
Abstract
Background
The proper identification of chronic migraine is one of the mainstays for general practitioners. This study therefore aims to assess the epidemiology and determinants of chronic migraine in primary care in Italy by testing five operational case definition algorithms.
Methods
Five case definition algorithms defining chronic migraine were developed to estimate the prevalence and incidence rate of chronic migraine in the Health Search database. For each algorithm, we conducted a nested case-control analysis to quantify the level of association between certain determinants and incident cases of chronic migraine.
Results
Considering a cohort of 1,091,032 patients (52% were females), the prevalence rate of chronic migraine increased from the first to the fifth case definition algorithm ranging from 0.03 to 0.28%. No 95% confidence interval overlapped the others, and every confidence interval reliably maintained 2% precision. Incidence rates showed a growing trend (0.008–0.056 per 100,000 person-years) as well. All case definition algorithms were able to capture sex (i.e. female) and nonsteroidal anti-inflammatory drug (NSAID) overuse as statistically significant determinants of incident cases of chronic migraine. Depression was associated with a statistically significant increase of incidence rate of chronic migraine only for two case definition algorithms.
Conclusion
Our findings show that prevalence and incidence rate of chronic migraine are underestimated when compared with current literature. On the other hand, we found acceptable correctness of chronic migraine definition in the light of the association with well-known determinants.
Introduction
Migraine is a relevant public health concern due to its association with increasing disability. In the Global Burden of Disease Study 2016 (GBD 2016) it was ranked the second–highest cause of disability worldwide in both males and females under the age of 50 (1). According to the International Classification of Headache Disorders migraine is classified as acute/recurrent or episodic form and chronic form. In general, a distinction between the episodic migraine (EM) and chronic migraine (CM) is based on the frequency and duration of migraine episodes. Namely, CM is defined as at least 15 days by month along with duration of 4 hours per episode for 3 subsequent months or longer and with 8 days a month on which the headache and associated symptoms are consistent with migraine attacks (2,3). Given that primary CM is rare, it has been suggested that CM results from episodic migraine that gradually increases in attack frequency (4).
From a clinical perspective, there are well-known determinants for CM occurrence. Namely, these include sex, obesity, depression, and nonsteroidal anti-inflammatory drug (NSAID) overuse (5–9).
Overall, the prevalence of migraine ranges from 11 to 15% (10). Considering CM, prevalence is usually reported to be 1–2% in a general population and around 2–4% in Western countries (10–13).
General practitioners (GPs) play an important role in migraine’s diagnosis and management. Indeed, around 4% of primary care consultations in the UK are related to headache (14). Nevertheless, a positive adequate management of patients with migraine is often complex, and it can be an important challenge for GPs, in particular regarding non-expert clinicians (15), leading to misdiagnosis and/or inappropriate treatment (16). The understanding of epidemiology of CM in primary care may be therefore relevant for a public health perspective. Nevertheless, few studies have been carried out on this topic. The present study therefore aims to assess the epidemiology of CM in primary care in Italy by testing a set of operational algorithms defining CM.
Methods
Data sources
We used the Health Search Patients Database (HSD), an Italian general practice database that includes patients’ records of a group of over 1000 GPs homogenously distributed across Italy. GPs voluntarily agreed to attend training courses for data entry on patients’ information.
Patients’ demographic details are linked with an encrypted code to clinical records (diagnoses, referrals, tests prescriptions and results), drug prescriptions (drug name, date of filled prescription, and number of days’ supply), lifestyle-related records (i.e. Body Mass Index (BMI), smoking and alcohol), hospital admissions, and date of death. In the HSD, medical diagnoses and prescribed medications are coded using the 9th version of the International Classification of Disease, Clinical Modification (ICD-9-CM) and the Anatomical Therapeutic Chemical (ATC) classification system, respectively. GPs are instructed to couple diagnoses with every prescription (e.g. indication of drug use).
To be considered for participation in epidemiological studies, GPs are required to meet up-to-standard quality criteria concerning the levels of coding, prevalence of well-known diseases, mortality rates, and years of recording (17). When this study was initiated, 700 GPs homogeneously distributed across all areas of Italy, and covering a patient population of 1,163,855 individuals, met the standard quality criteria and were included in the study. The HSD has been used in a number of epidemiological studies (18–21).
