
Abstract
Background
The association of trigeminal neuralgia with pontine lesions has been well documented in multiple sclerosis, and we tested the hypothesis that occipital neuralgia in multiple sclerosis is associated with high cervical spinal cord lesions.
Methods
We retrospectively reviewed the records of 29 patients diagnosed with both occipital neuralgia and demyelinating disease by a neurologist from January 2001 to December 2014. We collected data on demographics, clinical findings, presence of C2-3 demyelinating lesions, and treatment responses.
Results
The patients with both occipital neuralgia and multiple sclerosis were typically female (76%) and had a later onset (age > 40) of occipital neuralgia (72%). Eighteen patients (64%) had the presence of C2-3 lesions and the majority had unilateral symptoms (83%) or episodic pain (78%). All patients with documented sensory loss (3/3) had C2-3 lesions. Most patients with progressive multiple sclerosis (6/8) had C2-3 lesions. Of the eight patients with C2-3 lesions and imaging at onset of occipital neuralgia, five (62.5%) had evidence of active demyelination. None of the patients with progressive multiple sclerosis (3/3) responded to occipital nerve blocks or high dose intravenous steroids, whereas all of the other phenotypes with long term follow-up (eight patients) had good responses.
Conclusions
A cervical spine MRI should be considered in all patients presenting with occipital neuralgia. In patients with multiple sclerosis, clinical features in occipital neuralgia that were predictive of the presence of a C2-3 lesion were unilateral episodic symptoms, sensory loss, later onset of occipital neuralgia, and progressive multiple sclerosis phenotype. Clinical phenotype predicted response to treatment.
Introduction
Cranial neuralgias are often expressions of neuropathic pain in multiple sclerosis (MS), occurring with a prevalence of 2.26%, which is higher than the general population (1–4). Demyelination is thought to play an important role in the development of neuralgiform pain, as supported by the presence of demyelination of the centrally myelinated part of the trigeminal nerve root of surgical specimens from trigeminal rhizotomy in patients with trigeminal neuralgia and MS (5). The association and prevalence of trigeminal neuralgia in MS has been well documented, with a 20-fold increase when compared to the general population (6).
There is no data regarding the incidence and prevalence of occipital neuralgia in MS (7). There are case reports of occipital neuralgia and the presence of new high cervical demyelinating lesions where treated patients obtained pain relief from high dose intravenous steroids (8–10). However, data is lacking regarding predictors of upper cervical spinal cords lesions or the efficacy of medical and interventional management of occipital neuralgia in MS.
We tested the hypothesis that occipital neuralgia in MS is associated with a high cervical spinal cord lesion (C2-3), identified risk factors leading to the development of occipital neuralgia, and evaluated the efficacy of treatment.
Methods
Study design and patient selection
This study was approved by the Mayo Clinic Institutional Review Board. We retrospectively reviewed the records of 29 patients over the age of 18 diagnosed with both occipital neuralgia and an idiopathic inflammatory demyelinating disease (IIDD) (multiple sclerosis (MS), radiologically isolated syndrome (RIS), clinically isolated syndrome (CIS), acute disseminated encephalomyelitis (ADEM), neuromyelitis optica (NMO), or Balo’s concentric sclerosis) by a neurologist at our institution from January 2001 to December 2014.
