
Abstract
Studies suggest that a substantial proportion of headache sufferers presenting to headache clinics may overuse acute medications. In some cases, overuse may be responsible for the development or maintenance of a chronic daily headache (CDH) syndrome. The objectives of this study are to evaluate patterns of analgesic overuse in patients consulting a headache centre and to compare the outcomes in a group of patients who discontinued medication overuse to those of a group who continued the overuse, in patients with similar age, sex and psychological profile. We reviewed charts of 456 patients with transformed migraine (TM) and acute medication overuse defined by one of the following criteria: 1. Simple analgesic use (> 1000 mg ASA/acetaminophen) > 5 days/week; 2. Combination analgesics use (caffeine and/or butalbital) > 3 tablets a day for > 3 days a week; 3. Opiate use > 1 tablet a day for > 2 days a week; 4. Ergotamine tartrate use: 1 mg PO or 0.5 mg PR for > 2 days a week. For triptans, we empirically considered overuse > 1 tablet per day for > 5 days per week. Patients who were able to undergo detoxification and did not overuse medication (based on the above definition) after one year of follow-up were considered to have successful detoxification (Group 1). Patients who were not able to discontinue offending agents, or returned to a pattern of medication overuse within one year were considered to have unsuccessful detoxification (Group 2). We compared the following outcomes after one year of follow-up: Number of days with headache per month; Intensity of headache; Duration of headache; Headache score (frequency x intensity). The majority of patients overused more than one type of medication. Numbers of tablets taken ranged from 1 to 30 each day (mean of 5.2). Forty-eight (10.5%) subjects took > 10 tablets per day. Considering patients seen in the last 5 years, we found the following overused substances: Butalbital containing combination products, 48%; Acetaminophen, 46.2%; Opioids, 33.3%; ASA, 32.0%; Ergotamine tartrate, 11.8%; Sumatriptan, 10.7%; Nonsteroidal anti-inflammatory medications other than ASA, 9.8%; Zolmitriptan, 4.6%; Rizatriptan, 1.9%; Naratriptan, 0.6%. Total of all triptans, 17.8%. Of 456 patients, 318 (69.7%) were successfully detoxified (Group 1), and 138 (30.3%) were not (Group 2). The comparison between groups 1 and 2 after one year of follow-up showed a decrease in the frequency of headache of 73.7% in group 1 and only 17.2% in group 2 (P < 0.0001). Similarly, the duration of head pain was reduced by 61.2% in group 1 and 14.8% in group 2 (P < 0.0001). The headache score after one year was 18.8 in group 1 and 54 in group 2 (P < 0.0001). A total of 225 (70.7%) successfully detoxified subjects in Group 1 returned to an episodic pattern of migraine, compared to 21 (15.3%) in Group 2 (P < 0.001). More rigorous prescribing guidelines for patients with frequent headaches are urgently needed. Successful detoxification is necessary to ensure improvement in the headache status when treating patients who overuse acute medications.
Introduction
Chronic daily headache (CDH), defined as headaches occurring more than 15 days a month (or 180 days a year) for more than 4 h a day, is one of the more frequently seen headache syndromes at tertiary care centres worldwide (1–3). It represents up to 70% of the initial diagnoses seen in centres specifically devoted to headache management in the U.S (4). In population-based surveys, the prevalence of primary CDH is about 4% (5).
Transformed migraine (TM) is the most common type of CDH in the specialty care (1, 3, 4). Subjects with TM usually report a process of transformation over months or years, and as headache increases in frequency, associated symptoms become less severe and frequent. The process of transformation frequently ends in a pattern of daily or nearly daily headache that resembles chronic tension-type headache, with some attacks of IHS migraine superimposed (1, 3, 4).
Risk factors for the development of TM include depression (6, 7), stressful life events, such as divorce, widowhood, separation and problems with children (8), hypertension (9, 10), alcohol overuse (11) hypothyroidism (12), viral infections and sleep disturbance (13). Overuse of acute medications is commonly identified as a risk factor for TM; it is present in more than 80% of TM patients in subspecialty clinics (9, 14). In population studies, medication overuse occurs in about 30% of TM sufferers (5).
Although medication rebound has not been demonstrated in placebo-controlled trials, rebound headache has been shown in a controlled trial of caffeine withdrawal (15).
The importance of medication overuse as a risk factor is supported by several lines of evidence: Medication overuse can make headaches refractory to preventive medication (9, 14, 16–19); Discontinuation of these medications results in significant improvement in headache (20). Many primary TM patients withdrawn from medication overuse no longer have daily headache, although a significant subgroup still have episodic migraine (20).