With regard to the classification and implementation of observational drug-related research, as issued by the Italian National Drug Agency (an entity belonging to the Italian Ministry of Health), the present study does not require approval by an Ethics Committee in Italy (Italian Drug Agency note dated 3 August 2007). No patients or carers were directly involved in the conducting of this study.
Study population
We selected a cohort of patients active in the HSD aged ≥18 years during the period between 1 January 2002 and December 2016. The date of the first GP’s visit within the eligibility period was the study entry date. From this population, we excluded patients with less than 1 year’s medical history prior to the entry date. These patients were followed up until the occurrence of these events, whichever comes first: diagnosis of CM (see paragraph on “Event definition”), death, end of data registration in the GP’s database, or the end of the study period (31 December 2016). To calculate the prevalence rate, patients with less than 3 months preceding the index date did not enter the cohort. In order to calculate the incidence rate, patients with less than 8 years of clinical history preceding the index date did not enter in the cohort.
Event definition
According to the International Classification of Headache Disorders, CM is specifically defined by the presence of migraine attacks for at least 15 days per month for 3 consecutive months (3). Therefore, we hierarchically elaborated two groups of case definition algorithms for CM including three and two different algorithms, respectively. The first group was based on at least one migraine-related contact coded via ICD-9-CM being registered by month for 3 consecutive months (Algorithm 1A).
Thus, the others case definition algorithms were based on Algorithm 1A or when there were two contacts for 2 consecutive months and/or medications used for migraine attack (Algorithm 1B) and/or prophylaxis (Algorithm 1C) covering 15 days of therapy for 3 consecutive months. For the evaluation of duration of migraine attacks, we selected patients identified by two migraine-related contacts for two consecutive months (coded via ICD-9-CM) who were prescribed with medications used for migraine attack and/or prophylaxis. Using these criteria, we were able to identify patients with migraine episodes based on the duration of each prescription. To do so, for each medication class we adopted the prescribed daily dose (PDD). As such, the overall prescribed amount (e.g. in mg) was divided by the related PDD to obtain the duration for each prescription. The second group of case definition algorithms was based on the same aforementioned definition but keeping the three migraine related contacts for 3 consecutive months coupled with medications use for migraine attack (Algorithm 2A) and/or prophylaxis (Algorithm 2B) (Supplemental Figure 1). This hierarchical approach attempted to define CM diagnoses with an acceptable level of “completeness” to allow the identification of the highest possible number of events and “correctness” to reduce misclassification of cases.
Operationally, migraine-related contacts were identified using the following ICD-9-CM codes: 346.0*, 346.1*, 346.2*, 307.81, 784.0, all coupled with the term “migraine” as commented by GP in the diagnosis descriptor. We excluded the codes: 346.00, 346.10, 346.20, 346.80, 346.2 coupled with “abdominal”, “ciliary” or “neuralgic migraine” in the coding field. Furthermore, among patients with the aforementioned ICD-9-CM diagnosis, we identified prescriptions of medication for acute migraine attacks, including: i) triptans (ATC: N02CA*); ii) ergot derivatives (ATC: N02CC*); iii) NSAIDs (ATC: M01A*); iv) paracetamol (ATC: N02BE01, N02BE51, N02BE71); v) paracetamol-codeine combinations (ATC: N02AA59 besides the previous codes coupled with “codeine” in drug description). Then, we considered prescriptions for migraine prophylaxis, including: i) antidepressants (tricyclic (ATC: N06AA*) and SSRI (ATC: N06AB*)); ii) antiepileptic drugs (ATC: N03A*); iii) beta blockers (ATC: C07*); iv) dopaminergic drugs (ATC: N05A*); v) calcium antagonists (ATC: C08*); vi) pizotiphen (ATC: N02CX01); vi) antihistamines (ATC: N07CA*, R06A*).
