
Abstract
Introduction
ICHD-3 criteria for chronic migraine (CM) include a mixture of migraine and tension-type-like headaches and do not account for patients who have a high frequency of migraine but no other headaches.
Materials and methods
Patients from the Danish Headache Center and their relatives with ICHD-3 defined CM were compared with patients with high frequency episodic migraine (HFEM). Danish registries were used to compare the socioeconomic impact in these two groups. A Russian student population was used to determine the generalizability of the number of patients fulfilling CM and the proposed diagnostic criteria for CM.
Results
There was no difference in the demographic profile between the two groups in the Danish cohort. The number of lifelong or annual attacks (p > 0.3), comorbid diseases, or self-reported effect of triptans (p = 1) did not differ. HFEM patients purchased more triptans than CM patients (p = 0.01). CM patients received more early pension (p = 0.00135) but did not differ from HFEM patients with regard to sickness benefit (p = 0.207), cash assistance (p = 0.139), or rehabilitation benefit (p = 1).
Discussion
Patients with HFEM are comparable to CM patients with regard to chronicity and disability. We therefore suggest classifying CM as ≥ 8 migraine days per month (proposed CM), disregarding the need for ≥ 15 headache days per month. The proposed diagnostic criteria for CM approximately doubled the number of patients with CM in both the Danish and the Russian materials. Extending the definition of CM to include patients with HFEM will ensure that patients with significant disease burden and unmet treatment needs are identified and provided appropriate access to the range of treatment options and resources available to those with CM.
Conclusion
Patients with migraine on eight or more days but not 15 days with headache a month are as disabled as patients with ICHD-3 defined CM. They should be included in revised diagnostic criteria for chronic migraine.
Keywords
Introduction
Chronic migraine (CM) was distinguished from episodic migraine in the second edition of the International Classification of Headache Disorders (ICHD) (1). However, field testing revealed that the ICHD-2 criteria for CM were too restrictive for clinical practice as well as clinical trials because they excluded the patients who would constitute the intended target population for new treatments. As a result, the ICHD-2 criteria for CM were revised in 2006 (ICHD-2R), requiring that patients have 15 or more headache days per month with at least 8 days of headache that meet criteria for migraine without aura or that respond to migraine-specific therapy (2). According to the ICHD-2R criteria, CM was classified as a complication of migraine. The diagnosis could not be made in the setting of medication overuse and only days of migraine without aura contributed to the requisite number of migraine days. To address these limitations, in 2013, revised criteria (ICHD-3 beta) removed CM as a complication of migraine, migraine with aura was included among the 8 days minimum of migraine required per month, and simultaneous diagnoses of CM and medication overuse were permitted (3). These criteria remained in the recently published ICHD-3 (4). It has proven valuable to specifically identify this severely affected population of individuals with migraine as it has facilitated epidemiological studies that identified the significant burden of illness, comorbid diseases, and cost of illness compared to episodic migraine. It has also propelled the conduct of clinical trials of established and novel treatments and ultimately regulatory approval of treatments for a patient population that had previously been systematically excluded from therapeutic trials.
Despite these advances, there remains a number of weaknesses with the current diagnostic criteria for CM. First, the criteria are complex and few physicians, even neurologists, actually apply them correctly (5–7). Second, the diagnostic criteria allow for a combination of migraine and tension-type headaches (TTH). Some of these milder tension-type-like (TTL) headaches are widely believed to represent mild migraine attacks, while others may represent true tension-type headaches. Third, and perhaps most importantly, the diagnostic criteria do not account for individuals who have a high frequency of migraine, no TTH or TTL headaches, and a high level of disability. For example, a patient with 12 days of migraine per month but no TTH or TTL headache is not classified as chronic migraine but may be more severely affected than a patient with eight migraine days and 7 days of TTH or TTL headache. Finally, longitudinal studies have revealed that there is a high level of within-person variation in headache days per month (8). As a consequence, formal application of ICHD-3 criteria may result in frequent diagnostic changes.
The hypothesis of the present study was that patients with eight or more migraine days per month (with or without aura; hereafter referred to as migraine) but not 15 days with headache per month, are as disabled as patients with ICHD-3 defined CM, and therefore should be included in revised diagnostic criteria for CM. We test the hypothesis by comparing patients with chronic migraine, according to current ICHD-3 criteria, with patients with eight or more migraine days but less than 15 headache days per month (high frequency episodic migraine, HFEM) using the unique Danish registries.
