
Abstract
Background and aim
Factors implicated in the evolution of episodic migraine into chronic migraine are largely elusive. Medication overuse is considered to be one of the main determinants, but other possible clinical and psychological factors can play a role. The aim of this study is to identify factors that are associated with chronic migraine with medication overuse.
Method
We enrolled consecutive migraine patients, subdividing them in two groups: Subjects with a long history of episodic migraine and subjects with chronic migraine and medication overuse. We then compared their clinical and psychological variables in a cross-sectional study.
Results
Three hundred and eighteen patients were enrolled, of which 156 were episodic migraine and 162 were chronic migraine and medication overuse patients. The mean age was 42.1 ± 10.3, 80.8% were female. The duration of migraine was 24.6 years in episodic migraine and 24.0 years in chronic migraine and medication overuse (p = 0.57). After the multivariate analysis, the factors associated to chronic migraine and medication overuse were: Marital status (married vs. unmarried, OR 3.65, 95% CI 1.63–8.19, p = 0.002; separated/divorced/widowed vs. unmarried, OR 4.19, 95% CI 1.13–15.47, p = 0.031), physical activity (OR 0.42, 95% CI 0.19–0.91, p = 0.029), age at onset of migraine (OR 0.94, 95% CI 0.89–0.98, p = 0.016), use of at least one migraine preventive medication (OR 2.36, 95% CI 1.18–4.71, p = 0.014), history of depression (OR 2.91, 95% CI 1.25–6.73, p = 0.012), insomnia associated with the use of hypnotics (OR 5.59, 95% CI 1.65–18.93, p = 0.006), traumatic head injuries (OR 3.54, 95% CI 1.57–7.99, p = 0.002), snoring (OR 2.24, 95% CI 1.05–4.79, p = 0.036), previous and/or actual use of combined oral contraceptives (OR 3.38, 95% CI 1.10–10.3, p = 0.031) and higher scores in the Childhood Trauma questionnaire (OR 1.48, 95% CI 1.09–2.02, p = 0.012).
Conclusion
We considered several aspects that may be involved in the development of chronic migraine and medication overuse. A multivariate analysis identified 10 factors belonging to five different areas, to suggest that chronic migraine and medication overuse onset is likely influenced by a complex mixture of factors. This information is useful when planning strategies to prevent and manage chronic migraine and medication overuse.
Keywords
Introduction
Chronic Migraine (CM) is frequent, and represents a disorder with a high socio-economic burden (1). CM is often associated with medication overuse (MO), thus configuring the double diagnosis of CM + medication overuse headache (MOH), according to ICHD-3beta (2), which further increases the associated costs. MO does have a causal role in the development of CM, as demonstrated by scientific evidence showing that the increasing use of symptomatic medication is associated to the progressive worsening of migraine (3,4).
However, the reason why some migraine patients start overusing acute medications and evolve into chronic migraine and medication overuse (CM-MO) while others do not is largely elusive. Moreover, the distinctive features of the subgroup of migraine patients who will go on to develop CM-MO are largely unknown. The comparative analysis of sociodemographic data, family, physiological and medical history, acute medication and use of healthcare resources in EM and CM has been the object of a previous study (5). Unfortunately, the findings obtained do not grant reliable conclusions in light of some methodological issues such as: i) the duration of illness between EM and CM groups was not comparable, a discrepancy that does not allow an effective analysis of the evolution toward a chronic form of migraine in some of the subjects belonging to the episodic group, and ii) researchers did not perform a multivariate analysis among all the variables.
Our central hypothesis is that the transformation of EM into CM-MO occurs in predisposed patients in whom the predisposition results from a critical combination of a set of clinical factors. Accordingly, the objective of the present study is the identification of the factors that are associated with CM-MO. The achievement of this objective will contribute to the identification of a subpopulation of patients who are at a high risk of negative outcomes. Our findings will also shed light on the pathophysiological mechanisms of MOH.
Subjects and methods
Subjects
This study was conducted at the Pavia Headache Center (a tertiary referral center) of the C. Mondino National Neurological Institute in Pavia, Italy. We enrolled consecutive patients with long-term episodic migraine (EM, history of illness >10 years who never developed MO) and patients with CM-MO. The study was approved by the Local Ethics Committee (on 5 March 2014) and informed consent was obtained from all patients. Recruitment started in March 2014 and was completed in July 2016. All consecutive EM and CM-MO patients were enrolled. EM patients were enrolled in headache clinics; CM-MO patients were enrolled either in headache clinics or (in the majority of cases) during the inpatient detoxification program.