Nested case-control analysis
The date of CM definition was the study index date, which was defined as the 31st day of the third month of the related case definition algorithm. For each case, 20 controls were randomly selected from the risk set of the respective case using the incidence density sampling method (i.e. at the time of each case diagnosis) (22). Controls (i.e. person-times) were therefore matched with cases by month and year of cohort entry, age (±5 years), and duration of follow-up. The index date of the controls was the date of the respective cases.
We used a nested case-control analysis because of the time-varying nature of exposure, the size of the cohort, and the duration of follow-up. When compared with a time-dependent survival analysis, a nested case-control analysis is computationally more efficient, while producing odds ratios that are unbiased estimators of incidence rate ratios (RR), with little or no loss in precision (22). Thus, while a cohort study using a survival analysis uses the full risk set (i.e. all patients still at risk of the event at the time of the case’s event), the nested case-control analysis uses a random sample of patients (i.e. controls) from that same risk set. In other words, the nested case-control analysis should provide nearly identical results as that of the cohort approach with the advantage of being computationally more efficient and easier to implement.
Candidate determinants
We considered all potential determinants being registered in the HSD which, along with sex and age, were known to affect the occurrence of incident CM (5–7,23). The following variables were measured ever before or on the entry date, unless otherwise specified. Namely, obesity (ICD-9-CM: 278.0* or BMI ≥30 kg/m2), alcohol abuse and/or alcohol-related disease, smoking (current, former, non-smokers; last available measurement); depression (in the overall period preceding or on the entry date); NSAID overuse (30 days of cumulative use during 90 consecutive days) was defined in the period preceding the index date by adding a latency of 90 days (i.e. this period was considered as free of use for NSAIDs) to minimize the reverse causation (3,24,25).
Statistical analysis
We reported descriptive statistics for continuous (mean (standard deviation-SD)) and categorical values (N and percentage (%))
Prevalence and incidence rate of CM were calculated for each case definition algorithm defining the event. To calculate the prevalence rates, we identified both “old” and “new” cases of CM being captured in 2016 as the numerator. The number of patients being active in the database and with at least 3 months of follow-up being registered at 31 December 2016 was the denominator. Given that up to 26% of cases of CM go into remission within 2 years (26), this calculation considered as prevalent cases of CM (i.e. increasing the numerator) those identified up to 8 years earlier (up to 2008 included) as well, using the same selection criteria adopted for 2016. The incidence rate was calculated in the study cohort, dividing the number of new cases identified in 2016, by excluding those with the same diagnosis in the previous 8 years (numerator) by the total number of person-years cumulated during follow-up (denominator). All patients with at least 3 months of follow-up therefore contributed with their individual person-time.
A conditional logistic regression was used to calculated odds ratios (ORs) and related 95% confidence intervals (CI) for each potential determinant of CM as defined by every case definition algorithm. In particular, the logistic regression was conditioned on calendar period (i.e. month and year of cohort entry), age (i.e. ±5 years) and duration of follow-up (i.e. matching criteria). Those determinants were statistically significantly associated with CM and were linearly combined to retrieve a single estimate with related 95% CI.
We also conducted a sensitivity analysis to test the potential misclassification of old cases of CM being counted in 2016 as the numerator. In essence, patients diagnosed with CM before 2016 might be healed in 2016 with a rate of almost 25% every two years (27). The prevalence rate of CM was therefore re-calculated by limiting the cases of CM to those with old CM (from 2009 to 2015) and at least one current (in 2016) contact of migraine coded via ICD-9-CM.
We used STATA software, version 11 (Stata Statistical Software: Release 11. College Station, TX: StataCorp 2009 LP.).
Results
A total of 1550, 1791, 2991, and 368, 812 cases of CM were identified according to case definition Algorithm 1A, 1B, 1C and 2A, 2B, respectively. Among patients with at least one migraine-related contact per month for 3 consecutive months the mean number of contacts were 1.9, 1.5, and 1.6 in the first, second and third month, respectively. The highest number of contacts being registered in the first month were 12, while the second and third month registered nine and 12 contacts, respectively.
Prevalence and incidence rate of chronic migraine in 2016.

CI: confidence interval; CM: chronic migraine.
100,000 person-years.
Determinants of chronic migraine across case definition algorithms (Odds Ratio CI 95%).
