sensitivity of 81 and specificity of 100 (16).
We identified a large number of good quality studies, validating a wide range of different headache classification tools; the review provides a comprehensive evaluation and summary of tools that researchers and clinicians can use to classify headache disorders. However, we did not identify a tool that fully met our own research needs that has been validated in a primary care setting and could be used by a non-expert clinician in primary care to support the diagnosis of common chronic headache disorders and screen for primary headache disorders other than migraine and TTH. We propose that such a tool could potentially support more targeted referral to headache specialists and free up under-resourced neurology departments (1).
Strengths
We searched for tools that diagnose, classify or screen for all headache types rather than restrict the search to tools for chronic headache only.
All data extractions and quality assessments were double coded independently by three reviewers and agreement checked; we used the established tool QUADAS-2 to assess the quality of studies.
Limitations
Our search strategy used MeSH terms based on the search terms used to develop NICE headache guidelines to identify potential validation studies, but it is possible that some studies were missed. Reporting of psychometric results made it difficult to compare across studies.
Conclusions
Diagnosis of chronic headache disorders can be challenging for non-expert clinicians. Depending on the clinical or research need, there are a number of adequate tools available that could be used in specific contexts. Nevertheless, there are currently no tools validated in primary care that can be used by non-expert clinicians to classify chronic headache disorders that also allow the user to screen for primary headaches other than migraine and TTH. The availability of such a tool could support primary care clinicians in diagnosing and managing chronic headache disorders within primary care, and allow more targeted referral to headache specialists.
Footnotes
Key findings
The review identified 30 tools designed to diagnose, classify or screen for headache disorders, nine for multiple headache types, and 21 for one headache type only.
Depending on the clinical or research need, there are a number of adequate tools available that could be used in specific contexts.
There are currently no tools validated in primary care that can be used by non-expert clinicians to classify chronic headache disorders that also allow the user to screen for primary headaches other than migraine and TTH.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the NIHR Programme Grants for Applied Research programme (RP‐PG‐1212‐20018). The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Note
*indicates when the criteria used to judge risk of bias for the domain was unclear.