EM patients
Inclusion criteria for patients with EM were: i) age >18, < 65 years, ii) fulfilment of ICHD-3 criteria for migraine with or without aura, iii) migraine duration ≥10 years. Exclusion criteria were: i) previous or present history of MO or any other type of chronic headache (ICHD-3 beta), ii) dementia iii) psychosis iv) mental retardation.
CM-MO patients
Inclusion criteria for patients with CM-MO were: i) age >18, < 65 years, ii) fulfilment of ICHD-3 beta criteria for CM and MOH. Exclusion criteria were: i) dementia, ii) psychosis, iii) mental retardation.
Procedures
Each consultation was performed by a neurologist with long-standing experience in headache management (NEH). NEHs diagnosed the headache type, collected socio-demographic data, lifestyle habits, migraine characteristics and history, an accurate history of present and previous use of medications and/or other substances, a medical history, an obstetrical and gynaecological history and a family history. We assessed how physically active the patient was by asking “do you engage in physical activity (any activity implying active body movement that requires more energy than resting for at least 30 minutes) regularly at least once a week every week?”. Snoring was assessed through subjective accounts by the patient and his/her partner. The number of head injuries were ascertained by combining subjective accounts from the patients with consultation of medical records. Psychological variables were collected by specific self-administered questionnaires that included: i) Toronto Alexithymia Scale (TAS-20) (6) for the detection of alexithymia, a personality trait characterized by the inability to identify and express emotions; TAS-20 uses a five-point Likert response scale and has a three-factor structure consisting of difficulty in identifying feelings (F1), difficulty in describing feeling (F2) and externally oriented thinking (F3); ii) Leeds Dependence Questionnaire (LDQ) (7,8), which measures dependence upon every substance, exploring systematically ICD-10 diagnostic criteria for defining dependence; iii) Hospital Anxiety and Depression Scale (HADS) (9,10) for the quantification of state levels of anxiety and depression in the last seven days; iv) Childhood Trauma Questionnaire (11,12), a screening measure for maltreatment histories; a shorter version was used that includes 13 items referring to different types of childhood trauma such as emotional abuse, emotional neglect, physical abuse, physical neglect, and sexual abuse; for each item patients were requested to indicate whether or not they experienced each kind of trauma; the total score is derived from the sum of traumatic events experienced; v) stressful life-events questionnaire, which consists of a list of 58 stressful life events adapted by Paykel et al. in their article (13); the patient was asked to tick those that occurred to him/her in the last 10 years; the total score is derived from the sum of stressful life events indicated.
Statistical procedures
Data are presented as mean ± standard deviation for continuous data and as n/% for categorical data.
All analyses were carried out with logistic regressions. From the regressions, we derived ORs as estimates of the strength of association with CM-MO, the 95% CI of ORs, and the level of statistical significance.
The method of analysis was developed along three subsequent steps. Firstly, all the considered variables were entered into an unadjusted univariate analysis, and the statistical significance and OR with 95% CI of the association to CM-MO were calculated. Secondly, a multivariate analysis was carried out within each group of variables: Socio-demographic/lifestyle factors, migraine characteristics/history, obstetrical-gynaecological history (limited to women), familial pathological history, medical history, and psychological tests. In this analysis, we considered only those variables that were associated with CM-MO in the univariate analysis with a statistical significance of p < 0.10. Thirdly, a final multivariate analysis was carried out among those variables that reached a statistical significance of p < 0.10 in the first multivariate analysis. We considered those variables that had a p value below 0.05 to be statistically significant. Finally, due to the relevance of gender in the occurrence of migraine and due to the reasonable expectation that gender could act as a risk modifier of CM-MO, we conducted a separate analysis of female and male populations for the variables that were statistically significant in the final multivariate analysis.
All analyses were conducted using the Statistical Package for Social Sciences (SPSS) version 24.
Results
Patient population
Three hundred and eighteen patients were enrolled, of which 156 suffered from EM and 163 from CM-MO. One patient in the CM-MO group was excluded because of evidence of a probable secondary headache (headache associated to chronic infection). No EM patients were excluded. Six EM and five CM-MO patients who met inclusion criteria were not enrolled as they refused to fill in the questionnaires. Two CM patients were not enrolled because they did not fulfil the criteria for Medication Overuse Headache. All CM-MO patients enrolled had a previous multi year history of EM.
EM patients
Patients had the following characteristics: 81% were female (n = 126), average age was 40.3 ± 10.8 (range: 20–64), the average age at onset of migraine was 15.7 ± 7.5 (range: 3–40). The average monthly frequency of attacks of migraine without aura was 6.0 ± 3.0 (range: 1–14). Twenty patients (12%) also had attacks of migraine with aura.