Materials and methods
Study populations
The socioeconomic analyses were conducted on a dataset from the Danish Headache Center, Rigshospitalet-Glostrup, Denmark, consisting of patients and their relatives. To determine the proportions of CM and HFEM within different populations, a population-based student dataset from Yekaterinburg, Russia, was used.
Danish Headache Center
The Danish dataset consisted of 1960 adult (≥18 years of age) male and female patients from the Danish Headache Center and their relatives. Subjects were excluded if they had headaches thought to be secondary to another disorder or if they declined to or were cognitively not able to participate in the semi-structured interview; if they were of other than Danish descent; and if they were ≤ 18 years of age. Data were collected in three phases, as previously described (9–12). Each subject had a validated semi-structured interview (13,14). The interview included information about headache characteristics; aura; frequency; duration; accompanying symptoms; treatment response; precipitating and provoking factors; comorbidities; and familial occurrence. The diagnosis relied on a detailed recording of the above-mentioned symptoms using the diagnostic criteria of the ICHD-3 (4). All interviews were conducted by a neurology resident or a senior medical student specifically trained in headache diagnosis and subsequently validated by a physician, enabling high quality data.
Healthy Russian medical students
This dataset consisted of migraine patients among 1042 healthy Russian medical students. Subjects were excluded if they had a history of stroke or transient ischemic attack, intracranial hemorrhage, intracranial aneurysm, brain tumor, any operation on the brain, multiple sclerosis, epilepsy, encephalitis, meningitis, or dementia. Data collection, demographic profile, and additional information about the study population has been described elsewhere (15). Each subject received the same validated semi-structured interview as the Danish material (13,14), performed by a trained physician or a senior medical student specifically trained in headache diagnosis.
Proposed revision to the ICHD-3 diagnostic criteria for chronic migraine
Proposed diagnostic criteria for chronic migraine (pCM).

The Danish National Prescription Registry
The Danish National Prescription Registry is an individual-level prescription register that contains data on all prescription drugs sold in Danish community pharmacies since 1994 (16). The registry does not contain aggregate data on sales of over-the-counter drugs. We used data on triptans, a prescription class of acute drugs for treating migraine attacks. Triptans are prescription drugs in Denmark and are not sold over the counter. Fully anonymized data on triptans were merged at Statistics Denmark and combined with the Danish dataset.
Statistics Denmark
Statistics Denmark is a Danish governmental organization, which has created statistics on the Danish society since 1980. Statistics Denmark has an extensive collection of register data at its disposal for production of official statistics and they offer access to their data for research projects, only for researchers who are employed at authorized research institutions (17). We used data on socioeconomic variables retrieved from Statistics Denmark. Information on early retirement pension, sickness benefit, cash assistance, and rehabilitation benefit were available from the period 1980–2016. Information was available for n = 151 with CM and n = 159 patients who had at least 8 days with migraine but less than 15 days of headache (HFEM). Headache day frequency was determined from semi-structured interviews. Early retirement pension is granted to subjects who are not able to work either full time or part time, permanently. Subjects who are unable to work due to illness and have a medical certificate may qualify for sickness benefits (subjects who are not on pension). Cash assistance guarantees an income for adult subjects who are out of work and not studying, subjects must be approved for cash assistance by the authorities and cannot receive cash assistance if they have a partner who can support them or if they have a fortune. Rehabilitation is a program for adult subjects who can no longer work due to physical, psychological or social reasons. It is a program that intends to explore if subjects can maintain a job via education and training, and rehabilitation benefit is granted in conjunction with education and training. After the program, subjects are either working again or may receive, for example, early retirement pension.
Statistical analysis
Statistical analyses were performed using statistical software R version 3.3.2 and R Studio version 1.0.136. Standard deviations and t-tests were used to compare the means after checking that data were normally distributed. A non-parametric test was used for data that were not normally distributed; Wilcoxon rank sum test was used for the analysis on triptan purchases. Chi square test was used for the analysis on triptan effect and comorbidities. For single counts less than 6, Fisher's exact test was used. Logistic regression was used for the analysis on socioeconomic factors given the following variables: Current age (observation period), year of interview, and sex.
Results
Chronic migraine (CM) was defined according to ICHD-3 and high frequency episodic migraine (HFEM) as patients who had at least 8 days with migraine but less than 15 days with headache. Proposed diagnostic criteria (pCM) included both groups (Table 1).