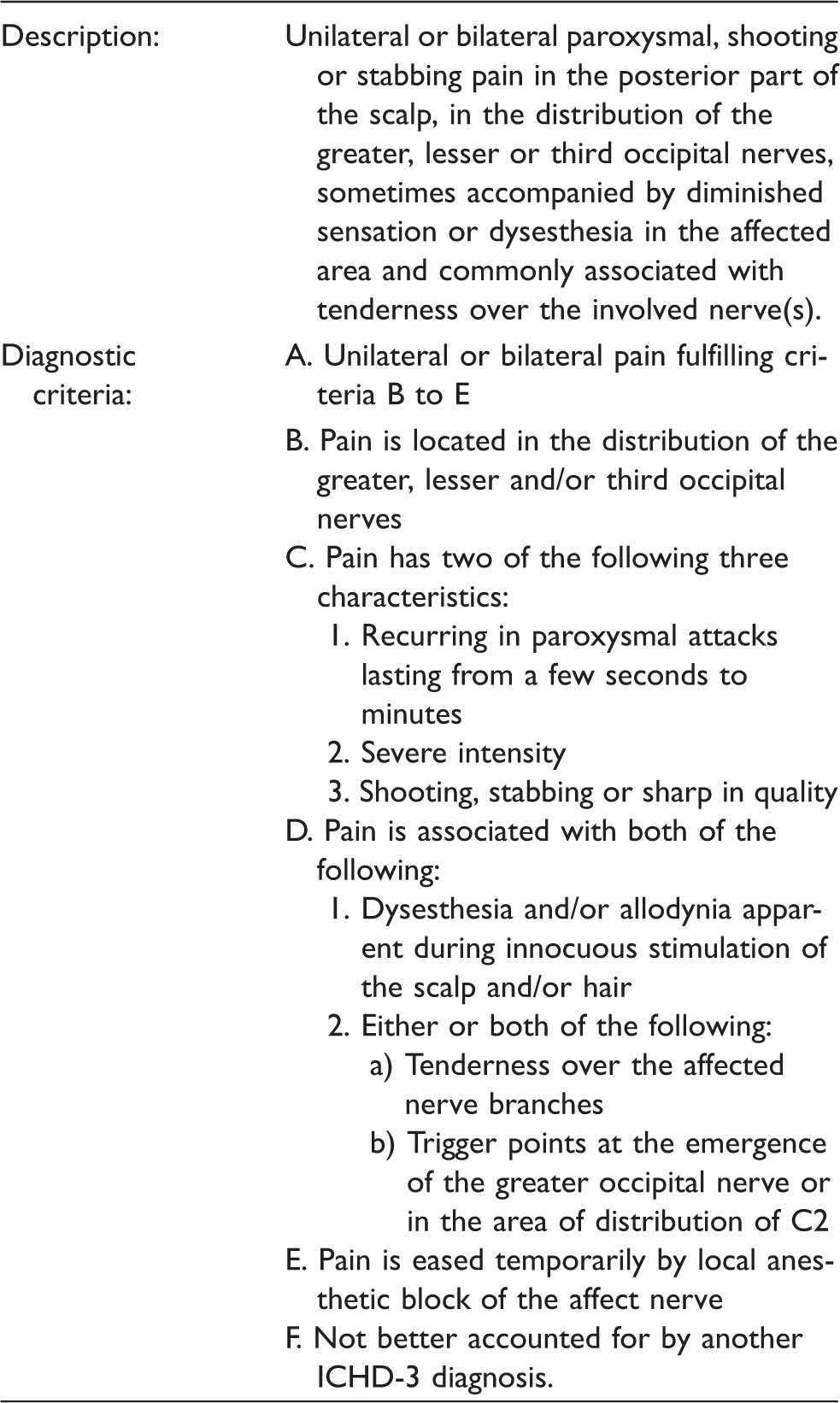
International Classification of Headache Disorders (ICHD-3 beta) diagnostic criteria for occipital neuralgia.
Demographical and clinical data collection
On all patients, we extracted demographics; risk factors for multiple sclerosis; family history; characteristics of pain; age of onset for occipital neuralgia; associated symptoms; prior history of migraine, head and neck surgery or trauma; documented medication overuse (listed as diagnosis); and coinciding trigeminal neuralgia.
The patients were categorized based on clinical phenotype of IIDD. Time to Expanded Disability Status Scale of 6 (EDSS6), (unilateral assistance required to walk 100 m), was recorded in all patients if this endpoint had been reached by the last follow-up (13). For patients with progressive MS diagnosis, the age of progressive MS onset was noted.
Cervical spine imaging including x-rays, CT, and MRI (both radiology interpretation at the time and retrospectively by one of the study investigators (NRK)) was reviewed to determine the presence of moderate to severe degenerative spondylosis, as determined by the radiologist on initial interpretation. The MRIs of the cervical spine were also reviewed for the presence of a C2-3 lesion and corresponding enhancement. The timing of MRI of the cervical spine with onset of occipital neuralgia was taken into account. The presence of coinciding brainstem lesions on MRI was also reviewed.