At least in a vulnerable subgroup medication overuse seems to be associated with the development of CDH (21–23). Medication overuse has been conceptually defined as the perpetuation or maintenance of chronic head pain in chronic headache sufferers, caused by the frequent and excessive use of immediate relief medications (14).
The aims of this study are to evaluate the patterns of acute medication overuse in TM patients presenting to a tertiary care Headache Centre and to compare the outcomes, at one year, of a group of TM patients who discontinued medication overuse, with those who persisted in it, in groups of patients with similar age, sex and psychological profile.
Methods
Clinical records and the headache calendars of 703 patients seen between 1980 and 2001 at The New England Center for Headache (NECH) in Stamford, CT, USA, a tertiary referral centre, were systematically reviewed to identify 492 with TM and medication overuse. We excluded patients who had a previous history of overusing medications different than the current being overused (n = 36). A total of 456 subjects were eligible for the study. Eligible patients had to meet criteria for TM diagnosed at the initial visit (24), and criteria for acute medication overuse (see below). Subjects were required to be followed at the centre for at least one year and not suffer from other forms of primary CDH (chronic tension-type headache, new daily persistent headache, hemicrania continua) or secondary headache disorders.
Acute medication overuse was diagnosed either based on amount of medication taken or the temporal profile of the headache (25). Patients were said to have medication overuse if they took:
Simple analgesic use (>1000 mg ASA/acetaminophen) > 5 days/week;
Combination analgesic use (caffeine, butalbital containing medication) >3 tablets a day for > 3 days a week;
Opiate use: > 1 tablet a day for > 2 days a week;
Ergotamine tartrate use: 1 mg PO or 0.5 mg PR for > 2 days a week;
Triptans > 1 tablet per day for > 5 days per week.
We also included patients with clinical features of rebound headache (headaches on awakening must mornings, escalation of pain at the end of dosing intervals, presence of pain after missing a dose of the medication) independent of the dose they were using.
During the entire time period reviewed, the clinic had been utilizing uniform clinical intake forms and headache calendars. We systematically collected information on all current medications, including dose, schedule, duration of use, degree of relief and side-effects, as well as all previous headache medications, including preventive and acute care medications. Medical records were abstracted by a study physician (MEB) using a standardized form.
The treatment of acute medication overuse at the centre includes nonpharmacological measures, preventive treatment, in- or out-patient detoxification from offending agents and initiation of proper acute care medication regimens. The choice of preventive drug was based on physician judgement and patients’ comorbidity. Standard preventives were used (data not presented). Based on this approach, two groups were identified:
Group 1 – Successful detoxification: Patients who were able to undergo the detoxification process and remained without medication overuse for the following year;
Group 2 – Unsuccessful detoxification: Patients who were not successfully detoxified, or returned to a pattern of medication overuse within one year.
Patients in group 2 were treated with nonpharmacological and pharmacological measures, as well as the patients in group 1, but continued overusing acute care medication. The choices and doses of preventive drugs were similar in both groups. Both groups were compared regarding the following outcomes, based on their headache calendars:
– Days with headache per month;
– Intensity of headache (none, mild, moderate, severe);
– Duration of headache (hours);
– Headache score (frequency × intensity);
the data was measured 1 year after the detoxification had being proposed.
As a part of the evaluation at the centre, all patients have their personality and psychopathology assessed at the first visit by taking the MMPI-2. The MMPI-2 is a 567-item, true-false questionnaire that evaluates the personality of the subject on 3 validity and 10 clinical scales. For each scale, a T-score of 65 is considered to be the level of clinical significance in the 95th percentile. The psychopathology of both groups prior to the treatment was also compared.
The Kolmogorov-Smirnov test was applied to assess the normality of the studied continuous data. Wilcoxon matched pairs test, Mann–Whitney U-test and Ficher exact test, were carried out on matched nonparametric data, nonmatched nonparametric data and contingency tables, respectively. The occurrence of T-scores > 65 at the MMPI-2 were analysed by the two-sided Fischer's exact test, the odds ratio being calculated considering a 95% confidence interval using the approximation of Woolf. Considering that scale 5 (masculinity-femininity) does not, by itself, allow a diagnosis, requiring further psychological evaluation, we did not consider the T-scores in such a scale.
