
Abstract
The clinical presentation of chronic post-traumatic headache in 53 patients from a highly specialized headache clinic was analysed and classified according to the diagnostic criteria of the primary headaches in The International Headache Classification 2nd Edition, and compared with the 1st Edition. All patients fulfilled the criteria for both editions indicating that the restrictions in the 2nd Edition have no major influence on the prevalence in specialized clinics. We found the phenomenology to be very heterogeneous, but the vast majority (77%) of patients presented with headache resembling chronic tension-type headache, either as the only manifestation or in combination with migraine symptoms. For the first time episodic tension-type headache is described as occurring after head trauma. The prevalence of coexisting analgesic overuse was 42% and the treatment outcome for these patients was just as favourable as in primary headaches, whereas the time-consuming multidisciplinary treatment demonstrated only very modest results.
Introduction
Acute post-traumatic headache following head trauma is frequent and often resolves within a few weeks but for a smaller proportion of patients the headache becomes chronic and often severely disabling (1–5). Because of the high incidence of head trauma (350 per 100 000 in Europe, 180–220 per 100 000 in North America; 75% of these being mild head injury) chronic post-traumatic headache (CPTH) is an important cause of secondary headache (1, 2). The incidence of post-traumatic headache varies between different studies, in an often quoted study by Cartlidge & Shaw (6), 52% had headache during hospitalization, 36% on discharge, 27% at six-month, 18% at one-year and 24% at two-year follow-up. Some more recent studies have shown that 44% had headache after 1–3 months (3) and 20% 3 years after head trauma (1).
CPTH has been a controversy for many years and still opinions differ as regards its pathogenesis, natural course, the role of litigation (2, 6–9) and to what extent it could be explained as analgesic rebound headache (5, 10). The debate concerning an organic vs. psychogenic basis is still ongoing (2, 3, 7, 9) but the evidence to support an organic basis is increasing (7).
Treatment of CPTH is often difficult and unspecific since treatment guidelines mostly copy the recommendations for treatment of the primary headache counterparts (11). Research into this area has only been scarce (11) and multidisciplinary treatment strategies are usually recommended (8).
The phenomenology of this intricate kind of headache is only systematically characterized in a few studies (12, 13). The aim of this study was therefore to analyse and characterize CPTH according to the diagnostic criteria of the primary headaches in the International Headache Classification 2nd Edition (IHC 2nd Ed.) (14). Furthermore we aimed to elucidate the role of analgesic overuse in this particular group of patients, evaluate the treatment outcome and clarify the extent of socio-economic consequences.
Methods
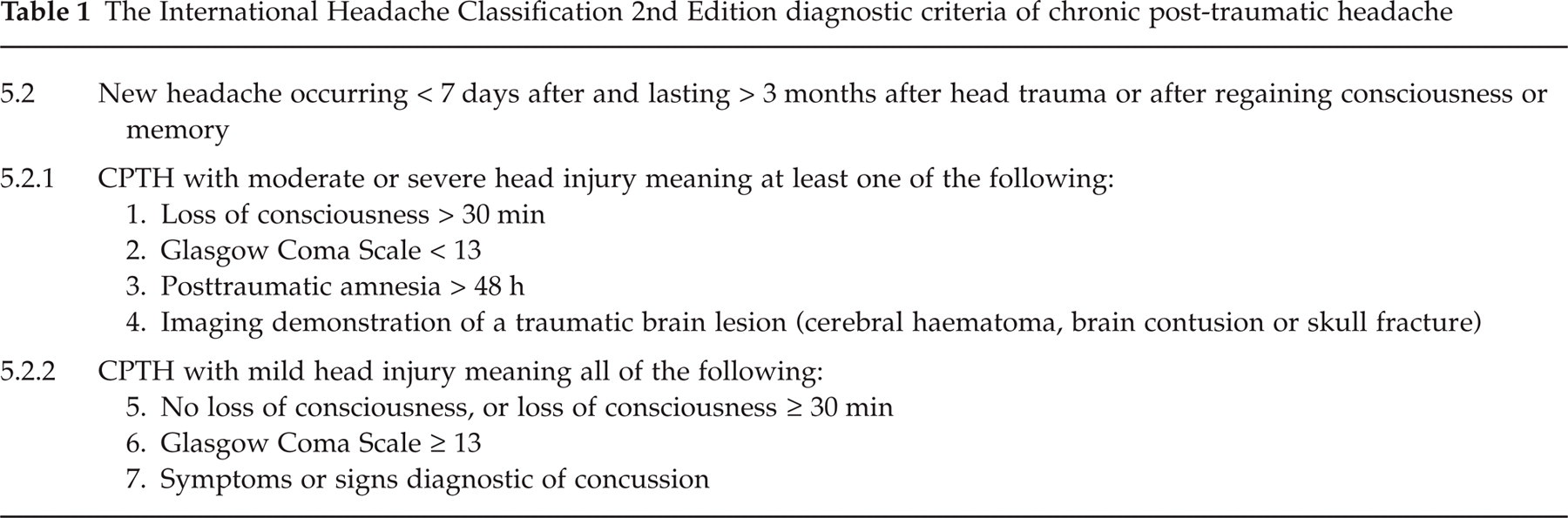
The study was conducted as a file based retrospective study at the Danish Headache Centre where clinical data and diagnostic headache diaries (15) are standardized and systematically recorded. 61 patients with the IHC 2nd Ed. diagnosis CPTH (Table 1) seen on an outpatient basis in the highly specialized Headache Centre from 1 January 2001 to 30 June 2003 were included initially.