Data was collected on any treatments for occipital neuralgia including occipital nerve blocks and high dose intravenous (IV) steroids. A good response was defined as pain relief for greater than one month with or without medications (14). Given the small number of patients in our case series (n = 29), descriptive data is presented, but no formal statistical analysis was performed.
Results
Characteristics of patients with progressive multiple sclerosis.

MS: multiple sclerosis; EDSS: expanded disability status scale.
Characteristics differentiated by type of demyelinating disease.

Note: When a variable was not available for all patients, the variable was excluded from the analysis for those cases, which may affect the percentages shown.
^Moderate to severe degenerative changes noted on imaging.
αEnhancement of the C2-3 lesion observed on MRI at any point in the clinical course.
MS: multiple sclerosis; CIS: clinically isolated syndrome; NMO: neuromyelitis optica; RIS: radiographically isolated syndrome; Dx: Diagnosis; ON: occipital neuralgia; TN: trigeminal neuralgia.
All but one patient had MRI imaging available to review. At the time of evaluation, this patient was unable to obtain MRI imaging due to an implanted metallic object in the body. Eighteen of the 28 (64%) patients had a C2-3 demyelinating lesion present on an MRI of the cervical spine obtained as part of the clinical evaluation. The location of the C2-3 lesions correlated to the distribution of pain and no discrepancies were noted between the initial report and retrospective analysis. All of the MS patients with C2-3 lesions had lesions that were 1–2 vertebral segments in length. The patient diagnosed with NMO had a longitudinally extensive lesion from C2 to T5 (nine vertebral segments). The CIS – transverse myelitis group was a heterogeneous group in which the CIS patients (n = 2) had lesions 1–2 segments in length, whereas the transverse myelitis patient (n = 1) had a longitudinally extensive lesion from C2 to C6 (five vertebral segments). All of the patients (n = 3) with documented occipital distribution sensory deficits on examination as part of the clinical evaluation had a C2-3 demyelinating lesion (Table 3).
Three patients had brainstem lesions as well as a history of coinciding trigeminal neuralgia (Table 3). All of the patients with progressive MS (n = 2) or CIS – transverse myelitis (n = 2) without C2-3 lesions had potential alternative causes for occipital distribution neuralgiform pain such as C2 fracture, C1-2 joint instability, prior suboccipital decompression, and severe cervical spondylosis. Of those with C2-3 lesions present on imaging, only five patients had findings of enhancement on MRI suggestive of active demyelination. However, only eight patients had an MRI taken within two weeks of onset of occipital neuralgia (Table 3).
A 52-year-old female with relapse remitting MS had a cervical MRI performed 2 years prior to the onset of occipital neuralgia that did not identify a C2-3 demyelinating lesion. Repeat MRI of the cervical spine obtained within two weeks after onset of occipital neuralgia demonstrated a new demyelinating lesion with enhancement at the level of the dens (Figure 1). This patient was treated with IV methylprednisolone 1 gram daily for three days and had resolution of her occipital distribution pain within two weeks after treatment (Table 4).
(a) T2 sagittal and (c) T1 sagittal post contrast image obtained 2 years prior to onset of occipital neuralgia, demonstrating the absence of any upper cervical demyelinating lesions. (b) T2 sagittal and (d) T1 sagittal post contrast image obtained within 2 weeks of onset of occipital neuralgia, demonstrating a new C2 demyelinating lesion with enhancement. Response to treatment. ^Pain free > 1 month with or w/o medications. αEnhancement of the C2-3 lesion observed on MRI at any point in the clinical course. Note: When a variable was not available for all patients, the variable was excluded from the analysis for those cases, which may affect the percentages shown.

Conversely, a 74-year-old female presented with a 1.5 year history of left occipital neuralgia and a non-enhancing left sided C2 demyelinating lesion at the level of the dens with only mild multilevel degenerative changes in the cervical spine (Figure 2). The patient received a left occipital nerve block with no pain relief. She was treated with carbamazepine up to 200 mg twice daily and had good pain relief, but the dose was limited due to gait imbalance and sedation, ultimately leading her to taper off the medication.
