
Abstract
Background
Localized facial scleroderma usually presents as frontal linear morphea or progressive hemifacial atrophy. Only isolated cases of trigeminal painful neuropathy have been described.
Case report
A 43-year-old woman developed an oval lesion on the right cheek. After 1 year, she noticed constant “pulling” pain and episodes of lancinating pain, both spontaneous and triggered by chewing and cold drinks. She was diagnosed with solitary morphea profunda and CT scan, ultrasonography, cranial MRI and biopsy were completed. Methylprednisolone (1 gr/day for 3 days) was prescribed. For pain, gabapentin, oxcarbazepine, amitryptiline, pregabalin and eslicarbacepine were all ineffective. A capsaicin patch was placed with prolonged benefit. Later on, the pain slightly worsened; occipital blockade was effective and methotrexate was recommended.
Conclusion
This is the first case of solitary morphea profunda associated with painful trigeminal neuropathy. Treatment should include immunosuppressants and treatment of neuropathic pain, in which local therapies seem particularly beneficial.
Introduction
Scleroderma is an autoimmune disease characterized by vascular damage, skin inflammation and subsequent fibrosis. It includes localized scleroderma (LSc), also known as morphea, and systemic scleroderma (SSc). Organ fibrosis and Raynaud’s phenomenon are usually absent in LSc, whereas they are usually present in SSc (1,2). Classification of morphea is often difficult. Classic plaque-type morphea is an indurated and solitary cutaneous oval plaque that involves the dermis and the subcutaneous fat. Many subtypes have been described, depending on different patterns of distribution, morphology and depth of involvement. Therefore, solitary Morphea profunda (SMp) is a plaque-like morphea that may also involve muscle and bone. Linear morphea is the most well-defined clinical entity, as it commonly has a forehead location, mainly affects children and has a linear morphology (morphea en coup de sabre) and high depth of invasion, including muscular and bony structures. When hemiatrophy progressively affects skin and craniofacial tissue from one or more trigeminal branches down the entire face, the clinical entity is named progressive hemifacial atrophy (PHA), also known as Parry-Romberg syndrome (2). Both linear morphea and PHA may coexist and are thought to exist on a spectrum of localized scleroderma, as histopathology is often undistinguishable (3). The etiology, although unknown, has been hypothesized as a lymphocytic neurovasculitis involving trigeminal branches (4).
In PHA, as well as in linear morphea, neurological involvement has been frequently described including myopathy, epilepsy, migraine, ophthalmologic symptoms, pyramidal signs, cognitive impairment, and cranial nerve involvement (4). Painful trigeminal neuropathy has scarcely been described in the literature (5–7), although it is probably underdiagnosed, following an internet survey among patients (8). Here we describe a patient suffering from an SMp localized in the right cheek, causing painful trigeminal neuropathy.
Case report
A 43-year-old right-handed Caucasian woman with no relevant medical history started, at 40 years of age, to notice a raised lesion on the right cheek “like a bite”, of hard consistency. Over approximately 1 year, she noticed that the lesion grew and associated a mild continuous pulling pain in the area. After an episode of trismus, she began to notice that the lateral region of the zygomatic arch on the right side “was sinking” and began to have episodes of lancinating pain lasting seconds, located in the area of the raised lesion, which rated 8–9 out of 10 on the Verbal Rating Scale. She experienced up to 10 episodes a day. During the pain, she experienced ipsilateral lacrimation with no other cranial autonomic symptoms. Pain could be spontaneous or triggered by chewing, teeth brushing and cold drinks but not by cutaneous stimulus within the lesion. There was no associated nausea, photo/phonophobia nor pain aggravated by movement. She was not aware of any family history of headache or trigeminal neuralgia. On physical examination, there was an atrophic plaque with hard consistency in the right cheek of 5 × 3 cm in approximate diameter (Figure 1). Pinprick touch over the area showed hyperalgesia, but would not follow the distribution of any complete branch of the trigeminal nerve. There was no tenderness in the region of the occipital nerve. The rest of the neurological examination revealed no other alterations. She was evaluated in the Dermatology consultation, being diagnosed with Solitary Morphea profunda (SMp). CT and cranial MRI were performed, showing a soft tissue lesion located in the subcutaneous cellular tissue, adjacent to the right masseter muscle (Figure 2), with no neurovascular contact or morphological changes in the trigeminal nerve. Additionally, ultrasonography of the right cheek was performed, showing loss of subcutaneous fat. She had previously been taking gabapentin (600 mg daily) without pain relief.