The International Headache Classification 2nd Edition diagnostic criteria of chronic post-traumatic headache
For each patient a thorough review of medical record and diagnostic headache diary was made and information on the following headings were recorded: sex, age, family history of headache, pretraumatic headache (frequency and type), head trauma (loss of consciousness, post-traumatic amnesia, examinations) and the post-traumatic headache: One or several different types of headache, temporal relationship between head trauma and onset of headache, persistence after the trauma, pain characteristics (location, intensity, quality, response to routine physical activity), duration and frequency (if episodic), accompanying symptoms (nausea, vomiting, photophobia, phonophobia, aura), use of analgesics. We also obtained information on further somatic complaints (fatigability, sleep disturbance, dizziness, alcohol intolerance), cognitive complaints (memory dysfunction, impaired concentration and attention), affective complaints (irritability, aggressiveness, anxiety, depression, emotional lability), treatment (medical, psychological, physiotherapy, other), treatment outcome and socio-economic consequences.
Results
Sixty-one patients were included initially, 30 women and 31 men. Eight patients were excluded from further analysis: 2 patients did not fulfil the diagnostic criteria as regards close temporal relation between head trauma and onset of headache (the time interval being, respectively, 1 and 3 years), in 5 patients the description (medical record, headache diary) of pain characteristics was incomplete and 1 patient had severe psychiatric comorbidity making assessment of headache unreliable.
Remaining for further analysis were 53 patients, 26 women and 27 men with a median age of 35 years (range 15–83 years); further clinical characteristics are given in Table 2. Thirteen (25%) patients had a family history of headache (tension-type or migraine) in first-degree relatives and 4 (8%) patients had a pre-existing headache prior to the trauma. The type of pretraumatic headache in all 4 patients was migraine without aura that was not altered by the trauma after which all 4 patients developed CPTH resembling chronic tension-type headache in addition.
Clinical characteristics of analysed patients with chronic post-traumatic headache (n = 53)

values are median (range).
IHC criteria indicated in Table 1.
Forty-five (85%) patients had suffered a mild head injury and 8 (15%) patients a moderate or severe head injury (Table 2) according to the IHC 2nd Ed. criteria. All the patients had experienced a direct head trauma – 18 (34%) in a road accident, 16 (30%) following a fall from the upright position, 7 (13%) during a violent attack, 6 (11%) were hit by an object, 4 (8%) fell from a horse and 2 (4%) fell from a great height.
The onset of headache varied only little between a few hours and 3 days after the trauma and so fulfilled the temporal criteria for post-traumatic headache of both the 1st and 2nd Edition of IHC. Only 2 patients had a prolonged interval (respectively 1 and 3 years) and were therefore as already mentioned excluded from analysis.