CM-MO patients
Patients had the following characteristics: 81% were female (n = 131), average age was 43.7 ±9.5 (range: 18–66), the average age at onset of migraine was 13.2 ± 6.2 (range: 3–40), the average age at onset of CM-MO was 37.0 ± 9.0 (range 15–60). Twenty-five patients (15%) also suffered from migraine with aura.
The average frequency of headache days per month was 26.1 ± 4.6 (range 15–30), the average frequency of days of medication intake per month was 23.9 ± 5.6 (range 12–30), the average frequency of medication use per month was 45.8 ± 37.8 (range 12–30). Overused medications were: Triptans in 21 patients (13.0%), simple analgesics in 51 (31.5%), combination-analgesics in 12 (7.4%), and multiple drug classes in 78 (48.1%). None of the patients qualified for ergotamine-overuse headache or opioid-overuse headache. Sixty two patients (38.3%) had previously undergone at least one detoxification program: 60 underwent inpatient detoxification (average of 2.1 ± 1.4, range 1–7) and 12 underwent day hospital detoxification (average of 1.6 ± 0.7, range 1–3).
Factors associated to CM-MO
Univariate and multivariate logistic regression equations performed for predicting the tendency to be a CM-MO versus EM patient.
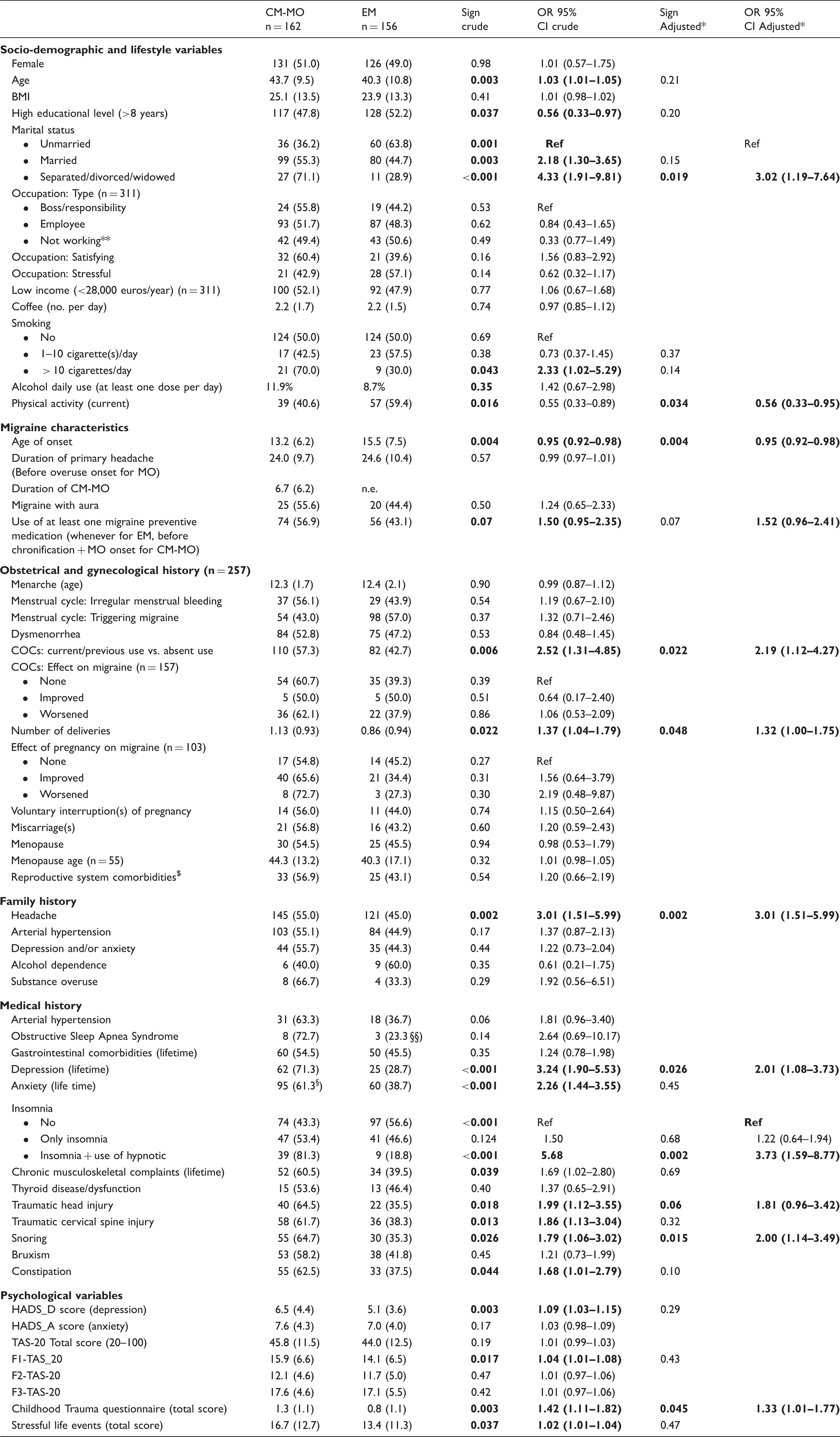
This multivariate analysis was carried out within each group of variables: Socio-demographic/lifestyle, migraine characteristics/history, obstetrical-gynaecological history (limited to women), familial pathological history, medical history, and psychological tests. Data are presented as means ± standard deviations for continuous data, and as n/% for frequency data (percentages refer to the rows).