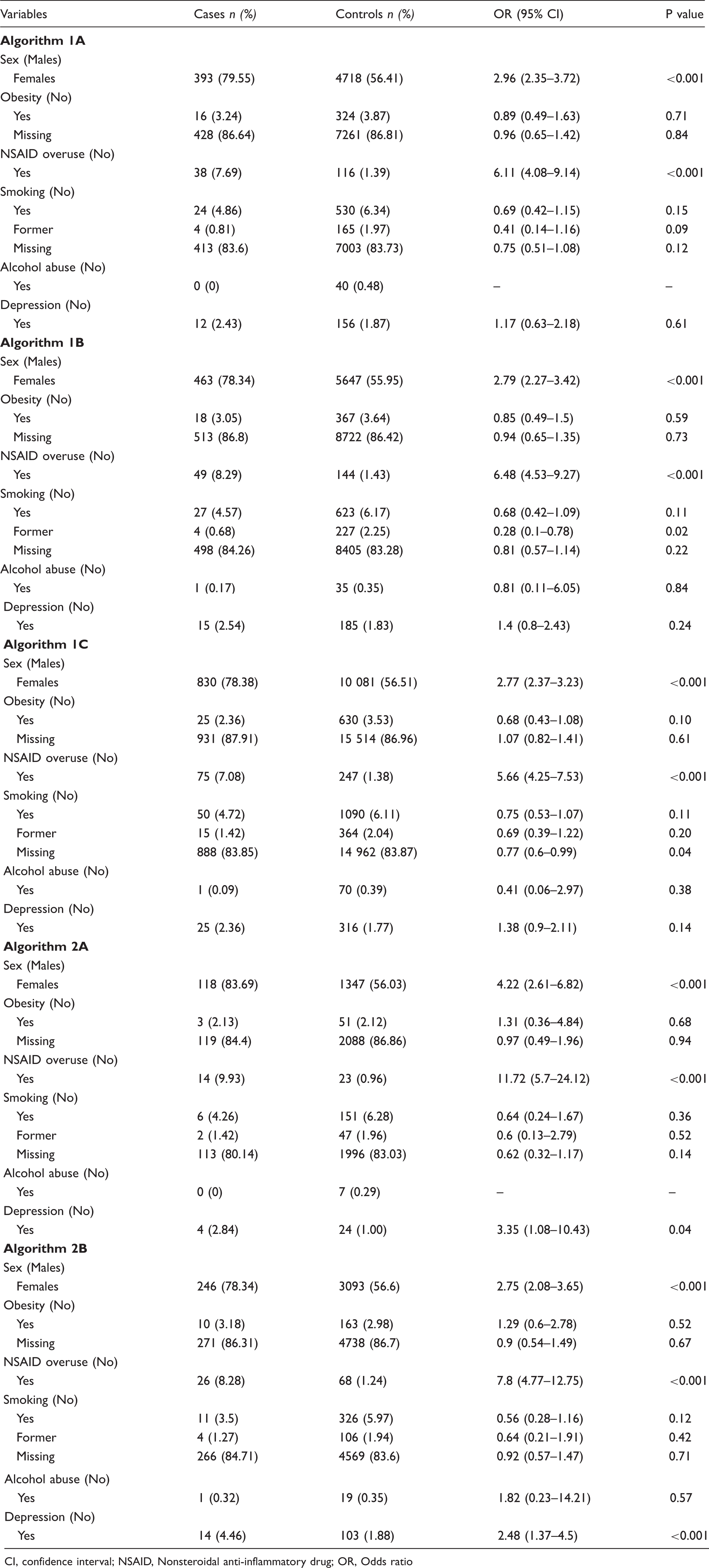
CI, confidence interval; NSAID, Nonsteroidal anti-inflammatory drug; OR, Odds ratio
Considering the other determinants, the presence of depression was associated with an increased incidence rate of CM although not statistically significant across case definition Algorithms 1A–1C. Otherwise, depression was statistically significantly associated to CM with OR of 3.35 (95% CI: 1.08–10.43) and 2.48 (95% CI: 1.37–4.5) for case definition Algorithm 2A and 2B, respectively.