Thirty-nine (74%) patients had only one type of headache and 14 (26%) patients had two different types. Regarding the patients with only one type of headache 6 (11%) presented with characteristics resembling episodic tension-type headache, 27 (51%) chronic tension-type headache, 1 (2%) migraine without aura and 5 (9%) were unclassifiable (alternating pain characteristics and/or accompaniments) (Table 3). The various pain characteristics and accompanying symptoms of CPTH patients in relation to their clinical presentation are presented in Table 4. For the patients with headache resembling episodic tension-type headache the headache frequency ranged from 3 to 12 days/month, i.e. fulfilling criteria for the frequent form of episodic tension-type headache. Regarding the patients with two different types of headache 4 (8%) patients had both chronic tension-type headache and migraine without aura and 10 (19%) patients had chronic tension-type headache and probable migraine (i.e. fulfilling all but one criteria for migraine) without aura. In total 41 (77%) patients had CPTH resembling chronic tension-type headache (with or without migraine/probable migraine) and the frequency of headache in these patients was daily in 38 (93%) patients, 25 days/month in 2 (5%) patients and 20 days/month in 1 (2%) patient.
Clinical presentation of chronic post-traumatic headaches (n = 53) Values are indicated as absolute values with percentage distribution in brackets

CTTH, Chronic tension-type headache.
Distribution of pain characteristics and accompanying symptoms in CPTH patients
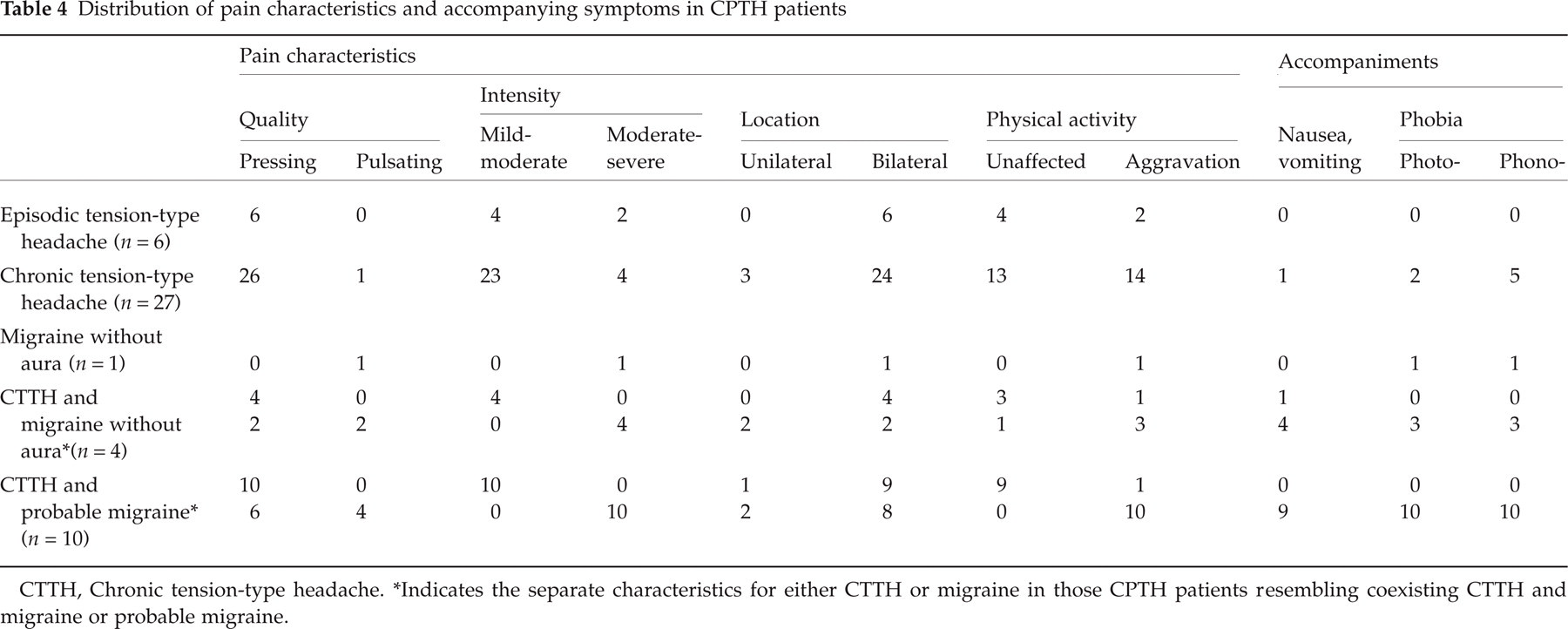
CTTH, Chronic tension-type headache.