Adjusted for variables of the same group with p < 0.10 at the univariate; **not working: housewife, retired, unemployed, students.
COC: combined oral contraceptive; $: Uterine fibroids, uterine polyps, endometriosis, ovarian cysts (no significant differences were found of each of these pathologies between EM and CM-MO); HADS: Hospital Anxiety and Depression Scale; TAS: Toronto Alexithymia Scale. F1-TAS20: Difficulty identifying feelings subscale. F2-TAS20: Difficulty describing feelings subscale. F3-TAS20: Externally oriented thinking subscale. Note: In bold, data referred to variables that reached a statistical significance (p < 0.05) in such analysis.
Second multivariate logistic regression equations performed for predicting the tendency to be a CM-MO versus EM patient.
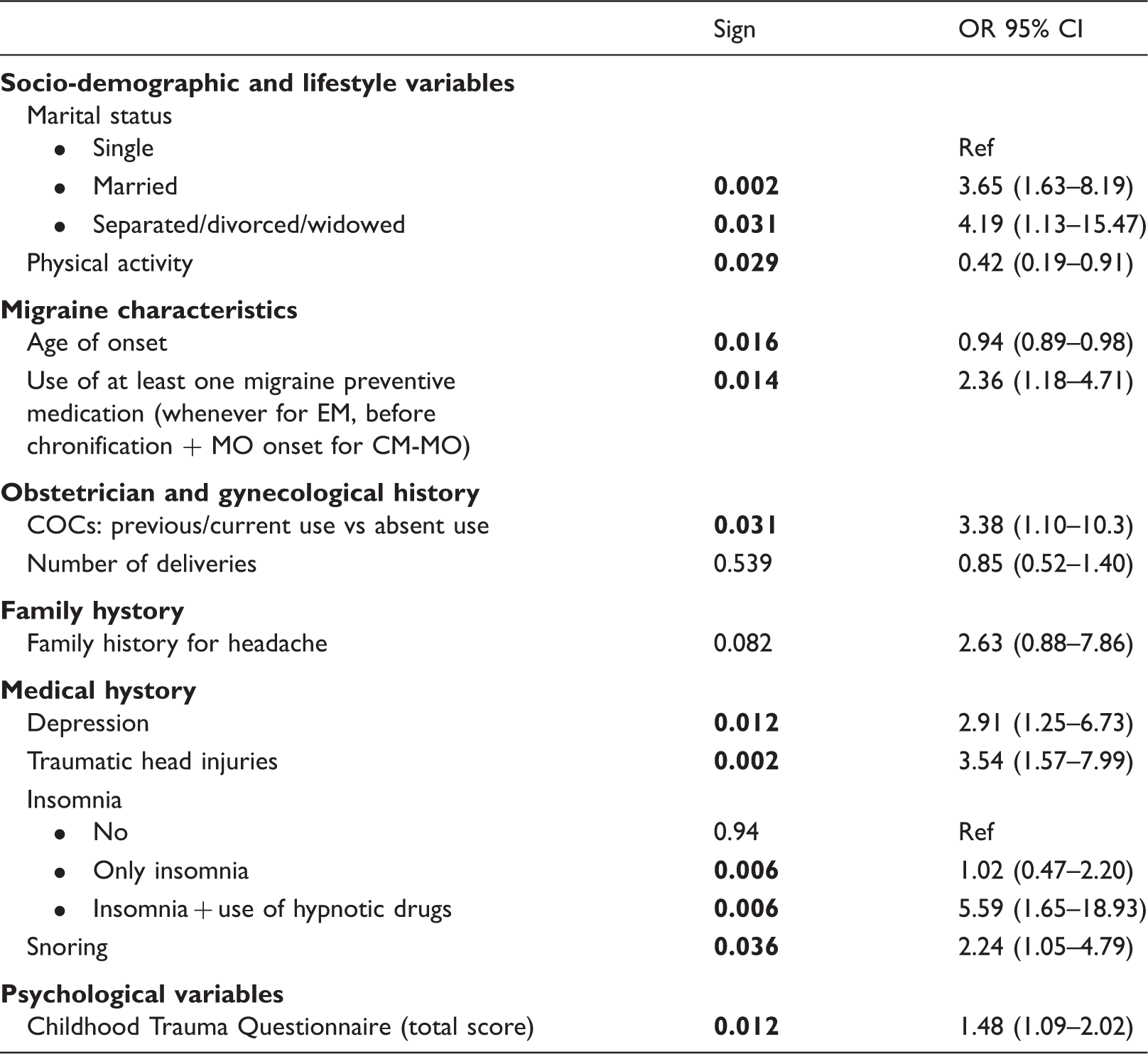
This multivariate analysis was carried out among those variables that reached a statistical significance with p < 0.10 in the first multivariate analysis (Table 1). COC: combined oral contraceptive. The two variables with a p < 0.10 in the multivariate analysis in obstetrical/gynecological history were tested in this model only within the female population without reaching the significance level of p < 0.05. Note: In bold, data referred to variables that reached a statistical significance (p < 0.05) in such analysis.