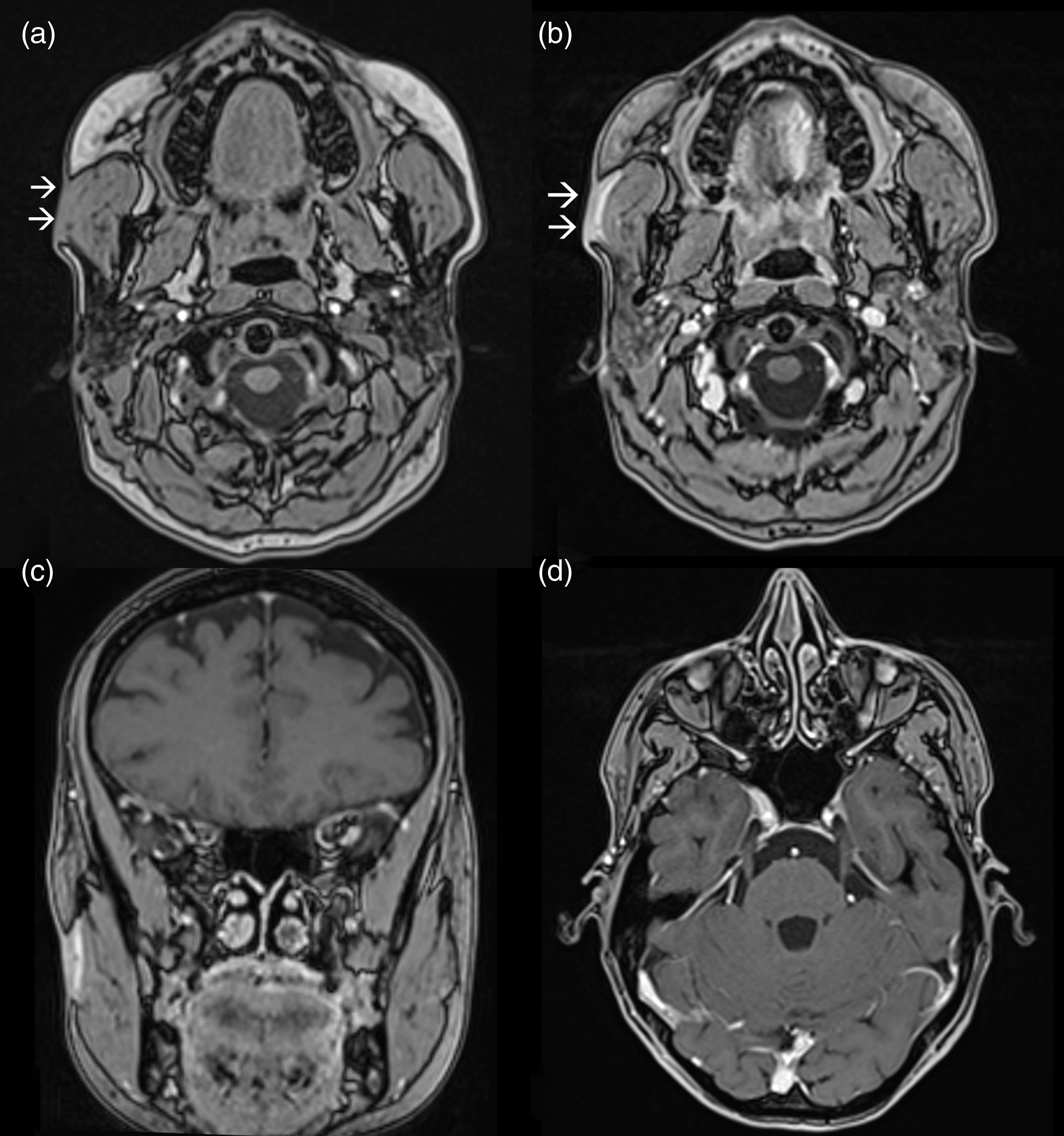
Oval lesion of 5 × 3 cm in approximate diameter in patient’s right cheek. MRI (3T): T1-weighted-contrast-enhanced, T2-FLAIR, diffusion weighted images (DWI), susceptibility weighted imaging (SWI) and three-dimensional (3D) constructive interference in steady state (CISS) sequences were performed. T1 weighted images showed a soft tissue plaque located in the subcutaneous cellular tissue adjacent to the right masseter muscle (a) which enhanced after gadolinium as observed in the axial (b) and coronal projections (c). The course of the right trigeminal nerve showed no abnormalities (d).