Point estimates pooling sex, NSAID overuse and depression across case definition algorithms.
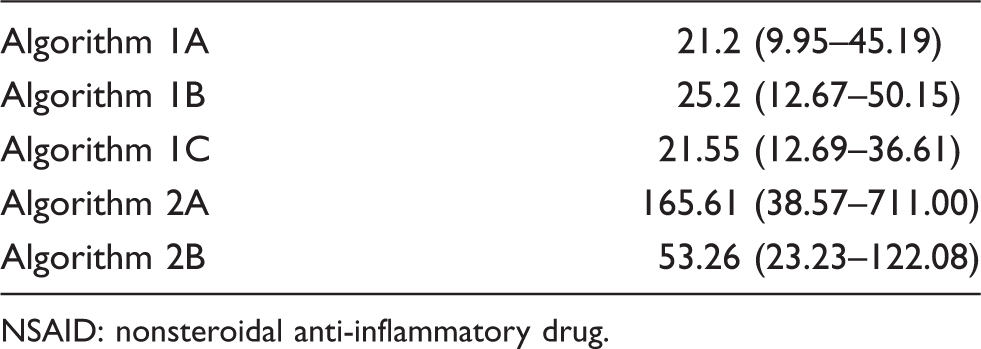
NSAID: nonsteroidal anti-inflammatory drug.
The best trade-off between the ability to identify the highest possible number of events and to reduce the misclassification of CM (i.e. the CI of the combined ORs overlaps with those of the most specific case definition Algorithms) was therefore obtained using case definition Algorithm 1C.
Discussion
To the best of our knowledge, this is the first nationwide population-based study on the epidemiology of CM in a primary care setting. Our findings indicate that although diagnoses of CM are underestimated in HSD, the strong association with well-known determinants reflects a relevant degree of correctness in the definition of CM.
The prevalence and incidence rates of CM were underestimated in our study, when compared with current medical literature. Indeed, the prevalence of CM is usually reported to be 1–2% in a general population, and about 8% among individuals with migraine (10,11).
This finding might be explained by the fact that GPs do not properly recognize and/or register CM, while missing cases are likely treated by Headache Centers in the first place.
The correctness of CM diagnosis was found with consideration of the significant association between CM and the investigated determinants, such as female sex, NSAID overuse and depression. In particular, an increase in size effect for the aforementioned determinants was found when the combination between diagnoses and medications for flares counted at least 15-day exposure periods monthly for 3 consecutive months.
There is a well-known relationship between CM and female sex; data from the 2015 Global Burden of Disease Study showed that migraine is two to three times more prevalent in women than in men (28). Furthermore, the results of the US AMPP study showed a higher risk of transition from episodic to CM in women than men (29).
In our study, the highest association was found between CM and NSAID overuse. It is common knowledge that migraine is frequently associated with overuse of acute medications, and this wrong practice is one of the factors contributing to migraine transition to chronic forms (8). Furthermore, NSAIDs are the most commonly overused drugs, also because they are easily available as over the counter (OTC) medications (30).
Specifically, the association between medication overuse and the risk of CM depends on a number of factors (e.g. type of molecule, days of medication use, and the headache patient’s characteristics) (31). Indeed, as reported by Lipton et al. (32), an increasing number of days per month of NSAID use was associated with increasing risk of CM onset in persons with 10–14 headache days per month.
We found a lower association between depression and CM onset, compared to the aforementioned determinants. Nevertheless, among the psychological factors, depression is one of the most important risk factors for CM. Indeed, Ashina et al. (33) reported that increased severity of depression led to an elevated risk of progression from episodic migraine to CM.