Demographic profile of the Danish study population
Demographic characteristics of the Danish study population.

CM: Chronic migraine; HFEM: High frequency episodic migraine.
Migraine attack frequency
Migraine attack frequency.

CM: Chronic migraine; HFEM: High frequency episodic migraine.
Medication
A strong indicator of a chronic disease history is continued use of triptans. As triptans are prescription drugs, we were able to retrieve data about triptan purchases from The Danish National Prescription Registry and compared the number of triptan purchases between CM and HFEM. Figure 1 shows that HFEM patients purchased significantly more triptans than CM patients (p = 0.01).
Distribution of Triptan purchases among patients with CM vs. HFEM.
The treatment effect of triptans was, in this study, defined as a 50% reduction in symptoms within 2 hours after taking triptans. This was recorded in the semi-structured interview. The response rate in the two groups was not significantly different (p = 1, CI[0.552:1.813]).
Comorbidities
A parameter which putatively reflects the complexity of disorders is the prevalence of comorbidities. As seen in Figure 2, the prevalence of comorbidities of migraine are the same for CM and HFEM, except for epilepsy (p = 0.01) and asthma and allergy (p = 0.007).
Comorbidities among patients with CM vs. HFEM. Note: Epilepsy p = 0.01; asthma and allergy p = 0.007.
Comparison of social parameters
Social parameters 1980–2016.

CM: Chronic migraine; HFEM: High frequency episodic migraine.
Another indicator of disability is the receipt of sickness benefit more than one time. From 1980–2016, there was no significant difference between CM patients and patients with HFEM in receipt of sickness benefit. Results did not change after adjusting for age, sex, and year of interview (p = 0.207), Table 4.
Cash assistance is granted to adult subjects who cannot support themselves, and thus is an indicator of disability. From 1980–2016, there was no significant difference between CM patients and patients with HFEM in receipt of cash assistance. Results did not change after adjusting for age, sex, and year of interview (p = 0.139), Table 4.
Rehabilitation benefit is granted to subjects who can no longer work due to physical, psychological or social reasons, and thus is an indicator of disability. From 1980–2016, there was no significant difference between CM patients and patients with HFEM in receipt of rehabilitation benefit. Results did not change after adjusting for age, sex, and year of interview (p = 1) (Table 4).
The proportion of chronic migraine and high frequency episodic migraine within different populations
The proportion of CM and HFEM in different populations.
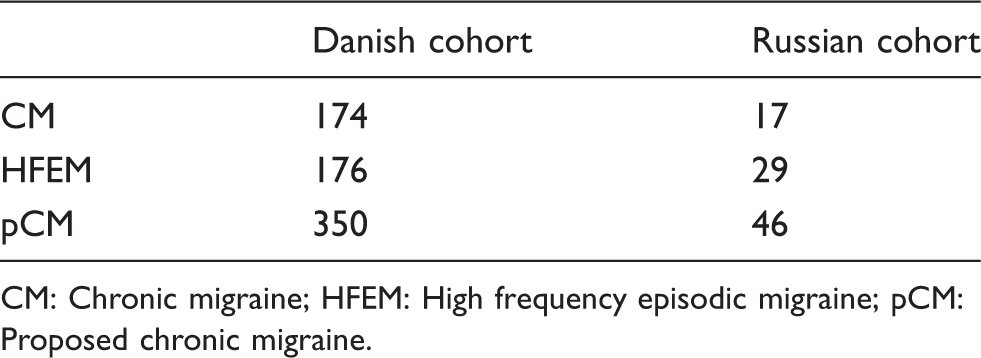
CM: Chronic migraine; HFEM: High frequency episodic migraine; pCM: Proposed chronic migraine.
Discussion
Our findings suggest that patients who have at least eight or more migraine days per month but not 15 days with headache, in this study referred to as high frequency episodic migraine (HFEM), do not differ from patients with ICHD-3 defined chronic migraine (CM) with regard to demographic characteristics, lifetime or annual migraine attack frequency, overall disease burden, or response to acute treatments. In addition, the overall prevalence of comorbid diseases was similar in both groups. Patients with HFEM purchased significantly more triptans than patients with CM (p = 0.01). Finally, we found that adding HFEM to ICHD-3 defined CM, the proposed new diagnostic criteria for CM (Table 1) doubled the number of patients with CM. These proportions were similar in the Russian population and the proportions are therefore likely to be universal.