Results
Our sample consisted of 456 (74.3%) subjects with TM, overusing acute care medication without a previous history of overusing a different medication. From the 456 subjects included in this study, 347 (76%) were females; mean age 42.8 years (range 11–74 years); mean follow-up period 6.3 years (range 1–15 years). Only 31 (0.7%) subjects were included on clinician diagnosis of medication overuse. All other patients met the defined criteria for medication overuse.
All patients had undergone previous medical consultation for headache, but only 171 (37.5%) had received any preventive treatment prior to their admission at the centre.
The vast majority of the subjects (76.7%) had daily headaches (≥28 days per month). Overall, 12.9% had 15–21 days of headaches per month.
Medication intake is displayed in Fig. 1. It ranged from 3 tablets per week to 30 per day (mean = 5.2 per day). More than 10 pills per day were taken by 48 (10.5%) subjects and more than 15 pills per day, by 20 (4.4%) subjects.

Medication intake: mean number of pills taken daily in subjects with transformed migraine presenting at a tertiary centre.
Figure 2 displays the number of different acute treatments that were currently overused, other than caffeine. The majority of patients were overusing 1(35.1%) or 2(36.8%) substances, but 31.6% were overusing 3 or more. Table 1 contrasts the medications involved in overuse, comparing patients whose first visit was more than 5 years ago with those whose first visit was in the last 5 years. The drugs more frequently associated with acute care medication overuse in the Center, butalbital, acetaminophen and opioids, are the same comparing both periods of time. There were statistically significant differences regarding NSAIDs (25.1%vs 10.1%, P < 0.0001), ASA (17.9%vs 31.7%, P= 0.0008), ergot compounds (19.5%vs 10.5%, P= 0.01) and sumatriptan (3.0%vs 10.5%, P= 0.001). The drugs associated with medication overuse did not significantly differ when comparing group 1 and group 2.

Number of different substances in overuse in subjects with chronic migraine presenting to a tertiary centre.
Drugs associated with medication overuse. Comparison between subjects whose first visit happened more than five years ago with those whose first visit happened in the last five years

P < 0.05.
Of 456 patients, 318 (69.7%) were successfully detoxified (Group 1), and 138 (30.3%) were not (Group 2). Of those unsuccessful, 67 (14.7%) were primary failures while 71 (15.6%) developed recurrent overuse (relapsed). All patients from both groups were receiving preventive medication after one year. Table 2 displays baseline characteristic of TM patients who successfully did (Group 1) and did not (Group 2) undergo detoxification. Group 1 consisted of 235 (73.8%) females; mean age = 41.7 years (range 11–74) and the mean number of days with headache per month at baseline was 25.5. Group 2 (overusing medication after one year) consisted of 138 (31.3%) patients, 71% females, mean age = 42.2 (range 19–72) and baseline mean number of days with headache per month of 24.9. No statistically significant differences were observed comparing these variables. We did not find positive correlation between the number of substances overused and the risk of unsuccessful detoxification.
Baseline characteristics of transformed migraine patients who successfully do and do not undergo detoxification

We did not find significant difference in the psychological profile of the patients of groups 1 and 2, prior to treatment (data not shown). No statistically significant differences were observed regarding the 9 considered scales of the MMPI-2.
Table 3 compares the number of days with headache, intensity and duration of pain at the baseline and after one-year of follow-up in groups 1 and 2. The number of days with headache and duration of pain were statistically reduced in both groups after one year of follow-up, compared to the baseline period. Number of days with headache decreased 73.7% in Group 1 and just 17.2% in Group 2 (P < 0.0001). Similarly, the duration of pain was reduced by 61.2% in Group 1 and 14.8% in Group 2 (P < 0.0001). We did not find statistically significant differences regarding the intensity of pain neither in group 1 nor in group 2, comparing the baseline and the follow-up periods.
Number of headaches per month, intensity and duration of the headache: comparison between Group 1 and Group 2

P < 0.001 when compared to the baseline period;
P < 0.001 when compared to Group 2;
P < 0.05 when compared to the baseline of group 1.
The evolution of the mean of the headache score comparing patients from both groups is displayed in Fig. 3. No statistically significant difference was observed in the baseline period between Group 1 and Group 2. The mean headache score is significantly lower in patients that stopped overuse compared both with the initial scores of this group (P < 0.001) and with the final scores (P < 0.001) observed in patients that did not stop overusing analgesic medication. A total of 225 (70.7%) subjects in group 1 returned to an episodic pattern of migraine, compared to 21 (15.3%) in group 2 (P < 0.001).