This study has some limitations. First, the use of the length of drug prescriptions to identify the cases of CM could reduce the correctness because they could not accurately reflect the actual presence of pain, its intensity and its related duration. Along this line, the lower estimates for prevalence rate of CM calculated in the sensitivity analysis may suggest a reduced event correctness as well. Nevertheless, the increasing association with determinants that we found for case definition algorithms, including medications for migraine attacks, was reassuring, as well as the effect size found for females (up to 4.5) and NSAID overuse (up to 11). Second, the case definition algorithms defining CM that we investigated cannot be automatically implemented in every data source before being confirmed by a formal validation study. In this respect, we attempted to find the best trade-off between completeness and correctness given that clinical databases are fully anonymized, including GPs’ identification, and validation studies is often unfeasible. For this reason, we would like to suggest a feasible approach to define such an event using retrospective data sources where the different levels of event accuracy may be sought and tested. Third, the presence of depression showed inconsistencies across the tested case definition algorithms because of the reduced statistical power (i.e. low number of exposed cases diagnosed with depression in their medical history). Nevertheless, the CIs of non-significant estimates were still contained within those identified by case definition algorithms able to find significant associations.
Fourth, linearly combining the significant determinants, the higher OR and wider 95% CI related to the second group of case definition algorithms (i.e. Algorithm 2A and Algorithm 2B) compared to the first group (i.e. Algorithm 1A, 1B and 1C) showed uncertainty across the tested case definition algorithms because of the reduced statistical power (i.e. including more contacts with GP, we were able to reduce case definition misclassification, despite a reduction in the number of CM cases). Nevertheless, the lower bound of the CI kept a relevant effect size (38.57), so confirming the direction and strength for this association.
Finally, we were unable to identify the use of OTC medications. However, given that a statistically significant association was found for NSAIDs being prescribed by GPs, the bias due to missing OTC use should be non-differential between cases and controls, so further increasing the association with the outcome.
Conclusion
This study provides information about epidemiology of CM in primary care. Our findings indicate that HSD is able to reliably capture diagnoses of CM, although GPs should recognize and register them with greater completeness. By doing so, GPs should identify CM early, and properly manage and refer CM sufferers to specialists because of the disease progression.
Public health relevance
Diagnosis of chronic migraine in the Italian primary care setting features low completeness (i.e. sensitivity) even using different case definition algorithms to define this disease. The association between chronic migraine with well-known determinants (i.e. sex, NSAID abuse) reflects a high degree of correctness (i.e. specificity) in defining chronic migraine. Italian general practitioners should detect and register chronic migraine diagnoses with better completeness. By doing so, an accurate definition of chronic migraine would support decision makers in identifying effective prevention and decision strategies.
Supplemental Material
CEP889351 Supplemetal Material1 - Supplemental material for Epidemiology and determinants of chronic migraine: A real-world cohort study, with nested case-control analysis, in primary care in Italy
Supplemental material, CEP889351 Supplemetal Material1 for Epidemiology and determinants of chronic migraine: A real-world cohort study, with nested case-control analysis, in primary care in Italy by Ettore Marconi, Serena Pecchioli, Mihaela Nica, Delia Colombo, Francesco Mazzoleni, Francesco De Cesaris, Pierangelo Geppetti, Claudio Cricelli and Francesco Lapi in Cephalalgia
Supplemental Material
CEP889351 Supplemetal Material2 - Supplemental material for Epidemiology and determinants of chronic migraine: A real-world cohort study, with nested case-control analysis, in primary care in Italy
Supplemental material, CEP889351 Supplemetal Material2 for Epidemiology and determinants of chronic migraine: A real-world cohort study, with nested case-control analysis, in primary care in Italy by Ettore Marconi, Serena Pecchioli, Mihaela Nica, Delia Colombo, Francesco Mazzoleni, Francesco De Cesaris, Pierangelo Geppetti, Claudio Cricelli and Francesco Lapi in Cephalalgia
Footnotes
Acknowledgements
All persons that contributed to this manuscript met the criteria for authorship and are listed as authors.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FL and EM provided consultations in protocol preparation for epidemiological studies and data analyses for Novartis, IBSA and Angelini. FM and CC provided clinical consultations for Novartis, IBSA, and ADC and MN are employers at Novartis. SP, FDC and PG declared no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Novartis Pharma Italy.
Ethics or Institutional Review Board approval
With regard to the classification and implementation of observational drug-related research, as issued by the Italian National Drug Agency (an entity belonging to the Italian Ministry of Health), the present study does not require approval by an Ethics Committee in Italy (Italian Drug Agency note dated 3 August 2007). No patients or carers were directly involved in the conducting of this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.