The development of diagnostic criteria for CM over several editions of the ICHD was driven by a desire to single out the most disabled segment of migraine patients. The diagnostic criteria were gradually opened to include more patients. The purpose was, of course, to focus research and drug development on these patients to ascertain a better treatment. The present study is one more step on the way. It documents that a large segment of debilitated patients has been left out, those with HFEM. We demonstrate that they are as affected as patients diagnosed according to the present criteria for CM. Therefore, the study provides strong evidence that the diagnostic criteria for CM should include these patients. This line of thinking is in accordance with principles previously outlined by Schulte and May (18).
Our study is the first to compare patients with CM according to the current ICHD-3 criteria with HFEM. Previous studies have demonstrated that patients with CM (relative to episodic migraine) have worse socioeconomic status (19) and health-related quality of life (20), higher rate of comorbid somatic and psychiatric conditions (19), and increased health care resource utilization (6). However, the subgroup with episodic migraine in these studies included all individuals regardless of headache day frequency. The influence of sociodemographic factors was moderately, but not statistically significantly, greater in CM than in HFEM. This may be a consequence of current diagnostic criteria. For political reasons, receipt of public support requires documented chronic disability in everyday life, and chronicity is not only built into the diagnostic term chronic migraine, but patients with CM are more likely to report daily or near-daily symptoms compared to those who have HFEM. Subjects who were diagnosed as CM could therefore more easily have obtained public support benefits than subjects with HFEM.
Our study used the unique Danish registries to document that patients who have HFEM are as affected as those fulfilling CM criteria with regard to chronicity and disability. We find that adding HFEM to CM in the proposed diagnostic criteria for CM (pCM) approximately doubles the number of subjects with CM. The results are similar in a Russian student population, which generalizes the results for the number of patients who fulfill the current and proposed diagnostic criteria for CM but not the result for the social impact. Our findings suggest a much-needed simplification of the diagnostic criteria for CM that better reflects the suffering of many patients who have a high frequency of migraine but no other headache. Extending the definition of CM to include patients with HFEM will ensure that patients with significant disease burden and unmet treatment needs are identified and provided appropriate access to the range of treatment options and resources available to those with CM. This is especially important since some treatments are reserved only for those that meet current CM criteria (OnabotulinumtoxinA). Novel emerging therapies (CGRP monoclonal antibodies) may be subjected to similar restrictions.
An alternative to the present proposal could be to define HFEM as an independent entity. In our opinion, that would complicate things and it would not serve the purpose of assuring access of novel expensive drugs to this group of patients who are just as disabled as patients with ICHD-3 defined CM.
The strengths of this analysis include a) the use of a validated semi-structured interview conducted by trained health care professionals; b) the robustness and standardization of the Danish National Prescription Registry and correlation with social assistance parameters from Statistics Denmark, and c) the validation of the proportions of CM and HFEM in a Russian student population who had the same semi-structured interview as the Danish study population. Limitations include a) the lack of more granular subdivisions in the HFEM subgroup (e.g. 8–10; 10–12, 12–14 headache days) and correlation with disability, medication use, and social parameters; and b) we added some patients to the CM concept who did not have headache on 15 days a month or more, and this contrasts with the IASP definition of chronic pain (21,22). We feel that this is acceptable as HFEM is so severe that patients are also disabled on days without migraine.
These data should be confirmed by studies in other countries to better document their generalizability, but the robustness of this analysis and its apparent convergence with the experience of clinicians who care for both groups of patients warrants a provisional revision of the chronic migraine criteria until further validation research is completed.
Conclusion
Patients with migraine on eight or more days but not 15 days with headache a month are as disabled as patients with ICHD-3 defined CM. They should be included in revised diagnostic criteria for chronic migraine.
Clinical implications
Patients who have at least eight or more migraine days per month but less than 15 days with headache are comparable to ICHD-3 defined chronic migraine patients with regard to chronicity and disability. Our findings suggest a much-needed simplification of the diagnostic criteria for chronic migraine that better reflects the suffering of many patients who have a high frequency of migraine but no other headache. Extending the definition of chronic migraine to include patients who have at least eight or more migraine days per month but less than 15 days with headache will ensure that patients with significant disease burden and unmet treatment needs are identified and provided appropriate treatment.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Our research group has received grants from Candys foundation (CEHEAD). The funding body had no role in the study.
Ethics board approval
The Danish research group has permissions and approval from the Danish Data Protection Agency (GLO-2010-10) and the Ethical Committee (H-2-2010-122).