Discussion
CM-MO is frequent, and it represents a costly chronic headache with a high socio-economic burden (1). The precise mechanisms involved in the progression from an episodic to a chronic pattern associated with MO are elusive. Here we report data from a study involving 318 long-term migraine sufferers, of which 162 developed CM-MO while 156 did not.
The first notable finding of our study is that the duration of migraine was similar between the two groups. This result was likely facilitated by the inclusion criteria selected for the EM group, which only included patients suffering from migraine for >10 years; however, we believe this was vital to control for the possibility to include subjects with EM who would have converted to CM-MO later in the course of their disorder. Unfortunately, this particular caution was not taken in other cross-sectional studies (5).
The multivariate analysis allowed the identification of 10 factors associated to CM-MO (Table 2). On the basis of the current literature, some of these factors were “expected”, such as physical inactivity, use of at least one migraine preventive medication, history of depression, insomnia, traumatic head injury, snoring and trauma in childhood. On the other hand, there were some unexpected factors, such as marital status (married or separated/divorced/widowed marital status vs. single) and age at onset of migraine (younger). Surprisingly, we did not note a correlation with gender, BMI, coffee, alcohol, smoking, obstetrical history, and family history of migraine (although the latter was close to the level of significance, p = 0.082). Furthermore, the reported association of COCs use with CM-MO showed an opposite correlation to what was previously described (5).
Although the cross-sectional design of the study does not warrant accurate conclusions as to which of these factors indeed have a causative role in the development of CM-MO, the findings highlight those factors that are likely to be a consequence of CM-MO (or of the process of its development) instead of a cause, while others are more likely to play a causal role.
Socio-demographic and lifestyle variables
Marital status
A married or separated/divorced/widowed status was more common in CM-MO (three to fourfold). In the univariate analysis, CM-MO patients showed a higher age (by 3 years), yet the variable age lost statistical significance after multivariate analysis. Therefore, the marital status itself is likely to enclose particular clues linked to CM-MO. This finding may have a dual explanation: Being married brings along responsibilities and duties that may increase the stress workload on the patients, thus triggering more attacks; on the other hand, the need to perform tasks may lead to more frequent use of acute medications.
Physical activity
The low percentage of CM-MO patients performing regular physical activity (PA) could be a consequence of the disease on physical function, as it is quite difficult to practice PA during migraine attacks. Also, in our study the “regular practice of physical activity” referred only to the recent period. On the other hand, PA is shown to be effective in reducing the frequency of migraine attacks (16). One prospective study found that physical inactivity doubled the risk of MOH after 11 years (17). If further observational studies are conducted, it would be useful to know: i) if the patients engaged in physical activity before the onset of CM-MO and, if this was the case, the chronological aspects in relation to migraine history (migraine onset, chronification, medication overuse); ii) which type of physical activity, frequency and intensity of training patients engaged in.
Migraine characteristics
Age of onset and familiarity for headache
Our results show that CM-MO patients had a lower age at the onset of migraine with respect to EM patients (−2.3 years). To better contextualize this finding, it is important to note that the earlier onset is not associated with the fact that patients had more time to develop CM-MO as, at least in our sample, the duration of primary headache (migraine) was similar in the two groups (24 years). The lower age of onset of migraine in the CM-MO group may be due to the fact that these patients may have been more prone to manifest migraine, which starts earlier in life (closer to puberty), and had more frequent attacks (17). In this scenario, patients are driven to use symptomatic medications more frequently and hence are at a higher risk of developing MO.