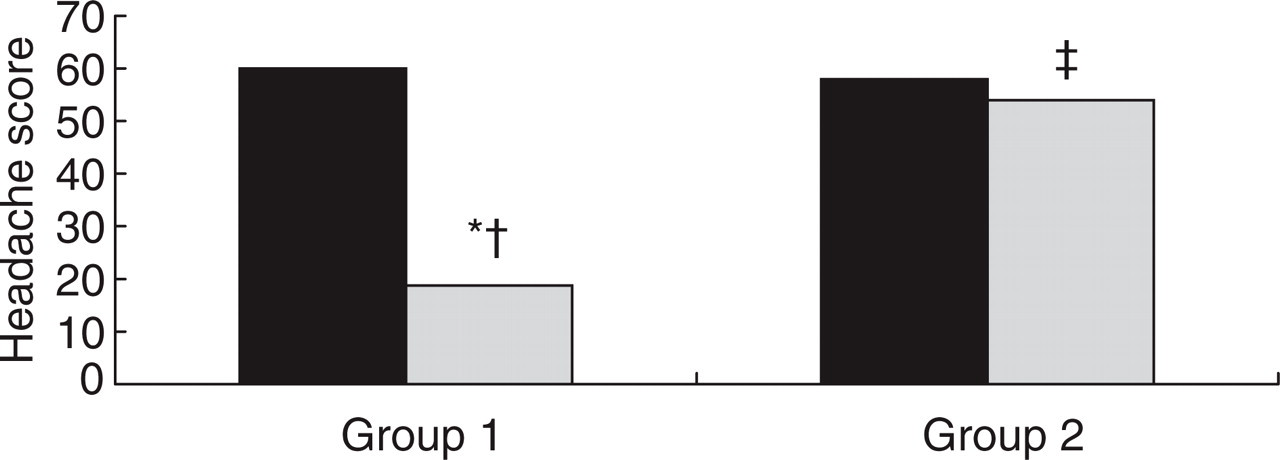
Evolution of headache score. Comparison between group 1 (persisted without medication overuse) and group 2 (continued or restarted medicaiton overuse). ∗P < 0.0001 compared to the baseline period; †P < 0.0001 compared to the follow-up period of group 2; ‡P < 0.05 compared to the baseline period.
Discussion
Acute medication overuse headache has been referred to, in the literature, as analgesic rebound headache, drug induced headache, medication withdrawn headache and several other names (2, 3, 17–20). These terms characterize the tendency for any type of acute antimigraine medication to perpetuate headache if used excessively. There is debate over the term rebound which sometimes refers to the fluctuating headache during the period of overuse of medication and at other times refers to the worsening of headache when the medications are abruptly stopped (D Dodick, personal communication). It may be better to call this syndrome acute medication overuse syndrome and the headache, acute medication overuse headache.
TM with medication overuse is one of the most common headache disorders seen by neurologists in practice or in clinics staffed by headache specialists (2–4). Among the several unanswered questions regarding TM, the role of the medication overuse in the chronification process deserves to be highlighted. Medication overuse is thought to be a cause of chronification of headache (9, 26, 27), although some authors argue that this association may be causal and that medication overuse is a response of chronic pain (28). Pini et al. (29) in a recent paper, showed that chronic analgesic use in CDH patients may be associated with a better quality of life than those with CDH not associated with medication overuse.
In this study we aimed to evaluate the patterns of medication overuse in a large sample of patients consulting in a tertiary care headache centre and to describe the outcomes after the withdrawal of the medication. Our data can be summarized as follow:
Only a 37% of patients presenting to a Headache Center with TM with medication overuse had used preventive migraine medication prior to their initial consultation;
The drugs more frequently associated with TM and medication overuse in new patients attending a tertiary centre have not significantly changed over the last several years. Butalbital-containing medications continue to be most frequent. However, ergot overuse has declined and triptan overuse has become more frequent;
TM sufferers frequently have headache every day, and nearly 70% use more than one pill per day and use more than one substance;
Both patients who were successfully detoxified and those who were not have statistically significant reduction in the frequency and duration of pain, and in the headache score, comparing the one-year follow up with the baseline evaluation;
No changes in the intensity of pain were observed in either groups.
Medication withdrawal is associated with a significant reduction in the number of days with headache, in the duration of pain, and in the headache score, after taken age, sex, and psychological profile into account.
