
Abstract
Background
Knowledge about long-term outcomes after medication withdrawal therapy for chronic headache, including tension type and migraine headache is lacking.
Methods
We re-examined 56 patients an average of nine years after they participated in a medication withdrawal study with a one-year follow-up. We collected and compared data on headache, use of medication, quality of life, quality of sleep, anxiety, depression, and labor participation one and nine years after the start of withdrawal therapy.
Results
Headache days per month decreased from 16.7 (14.0–19.3) at one year to 13.3 (10.6–15.9) at nine years (P = 0.007). The proportion of patients meeting the criteria for chronic headache decreased from 27/56 (48%) at one year to 18/56 (32%) at nine years (P = 0.004). Medication overuse was reported in seven (13%) patients at one year and 18 (32%) at nine years (P = 0.013). The majority of patients overusing medication at nine years (10/18) belonged to a group of 14 patients who had a poor early response to withdrawal therapy and had sustained chronic headache after nine years. After excluding patients receiving retirement pensions, the proportion who received disability benefits increased from 21/55 (38%) at one year to 30/49 (61%) at nine years (P = 0.003).
Conclusion
Improvements after withdrawal therapy for chronic headache last at least nine years, with a parallel increase in the use of disability benefits. However, a high proportion of patients with a poor initial response to withdrawal therapy and sustained chronic headache overuse medication.
Background
Chronic headache, defined as the occurrence of headache 15 days or more per month over at least three months (1), has a prevalence of 2–3% (2). In the Head-Hunt study in Norway in 2000, chronic headache was defined as occurring >14 days/month and had a prevalence of 2% (3). The same group published a new study in Norway in 2011 and reported a prevalence of 2.5% for chronic headache and 1% for medication overuse headache (4). In a recent study from Denmark, the prevalence of chronic headache with medication overuse was 1.8% (5).
Modifiable risk factors for developing chronic headache include obesity, stressful life events, anxiety/depression, and medication overuse (6). Medication withdrawal therapy is a well-established treatment that leads to significant early improvement in approximately 28% of cases (7). According to follow-up studies, the effect seems to last for at least five years (8, 9). However, the long-term prognosis beyond five years has not yet been described.
From 2003 to 2007, we treated 80 patients with chronic headache (migraine and tension-type headache) and medication overuse with medication withdrawal and followed them for one year (10–12). In the present study, we re-examined 56 of these patients an average of eight years after the last follow-up, nine years after the start of withdrawal therapy. We collected data on headache, medication use, quality of life, sleep quality, anxiety, depression, and working ability. We also tried to identify the characteristics of patients with a persistent poor response to withdrawal therapy.
The study was approved by the ethical committee of Southern Norway and the research unit at Sørlandet hospital. The study was funded by the research unit at Sørlandet hospital.
Methods
Patients and outcome measures
This study recruited patients from the Agder counties in southern Norway. Inclusion criteria in the previous withdrawal study (10–12) were chronic headache (defined as headache occurring 15 days or more per month over at least three months, and classified as migraine or tension type headache) and medication overuse. The patients stayed in hospital for the first three days of the withdrawal period and were followed for one year at the out-patient clinic and/or by their general practitioner. At one year, 36% were responders, defined as ≥ 50% reduction in headache, and 23% relapsed regarding medication overuse.
Nine years after the start of withdrawal therapy, in 2013 we contacted all 80 patients from the previous study and asked them to participate in the present study. The patients who were willing to participate were informed in advance to use a headache diary for at least two months prior to the visit with the same doctor as in the previous study. During the visit, the headache diary was discussed and relevant headache data recorded. The primary headache type was classified according to ICHD III-beta criteria (1). We also collected data on medication use, labor participation, self-reported sleep quality, life quality assessed by SF-36 (13), and anxiety-depression using HADS (14) as described in detail in our previous papers (10–12). When evaluating labor participation, we recorded paid labor as a percentage of labor participation to 100%. Full labor participation of 100% is to be expected among healthy individuals.
Statistical analysis
We used student’s t-test to compare continuous variables in different groups, and the paired sample t-test to compare continuous variables at one and nine years within the same group. We used chi-square or the Fischer exact test (when there were fewer than five in a group) to compare categorical variables in different groups, and the McNemar test to compare categorical variables at one and nine years within the same group. We performed a multivariable regression analysis using days with headache in 2013 as the dependent variable (regarded as a continuous variable). The following independent variables were chosen due to their clinical relevance: having chronic headache at one year-follow-up, age, sex, present medication overuse, use of prophylactic drugs and the receipt of disability benefits. We adjusted for multiple comparisons by considering p < 0.01 as significant instead of 0.05. A significance level of 0.01 is frequently used in statistical literature as a somewhat stricter level. All statistical analyses were performed using IBM SPSS Statistics version 21 for Windows.