Migraine preventive medications
One of the variables that is likely a consequence of the process leading to CM-MO is the previous use of migraine preventive medications. Headache frequency has emerged as the strongest risk factor for the development of MOH (17). Thus, the higher frequency of migraine attacks in the CM-MO group has probably prompted physicians to prescribe preventive medications, which explains the present finding. It is interesting to note that, although around half of CM-MO had previously tried preventive medications before chronification, they nonetheless evolved toward CM-MO. This observation introduces another potential risk factor for CM-MO: The possibility that these patients have a poorer response than the EM group to preventive therapy. Indeed, we attempted to collect this information by asking patients whether at least one preventive medication was effective in the past. Unfortunately, 50% of the data were ultimately missing as i) some patients did not use any preventive medication, ii) some could not recall the effect of the treatment, iii) others did not use the preventive medication with proper dosage, duration of treatment and compliance. It is likely that the issue of poor responsiveness to medications (preventive and/or symptomatic (18)) may be linked to medication overuse. Accordingly, it is worth noting that a recent study involving more than 5,000 subjects showed that ineffective acute treatment doubled the risk for migraine chronification compared with effective acute treatment (19).
Medical history
Depression
Our data show that a history of depression (but not current depression) is associated with a threefold risk of being a CM-MO patient. Two prospective, population-based studies showed that depression confers a higher risk of developing CM (20) and MOH (17). Reproduction of the same finding in large prospective studies seems to weaken the hypothesis that depression is, in the majority of cases, a consequence of MOH. Nevertheless, symptoms of depression may influence pain-coping abilities and encourage frequent use of analgesics. In the latter case, depression represents a causal factor of MOH, yet it is also possible that depression and CM-MO share a common biological background. It is known that alterations in neurotransmitters that play a role in pain are present in depression (21), and they may of course play a role in the chronification of migraine. As such, it is interesting to contemplate whether CM-MO and depression share susceptibility genes. Although no shared genes between MOH and psychiatric disorders have convincingly been demonstrated so far, a previous study by our research group (22) showed that a subgroup of MOH patients who did not respond to detoxification carried a specific catechol-O-methyltransferase gene polymorphism. This finding seems particularly relevant when considering that the same polymorphism is associated with major depression disorder (MDD) (23). We have also demonstrated in a population of MOH that specific polymorphisms of the serotonin 5HT2A receptor and serotonin transporter gene SLC6A4 are associated respectively to a higher number of symptomatic drug doses (and therefore possibly to drug-seeking behaviour in these patients) (24) and to a higher number of monthly days of headache (and therefore with a more severe disease) (25). Also in this case, 5-HT-related gene polymorphisms are known to be related to the pathogenesis of MDD (26).
With respect to the association with anxiety, Hagen et al. (17) reported that depression was associated to a twofold increase in the risk of developing MOH in patients who also suffered from anxiety (OR for depression = 2.6). In our study, using the univariate analysis we found a significant difference (p < 0.001) for anxiety (lifetime) between CM-MO and EM patients with a crude OR of 2.26 (95% CI 1.44–3.55) toward CM-MO. This significance disappeared at the first multivariate analysis that included other variables of medical history (p = 0.45, OR 1.22, 95% CI 0.71–2.09) (Table 1). It is worth noting that Hagen and colleagues adjusted the OR of anxiety only for a few variables (age, gender, education and headache frequency). When we analysed our data, adjusting the OR of anxiety for the same four variables, it remained statistically significant (p = 0.002, OR 2.0, 95% CI 1.30–3.29). However, when we added depression to anxiety and these four variables in the multivariate analysis, anxiety lost its statistical significance (p = 0.07, OR 1.57, 95% CI 0.96–1.59). Therefore, it is possible that the association between anxiety and MOH found by Hagen et al. is actually due to the co-occurrence of depression.
Head injury
Our results show that head injury was associated with MOH with an OR of 3.5. Couch and colleagues reported a relationship between head and neck injury (HANI) and chronic daily headache (CDH) (where the majority of subjects had migraine), which was not limited to injuries proximate to CDH onset (27). Moreover, they showed evidence that the lifetime risk of CDH increases with the increasing number of HANIs, and that the number, but not severity, of HANIs was a risk factor for CDH. From a pathophysiological perspective, it has been postulated that HANI may modify central mechanisms, including perturbation of pain-related structures such as the periaqueductal grey (28,29) that are implicated in the pathophysiology of migraine and MOH.