Indicates the separate characteristics for either CTTH or migraine in those CPTH patients resembling coexisting CTTH and migraine or probable migraine.
Twenty-two (42%) patients had an analgesic overuse defined as more than 100 tablets/month of mild analgesics and/or use of ergotamine or triptans more than 10 days/month. Among the 13 patients who managed to stop their analgesic overuse 2 (15%) patients fully recovered, 4 (31%) patients experienced remarkable relief (headache frequency reduced from daily to 12 days/month or less) and 7 (54%) patients had no effect or worsening of their headache.
As regards post-traumatic symptoms besides headache we found that 28 (53%) had at least one somatic complaint from among fatigability, sleep disturbance, dizziness and alcohol intolerance, 26 (49%) at least one cognitive complaint from among memory dysfunction, impaired concentration and attention and 14 (26%) had at least one affective complaint from among irritability, aggressiveness, anxiety, depression and emotional lability. Nine (17%) had both somatic, cognitive and affective complaints and 9 (17%) had none of these additional complaints.
Thirty-five of the patients analysed in this study had completed their treatment programme at the Headache Centre at the end of the study and the remaining 18 patients were still in a treatment course. For the 35 patients completed we evalu-ated the treatment outcome and found that 4 (11%) had recovered spontaneously, 6 (17%) had experienced remarkable relief (headache frequency reduced from daily to 15 days/month or less) or full recovery after ending previous analgesic overuse and no other treatment, 3 (9%) had experienced remarkable relief after multidisciplinary treatment with amitriptyline, physiotherapy and psycho-education, 6 (17%) did not respond to this regime and 16 (46%) refused the offered treatment, presented with incomplete evaluation forms or failed to turn up.
For the 35 completed patients we also investigated the socio-economic consequences and found that 2 were dismissed from work, 12 received long (more than 3 months) sickness benefit, 2 had early retirement, 7 were put on reduced working time – in total 21 (60%) received some sort of financial aid or compensation.
Discussion
According to the IHC 1st Edition (16) CPTH must have occurred within 14 days after the head trauma and continue for more than 8 weeks, but many studies have included the so-called late-acquired headaches as described by Cartlidge and Shaw (6). However, because of the high prevalence of primary chronic headache in the general population a close temporal relationship between head trauma and onset of headache is necessary in order to rule out that the headache is actually a primary headache that just happens to arise some time after a head trauma. The revised IHC 2nd Ed (14). is even more restrictive concerning this matter as it requires that the post-traumatic headache occurs less than 7 days after the head trauma and continues for more than 3 months. In the present study all 53 analysed patients fulfilled the diagnostic criteria both for the IHC 2nd and 1st Edition, indicating that the new diagnostic restrictions have no major influence on the great majority of patients with CPTH. Only 2 patients were excluded because they did not fulfil the IHC diagnostic criteria of CPTH as regards a close temporal relationship between head trauma and onset of headache – in the 1st as well as the 2nd Edition of IHC. In this material we did therefore not find many of the so-called late-acquired post-traumatic headaches, indicating that this subgroup is not as common as earlier assumed (6). However, it could also reflect a consequent implementation of the IHC diagnostic criteria in the coding procedure in the present Headache Centre meaning that patients with a history of head trauma were only coded as post-traumatic headache if the IHC requirements were fulfilled.