(a) T2 sagittal and (c) T2 axial image obtained 6 months after onset of occipital neuralgia demonstrating a left C2 demyelinating lesion. Repeat imaging 1 year after onset of occipital neuralgia with (b) T2 sagittal and (d) T1 sagittal post contrast images shows persistence of left C2 demyelinating lesion without enhancement.
A total of 14 patients received treatment with either occipital nerve blocks or high dose IV steroids. None of the three progressive MS patients who received either treatment responded (Table 4). All of the other treated patients (n = 8) with either relapse remitting MS (n = 5), RIS (n = 2), or CIS (n = 1) that had long term follow-up responded to occipital nerve blocks or a course of high dose IV steroids (Table 4). The patients who had good responses to occipital nerve blocks (n = 7) with long term follow-up were not treated at onset of occipital neuralgia and did not have enhancement noted on MRI imaging. The presence of a C2-3 lesion did not reliably predict a treatment response, as patients both with (n = 4) and without (n = 3) C2-3 lesions responded to occipital nerve blocks. Three of the patients with relapse remitting MS who received occipital nerve blocks did not have long term follow-up to review treatment responses.
One patient with the comorbid diagnoses of rheumatoid arthritis and static myelopathy (not confirmed as MS related) had C1-2 joint instability with resolution of pain after C1-2 joint arthrodesis. The remaining patients (n = 14) who did not receive treatments with occipital nerve blocks or high dose IV steroids were managed conservatively with medications such as gabapentin, carbamazepine, pregabalin, amitriptyline, nortriptyline, lamotrigine, and/or duloxetine. Nine of the patients who were medically managed had C2-3 lesions. Four (all with C2-3 lesions) of these 14 medically managed patients had resolution of occipital neuralgia (range, 2 weeks to several years after onset of pain). Of the 10 patients who did not have eventual resolution of occipital neuralgia, only one patient with relapse remitting MS had good control of pain with pregabalin, and that patient also had the presence of a C2-3 lesion. The remaining patients either were lost in follow-up or did not have a response with medication management.
Discussion
To our knowledge, this is the largest case series of patients with both occipital neuralgia and IIDD to date. Following strict International Headache Society (IHS) criteria, most of these cases would not technically fulfill criteria for occipital neuralgia, but would fulfill criteria for headache attributed to a non-infectious inflammatory disease (Table 1). The descriptive term of occipital neuralgiform pain (8,9) may be more appropriate for use in IIDD and is the common vernacular of clinicians.
Alternatively, the term painful occipital neuropathy attributed to idiopathic inflammatory demyelinating disease could be used. This would be akin to how trigeminal neuralgia in MS is classified in the current IHS criteria (11) and still the term trigeminal neuralgia has been commonly used in the literature (2,5,6,14–16). Also similar to trigeminal neuralgia, the presence of demyelination of the centrally myelinated part of the nerve root could result in ephaptic transmission of nerve impulses. In addition, occipital neuralgia has been used in the literature to describe cases of occipital distribution neuralgiform pain attributed to secondary causes such as neurosyphillis (17), C1-2 arthrosis (18), cervicomedullary dural arteriovenous fistula (19), upper cervical cavernous angioma (20), and vascular compression (21), with some of the lesions affecting the central nervous system. Based on the above, the term occipital neuralgia was used in this study.
No prior studies have compared the different subtypes of IIDD. Eriksson et al. was the first to report on occipital neuralgia in MS as part of a larger investigation looking into paroxysmal symptoms associated with MS (1). In this study, all cranial neuralgias (trigeminal, intermedius, retroauricular, and occipital neuralgia) were grouped together and from the cohort a reported incidence of 189 per 100,000 MS patients and prevalence of 2.26% was noted for all of these cranial neuralgias. A subgroup analysis for each of the cranial neuralgias was not performed, and minimal demographic data was presented as part of the study.