Insomnia
With regards to insomnia, our results show that only insomnia severe enough to require the use of hypnotics is associated with CM-MOH, with an OR of 5.5. This finding agrees with the results of the prospective study by Hagen and colleagues (17), where they found that only severe insomnia was associated with the risk (OR 1.9) of developing MOH, and with those of another such study (30).
Regarding the mechanisms for the relationship between insomnia and CM or MOH, experimental studies have shown that total and selective sleep deprivation (31) as well as disrupted sleep continuity (32) leads to hyperalgesia in healthy subjects, possibly because sleep loss causes a transient disturbance of the descending pain inhibitory control system (33). An alternative theory is that sleep disruption leads to an increase in inflammatory mediators like IL-6, which may sensitize several types of nociceptors (34,35). Interestingly, behavioural sleep modification proved effective in reducing the frequency and intensity of chronic headache (36).
Snoring
In our sample, snoring was also associated with CM-MO (OR 2.2). Snoring has a high prevalence in chronic headache patients with respect to the episodic forms (48.6% vs. 37.2%, respectively) according to the findings in an Italian study (37). Snoring may thus represent an independent risk factor for increasing migraine frequency, thus laying the ground for an increased need for symptomatic medications.
Obstetrical and gynaecological history
Previous and/or current use of COCs
In our female population, the current/previous use of COC was associated with the risk of CM-MO. This finding is in line with the data from the literature, which in general suggest a worsening effect of COC on migraine. In a previous study on EM and CM, Ferrari et al. found the opposite association (5); however, in their study the group of CM was 13 years older than the EM group, and the association was not adjusted for age. Thus, methodological issues may have confounded the finding.
Psychological variables
Childhood trauma
Our data shows that childhood trauma is associated with MOH. It is increasingly known that psychosocial variables play key roles in conferring a risk for the development of pain, in shaping long-term pain-related adjustment, and in modulating pain treatment outcomes (38). In particular, strong prospective links have been observed between early traumatic experiences and the subsequent development of chronic pain (39–41). It should be noted that many of the traumatic experiences reported are social and interpersonal in nature. It is likely that occurrence of such trauma in genetically predisposed children during an extremely vulnerable period of life is able to change the pain modulating system. Our finding is in agreement with a previous study specifically aimed at investigating the association of childhood trauma with migraine (42), where the authors found a higher risk of developing CM in patients with a history of child abuse.
Other factors
Other studies have identified factors associated to CM-MO that were not confirmed in the present investigation. Hagen and colleagues (17) found an association between MOH and musculoskeletal complaints. In our population, “musculoskeletal chronic pain symptoms” were associated with CM-MO in the univariate analysis, but the association was not confirmed in the subsequent multivariate evaluation. It is possible that the discordance is related to dissimilar terms used in the two studies: “musculoskeletal chronic pain symptoms” may include fewer pathological conditions with respect to “musculoskeletal complaints”.
The same Norwegian study found smoking as a risk factor for MOH (17), a finding that was not confirmed in our study. The two studies are methodologically different, since the Norwegian study was prospective, while ours is cross-sectional. This factor alone may explain the discrepancy, since Hagen et al. may have captured smoking in the very process of evolution from EM to CM, while our population, suffering CM over several years, could have quit smoking before participation. In everyday practice, many migraine patients report that they avoid smoking during attacks due to osmophobia, and cigarette smoke is indeed one of the smells that can be used to evaluate osmophobia at the bedside (43).
Low socioeconomic status was found to be associated with chronic headaches in general (migraine and non-migrainous) (44). The difference in the terms used for these diseases and for our groups makes it difficult to compare the data with our findings.
In the study by Ferrari and colleagues (5), associations with many variables were found with chronic migraine/MOH versus episodic migraine. Some of those variables were confirmed in our study (marital status, constipation and use of hypnotics – the latter two only in the univariate analysis), whereas others were not (lower levels of education, unemployment, migraine remission during pregnancy, pregnancy, no use of oral contraceptives, menopause). There are a number of limitations in Ferrari’s study that suggest caution when interpreting their results. Firstly, the age difference between episodic migraine patients and the MOH group was 13 years, which is significant. Data on the duration of migraine before overuse in the MOH group was not reported, thus it is not possible to compare the duration of primary headache between the two groups. Consequently, it is not possible to reasonably rule out that a portion of episodic migraine patients would not have evolved into MOH in the next few years. Finally, a multivariate analysis was not performed.
Medication overuse: Cause or consequence of migraine chronification?