Skin biopsy was performed and showed a collagenous connective tissue arranged in bands. No adipose tissue was present, nor was inflammatory infiltrate observed. Nevertheless, following experts’ guidelines (2), an intravenous pulse of methylprednisolone (1000 mg/day for 3 days) was administered. Methotrexate was considered, but after talking to the patient this approach was initially dismissed due to her child-bearing potential. Anaesthetic blockades with lidocaine were not considered initially, as the pain affected distal trigeminal fibres and its distribution was not restricted to a specific trigeminal terminal branch. Gabapentin was substituted by oxcarbazepine, increasing the dose up to 900 mg daily although it was reduced to 600 mg/day due to dizziness. Additionally, amitriptyline was prescribed up to 50 mg with only slight pain relief. Afterwards, a capsaicin patch (179 mg) was applied over the V2 dermatome in the right side for 1 hour. This caused an erythematous reaction and burning pain, which resolved with NSAIDS and applying cold therapy. After discharge, lancinating pain attacks significantly improved in severity from 9/10 to 2–3/10 on the Verbal Rating Scale. Furthermore, pulling continuous pain over the lesion almost disappeared. Pain remained unchanged for 2 years, but the lesion grew moderately involving no other facial regions. In the most recent follow up the pain worsened again, the area of hyperalgesia spread to involve the pre-auricular region and the patient was treated with high dose pregabalin (300 mg) and eslicarbazepine (1200 mg) with no relief. The occipital region was tender and therefore, following previous recommendations (6), an ipsilateral great occipital nerve (GON) blockade was performed (lidocaine 2% 2 ml and 40 mg of methylprednisolone) with moderate efficacy over both types of pain. Additionally, oral methotrexate (25 mg/week) was recommended in order to treat the underlying disease, although it has not been started to date.
Discussion
As commented above, SMp is defined as an extension of the skin lesion beyond the dermis, involving adipose tissue, the fascia or muscle (1,2). Although this type of lesion is characteristically found in the upper part of the back, our patient’s lesion, with an oval shape and indurated skin, can correctly be classified as SMp. Therefore, this would be the first reported case of this specific type of LSc involving the face and can be classified as painful trigeminal neuropathy attributed to morphea. However, even after several attempts to classify scleroderma (1,2), distinction among the different types is not always clear and overlap is common. In our opinion, this patient may be suffering an early stage of LSc that could potentially progress to Parry-Romberg Syndrome. In fact, a 20-year follow-up found that disease pattern in facial involvement changed progressively over time in a series of patients (10).
Although the predominant pain was lancinating and could be attributed to trigeminal neuralgia, as previously published (6), the patient suffered continuous pain and most attacks described herein were spontaneous. Additionally, there was no cutaneous trigger point. Hence, we considered this to be a painful trigeminal neuropathy attributed to SMp as pain was localized in the distribution of the trigeminal nerve affected by the disorder and it developed clearly after the disorder’s onset. Furthermore, there was a patch of hyperalgesia (a positive sign of trigeminal nerve dysfunction) over and surrounding the skin lesion, therefore fulfilling the latest diagnostic criteria (11). The morphea plaque may have damaged distal trigeminal fibres, leading to the patient’s symptoms.
Treatment for pain.

The only case in which carbamazepine was effective was diagnosed with trigeminal neuralgia (5).
Clinical implications
Localized scleroderma involving the face may cause painful trigeminal neuropathy even as a Morphea profunda presentation. Treatment should include prompt immunosuppressive therapy as well as specific neuropathic pain treatment, in which local approaches have had beneficial results.
Footnotes
Patient consent
Informed consent was obtained from the patient included in this case report.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.