One of the patients in our study was previously reported, and had C2 myelitis presenting with occipital neuralgiform pain, where resolution of pain coincided with resolution of the C2 lesion on imaging (9). Another case of occipital neuralgia as an isolated symptom related to a C2 demyelinating lesion has also been reported (10). A third case with occipital distribution headache and a C1-2 lesion along with pain in the face, head and neck was reported (22). There is only a single small (three patient) cases series that demonstrated the association of occipital distribution neuralgiform pain and C2 lesions (8). In this study by De Santi et al., all of the patients responded to acute treatment with high dose IV steroid infusions, but minimal demographic and clinic data were able to be compared for predictors of an upper cervical lesion or response to treatment (8).
Most of the patients in our case series had the presence of a C2-3 level demyelinating lesion. It is difficult to confirm the presence of a C2-3 lesion as causative of occipital neuralgiform pain, but the few patients in this series that had prior imaging before onset of pain had interval development of C2-3 lesions associated with the development of occipital neuralgia. When no C2-3 lesion was identified, patients typically had clinical and/or imaging features of an alternative diagnosis such as cervicogenic headache with constant neck pain, C1-2 joint arthropathy and instability, cervical spondylotic changes, or prior suboccipital surgery (23). In keeping with the diagnostic criteria for occipital neuralgia, the presence of a unilateral and episodic pattern of pain predicted the presence of a C2-3 lesion. Sensory loss in the occipital distribution was indicative of a demyelinating lesion and therefore useful in the evaluation of these patients, but was not routinely evaluated in our cohort.
There is evidence that onset of the progressive phase in MS is age-dependent, occurring in the fifth decade of life (24). The majority of our patients typically developed occipital neuralgia after the age of 40. Nearly all of the patients with progressive MS in this cohort had the presence of a C2-3 lesion with the remaining two patients having potentially alternative causes for their occipital distribution pain. Other studies have shown an association between cervical spinal cord lesion load and disability independent of atrophy as well as an association with progressive MS and grey matter involvement in cervical spinal cord lesions (25,26). Based on this, the presence of C2-3 lesions in a majority of progressive MS patients with occipital neuralgia is not surprising. In this case series, the lack of response to treatment with high dose IV steroids and occipital nerve blocks in patients with progressive MS could be explained by the more irreversible neurodegenerative phenotype of progressive MS as opposed to the relapsing-remitting phenotype. In contrast, in non-progressive IIDD phenotypes, despite the similar presence of C2-3 lesions, the observed more favorable response to treatments targeting occipital neuralgia was potentially related to the presence of more intact neurons. Alternatively, since many of our patients had resolution of pain without acute treatments (e.g. IV steroids or occipital nerve blocks), it is also possible that patients without a progressive phenotype could have improved independently of treatment.
Occipital neuralgia can present as the initial heralding symptom of IIDD, and a cervical spine MRI can be helpful as part of the evaluation of occipital neuralgia to exclude secondary causes. Our findings in this case series support the association of occipital neuralgia with MS, much like the association of trigeminal neuralgia with MS. If patients with MS present with pain suggestive of occipital neuralgia, then an MRI of the cervical spine should be obtained to look for the presence of a demyelinating lesion or potential alternative causes of occipital distribution pain such as cervicogenic headache. Potential predictors of the presence of an upper cervical spinal cord lesion were unilateral episodic symptoms, sensory loss, onset occurring later in life (age > 40), and progressive MS phenotype. Occipital nerve blocks may be a therapeutic option with an isolated pain presentation (without neurological deficits) in order to spare the patient from side effects related to high dose IV steroids. More proximal image guided nerve blocks, such as ultrasound guided occipital nerve blocks at the level of C2 (27), could be considered for those patients with C2-3 lesions that did not respond to traditional landmark guided occipital nerve blocks and high dose IV steroids.
Footnotes
Clinical implications
If patients present with pain suggestive of occipital neuralgia, then an MRI of the cervical spine should be obtained to look for the presence of demyelinating lesions or alternative causes of occipital distribution pain.
Unilateral episodic symptoms, sensory loss, onset occurring later in life (age > 40), and progressive MS phenotype predict upper cervical spinal cord lesions in MS.
Occipital nerve blocks may be a therapeutic option with isolated pain presentations in MS.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.