Repeated intake of acute drugs is one of the major risk factors for developing CM (3,4,45–51), and many mechanisms have been suggested for this phenomenon (52). The fact that withdrawal/detoxification procedures are capable of reinstating the episodic pattern in the large majority of subjects (46,53) strongly supports a causative role. On the other hand, another strong risk factor for migraine chronification is the number of headache days (17), and one third of patients undergoing withdrawal/detox do not revert to EM (54), thus it is also possible that MO in a relevant portion of subjects might be associated with CM simply as a consequence of the increasing frequency of attacks rather than being the cause of chronification. Some of the risk factors found here plausibly relate to medication behaviour, whereas others are more likely related to the underlying natural history of migraine progression.
Use of at least one migraine preventive medication might relate to the first aspect, while age at onset of migraine, snoring, traumatic head injuries, previous and/or actual use of combined oral contraceptives and physical activity may relate to the latter, and higher scores in the Childhood Trauma questionnaire, marital status, history of depression, and insomnia associated with the use of hypnotics might relate to both.
Limitations of the study
A major limitation of this study is the cross-sectional observational design used to evaluate the susceptibility of migraine patients evolving toward CM-MO. A prospective design would have yielded more conclusive findings, but prospective studies are very onerous in terms of economic and human resources and, in the case of CM-MO, a very long period of observation would be required in order to collect data for the same population size evaluated in the present study. The only prospective study conducted so far (17) was very valuable for the long follow-up, but was hindered by the fact that the data collected were based on questionnaires, rather than on face-to-face consultations or physician-checked headache diaries, and that non-migrainous chronic headaches were also included. Furthermore, the authors evaluated only a limited number of variables and the OR was adjusted only for three socio-demographic factors and the headache frequency. A multivariate logistic regression including all the variables was not performed. Another possible limitation of the present study is the limited level of detail used in the collection of data for some variables (i.e. previous engagement in physical activity, type of activity, time relationship with different phases of CM-MO development). This was partly due to the awareness that asking patients to commit to too much can lead to a refusal to participate. Patients had to complete questionnaires for around 40 minutes and undergo an accurate clinical evaluation, which already requires a high level of compliance.
Moreover, the use of self-administered questionnaires for collecting psychiatric variables may represent a weakness of the study, given that patients might be less precise when completing it alone as opposed to being directly interviewed. Unfortunately, interviewer-administered questionnaires are time consuming and expensive, and consequently self-administered questionnaires represent an acceptable compromise in the case of studies conducted on large populations.
Conclusion
CM-MO is a highly disabling and costly type of chronic headache. The mechanisms behind the development of CM-MO in a given population of migraineurs are unknown.
In this study, we evaluated a high number of variables and identified socio-demographic/lifestyle factors, as well as medical, gynaecological and psychological ones, that are associated to CM-MO. A longitudinal study is necessary to confirm the role of these factors. Once the causal relationship is ascertained, the identification of migraine patients at risk of developing CM-MO via clinical features will allow the development of specific training programs, follow-up programs and prevention strategies to minimize the risk of chronification and drug overuse, and therefore contain its social and economic burden.
Clinical implications
We analysed several aspects that may be involved in the development of chronic migraine with medication overuse (CM-MO). A multivariate analysis identified ten factors: Age of onset of migraine (earlier), use of at least one migraine preventive medication, marital status (married or separated/divorced/widowed marital status vs. unmarried), physical inactivity, history of depression, insomnia (associated to use of hypnotics versus absence of insomnia), previous traumatic head injuries, snoring, use of combined oral contraceptives (previous/current use vs. absent use) and childhood traumas. These factors belong to five different areas (migraine history, socio-demographic/lifestyle habits, medical history, gynaecological and psychological factors), meaning that CM-MO develops from a mixture of factors. This fact is useful to know, as CM-MO can be prevented by different perspectives and strategies.
Supplemental Material
Supplementary Tables -Supplemental material for Factors associated to chronic migraine with medication overuse: A cross-sectional study
Supplemental material, Supplementary Tables for Factors associated to chronic migraine with medication overuse: A cross-sectional study by Michele Viana, Sara Bottiroli, Grazia Sances, Natascia Ghiotto, Marta Allena, Elena Guaschino, Giuseppe Nappi and Cristina Tassorelli in Cephalalgia
Footnotes
Acknowledgements
This study was carried out in collaboration with UCADH (University Consortium for Adaptive Disorders and Head pain), University of Pavia, Italy. We would like to thank Professor M Musicco (Italian National Research Council – Institute for Biomedical Technologies, Milan, Italy) for his help in the data analysis, and Dr Farihah Khaliq for her support in editing the language.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants of the Italian Ministry of Health to RC 2013-2015 to C. Mondino Institute, Pavia, Italy.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.