Results
Fifty-six of the 80 patients (70%) were examined an average of 9.2 (9.0–9.4, SD 0.68) years after they started withdrawal therapy. Twenty-four patients (30%) from the previous study were not included because two were dead (unknown causes, but to our knowledge not related to a neurological disease) and 22 did not respond to the invitation or did not want to participate. The non-participants did not differ significantly from the patients who agreed to participate regarding improvement to an episodic headache pattern after one year (11/24 vs. 29/56, P = 0.63), age, HADS, or number of days with headache before withdrawal therapy.
Patient and headache characteristics at one-year follow up and at nine-year follow up.


Patient flow chart showing how chronic headache status changed over time. Chronic headache = headache <15 days/month.
Use of medications at one-year follow up and at nine-year follow up.

McNemar test.
Sleep quality, anxiety, and depression at one-year follow up and at nine-year follow up.
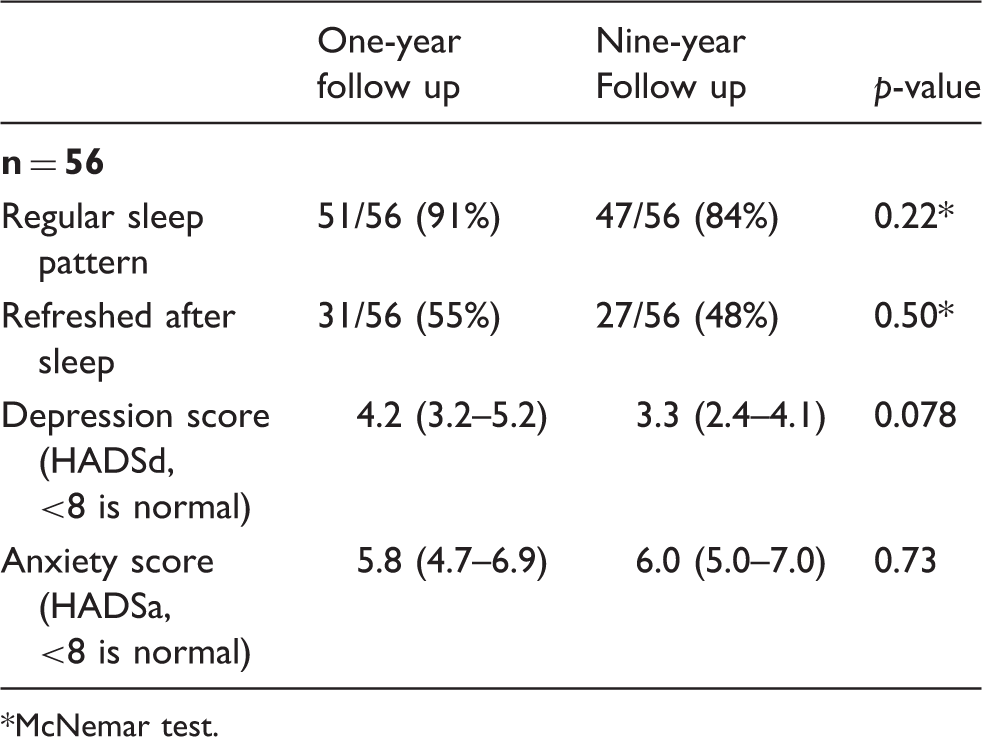
McNemar test.
Health related quality of life scores measured by SF-36 at one-year follow up and at nine-year follow up.
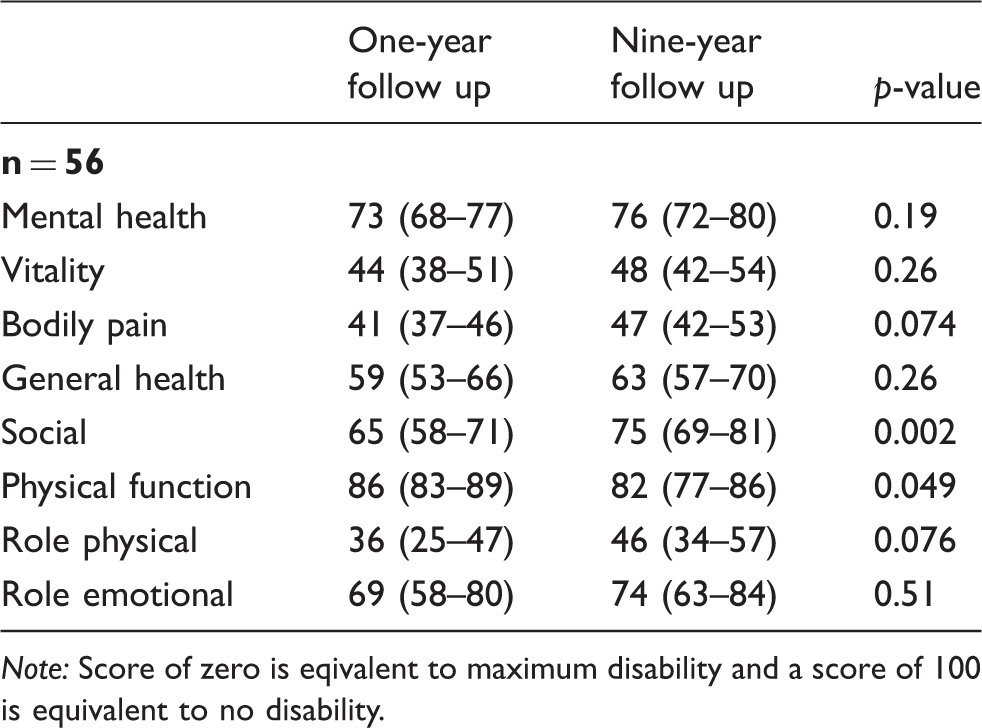
Note: Score of zero is eqivalent to maximum disability and a score of 100 is equivalent to no disability.