Almost 50% of our patients were overusing butalbital and/or acetaminophen compounds followed by opioids and NSAIDs/ASA, and this pattern has not changed over the years. Data from a physician survey conducted 7 years ago (2) found similar results: nearly three quarters of respondents indicated that at least 50% of their patients with TM and medication overuse took over-the-counter analgesics (acetaminophen and NSAIDs/ASA); over half indicated that at least 50% were taking prescription analgesics. Medications that respondents reported were routinely overused by their patients with chronic headache were acetaminophen (27%), butalbital + ASA + caffeine (24%), aspirin (91%), other butalbital combinations (19%), ibuprofen (18%), codeine combinations (15%) and other opioids (13%). Kudrow, in 1982, (30) found a very similar pattern. These results are very similar to what we found and are indicative of a clear trend: butalbital, OTC analgesics and opioids are consistently associated with TM with medication overuse in the U.S. A reevaluation of the regulations governing the continued approval and dissemination of such medications seems to be of paramount and immediate importance (31).
The second part of our study regarded the comparison of outcomes after treatment in subjects that were and were not detoxified. Two strengths of the present study were firstly, the availability of the MMPI profile of subjects in both groups. Because psychological profiles were similar at baseline, psychological disturbances (depression, anxiety) that could lead to poor treatment response are unlikely to account for differences. Secondly, the availability of structured clinical records, questionnaires and patients calendars, used at the centre over the last 2 decades, allowed us to capture information in a uniform fashion.
Our results showed that, although the group that did not withdraw from overused medication improved with time, the group the successfully completed withdrawal showed far greater improvement in frequency, duration and headache score. The lack of improvement in pain intensity is consistent with the fact that episodic migraine is usually associated with higher intensity of pain than TM (24).
The benefits of discontinuing potentially overused medications in TM is supported by prior literature. Mathew et al. (16) showed that the results of combining discontinuation of the overused analgesics with the initiation of preventive medication resulted in headache improvement in about 80% of patients at two-month follow-up. In a recent prospective study of 95 patients, the duration and severity of withdrawal headache was investigated after complete withdrawal from overused symptomatic medications (32). At the end of the 2-month observation period, 85% of patients were pain-free. The authors’ assertion based on these findings was that discontinuation of the overused analgesic medication is the treatment of choice for medication-overuse headache. Young and Silbertein (33) recently stated that the standard of care for patients with TM and analgesic overuse remains detoxification from the overused medication followed by an intensive, long-term treatment plan which usually includes preventive medication.
While it is clear that detoxication and headache improvement are associated in these studies, the temporal sequence is not clear. Our clinical experience suggests that detoxication leads to clinical improvement but it is possible that instead, at least in some patients, clinical improvement may lead to detoxification. Because of the observational nature of the study and the simultaneous introduction of multiple interventions, causal sequence can’t be confidently specified. Other cautions are needed when interpreting our results:
This is a retrospective study with the weaknesses inherent in such research. Our results must be confirmed by prospective studies;
This study was conducted in a tertiary care headache centre and, despite the fact that the results agree with those of other physicians surveyed (2), selection bias may influence our results. For example, the pattern of medication overuse in this centre may not reflect medication use in the population;
We could not evaluate the critical dose of any medication in inducing medication overuse headache. Additionally, the criteria we used required the use of a triptan for at least 5 days per week. Recent studies show that triptan can induce medication overuse with lower doses (32);
Since all patients received preventive medication, the benefits of the drug withdrawal and of the preventive drug may have overlapped. It is clear, however, that those who stopped overuse reached much better outcomes after one year;
We did not collect data regarding disability and health-related quality of life. Pini et al. (29) showed that, patients who continued to overuse medication had a better quality of life than patients that did not, results criticized by Young and Silberstein (33). Though it seems unlikely that subjects that have lower frequency, duration and headache score would have reduced health-related quality of life, this information was not captured in our study.
Our results are restricted to patients with TM. These patients had episodic migraine in the past (24). Recent data (21) support the hypothesis that analgesic overuse can predispose the development of TM in those with migraine, but not in subjects without primary headache (21). Since all our patients had episodic migraine, we can’t, and do not intend to, propose any new conclusion about the causative effect of analgesic overuse in normal subjects.
Finally, although detoxification was tried in all patients overusing acute medication, data are presented overall because we did not contrast the outcomes of particular groups.
On conclusion, the careful analysis of our data strongly support the concept that successful detoxification is necessary to ensure improvement in the headache status when treating patients with this chronic and severe condition.
Footnotes
Acknowledgements
The authors thank AstraZeneca for funding this research.