For many years CPTH was not systematically characterized (2, 17) but in a recent study by Haas (12), 48 patients with CPTH (including headaches arising within 3 months after the head trauma, i.e. not fulfilling the IHC diagnostic criteria) were classified as if they had primary headache according to the criteria of IHC. Seventy-five per cent of these patients had post-traumatic headache fulfilling the criteria for chronic tension-type headache, 21% migraine without aura and 4% were unclassifiable. The study also addressed the role of analgesic overuse in CPTH and found that 19% of the study population and 25% of the patients with post-traumatic headache resembling chronic tension-type headache had an analgesic overuse that might aggravate or even induce chronic analgesic rebound headache. However, it was not evaluated whether cessation of analgesic intake actually had an influence on the headache.
An even more recent study analysed chronic post-traumatic headache following cranio-cervical acceleration/deceleration trauma, also according to the IHC criteria, and found that 37% had chronic post-traumatic headache resembling tension-type headache, 27% migraine and 18% cervicogenic headache (13).
In our study the vast majority (77%) of patients resembled chronic tension-type headache, either as the only manifestation or in combination with migraine symptoms and only 9% were unclassifiable. None of the patients had post-traumatic headache resembling the two other major classes of primary headaches, migraine with aura and cluster headache.
These results are in agreement with the before mentioned previous studies (12, 13). However, episodic tension-type headache has not been shown to occur as post-traumatic headache in any other study and the prevalence of migraine without aura is low compared to those other two studies. Indeed, others have reported migraine both with and without aura to be a frequent type of post-traumatic headache (18). In contrast to prior studies, we used prospective diagnostic diaries and recorded therefore more than 1 type of headache in some patients (26%) and probably also a higher proportion of analgesic overuse than in former studies.
We found a fairly high proportion of patients with analgesic overuse; 42% of all and 44% of chronic tension-type headache patients compared to 19% and 25% in the study by Haas (12). Seven (54%) of the 13 detoxified patients were not relieved after stopping their overuse of analgesics suggesting that the post-traumatic headache in these patients was not aggravated or induced by analgesics. However, the results do emphasize the importance of a detailed analysis of the use of analgesics in all headache patients. Likewise, cessation of such analgesic overuse should be encouraged in CPTH patients also due to a remarkable relief in the same rate as in the primary headaches.
Eight per cent of the patients had pretraumatic headache. These patients were not excluded from analysis as in most other studies of post-traumatic headache populations because:
their post-traumatic headache was undoubtedly distinct from their pre-existing headache
new guidelines of coding the secondary headaches in IHC 2nd Ed. which open the possibility of coding worsening of pre-existing primary headache in close temporal relation to trauma as both the primary and secondary headache diagnosis
a study by Jensen & Nielsen (19) who found that patients with and without pretraumatic headaches have similar incidences of chronic post-traumatic headache, i.e. pre-existing headache does not influence the risk of developing post-traumatic headache
The majority (85%) of patients in this study had suffered mild head injury rather than moderate/severe head injury which agrees with most other studies of post-traumatic headache (3, 12, 19), and supports the often quoted paradox that there is an inverse relationship between the severity of the head trauma and the occurrence of chronic post-traumatic headache (2, 6, 7, 12, 19–21).
It is often stated that post-traumatic headache is mostly part of a more complex constellation of symptoms known as the postconcussional syndrome (3, 20) including further somatic complaints (fatigability, sleep disturbance, dizziness, alcohol intolerance), cognitive complaints (memory dysfunction, impaired concentration and attention) and affective complaints (irritability, aggressiveness, anxiety, depression, emotional lability). This was also true in this study where, respectively, 53%, 49% and 26% had such additional complaints and only 17% had headache alone.
Sixty per cent of the completed patients had received some sort of financial aid or compensation from society which supports the general assumption that chronic post-traumatic headache causes a substantial socio-economic cost due to absence from work, payment of sickness benefit, early retirement and claim for compensation. A detailed long- term analysis of the socio-economic costs of such post-traumatic symptoms could probably be very useful and lead to future prophylactic information campaigns.
The treatment outcome was fairly better than expected from the literature and medication induced headache was very frequently occurring and just as rewarding to treat as in the primary headaches. The time-consuming multidisciplinary treatment strategy demonstrated, however, only very modest results. This brings attention to evaluation of present procedures, more effective treatment strategies and an urgent need for randomised, placebo-controlled studies.