Labor participation was, on average, 47% (36–57%) at one year and 36% (25–46%) after nine years (p = 0.070). After excluding one patient receiving a retirement pension at one year and seven receiving retirement pensions at nine years, 21/55 (38%) patients received disability benefits at one year (from 25% to 100%) compared to 30/49 (61%) at nine years (p = 0.003).
Subgroup analyses showed that women (n = 39) under the age of 52 years (n = 19) had more headache days per month than women ≥ 52 years of age (n = 20) (16, range 12–21, SD 10.1 days vs. 10, range 6–14, SD 8.2 days; p = 0.027), but the difference was not significant. The mean age for menopause in Norway is 51.1 years (15). We set the limit at 52, because many women may have a more disturbing headache in the perimenopausal period (16). Men under and over the age of 52 (n = 10 and 7, respectively) had similar headache days per month (17, range 10–24, SD 9.7 vs. 9, range 0–19, SD 10.1; p = 0.119).
We performed a regression analysis using the following factors as possible predictors of headache-free days at nine years: having chronic headache at one year, age, sex, present medication overuse, use of prophylactic drugs, and receiving disability benefits at the end of the last study. The analysis showed that overusing medication at nine years contributed significantly to the number of headache days (B 12.352, SE 2.405, beta 0.596, p < 0.0001). The other variables had no significant impact on the number of headache days.
Patients with a sustained chronic headache pattern at nine years
Fourteen of the 56 patients (25%) had a poor initial response to withdrawal therapy and had a sustained chronic headache pattern (SCH) at nine years. Twelve had a chronic migraine (86%) and two had a chronic tension type headache (14%). They had 27.9 (25.9–29.9) headache days per month at one year and 25.2 (21.6–28.8) headache days per month at nine years (p = 0.036). SCH patients had lower SF-36 vitality scores (33, range 20–47 vs. 53, range 47–59; p = 0.003) and more common medication overuse than the other patients [10/14 (71%) vs. 8/42 (19%), p = 0.0001]. Not feeling refreshed after sleep was more common among SCH patients, but the difference from other patients was not significant [11/14 (79%) vs. 18/42 (43%), p = 0.030]. SCH patients did not differ from the rest of the patients regarding anxiety, depression, and labor participation. Four of the 14 SCH patients (29%) used preventive drugs compared to 19/42 (45%) of the other patients (p = 0.36). In addition, 6/13 (46%) patients that reverted from a chronic headache pattern at one year to an episodic pattern used preventive drugs (p = 0.44 compared to SCH patients).
Patients who changed from chronic headache to episodic headache at nine years
Thirteen patients had chronic headache after one year, but had changed to an episodic pattern by nine years (Figure 1). A subanalysis of these 13 patients compared to the 14 SCH patients at nine years did not reveal any significant differences regarding the use of prophylactic drugs or acute headache medication. We found a non-significant difference in the use of codeine medications, as those with SCH were more prone to use it (p = 0.077). No significant difference was found regarding age, labor participation, the receipt of disability benefits, self-reported sleep quality, or anxiety or depression measured by HAD. The vitality scores on SF-36 were not significantly different (p = 0.029). However, we did find a significant difference regarding headache days among those that converted to an episodic pattern at nine years compared to SCH patients (8.9, range 5.6–12.3 headache days/30 days vs. 25.2, range 21.6–28.8 headache days/30 days; p = 0.0001).
Discussion
Approximately 30% of patients with medication-overuse headache respond to withdrawal therapy (7), and follow-up studies have shown a lasting effect for up to five years (8,9). In the present study, we followed a cohort of patients for nine years after withdrawal therapy. Unlike previous studies, we paid special attention to the subgroup with an initially poor response and sustained chronic headache.
Our study shows that the beneficial effect of withdrawal therapy on chronic headache persists over nine years. The majority (86%) of patients with an early response to withdrawal therapy (defined here as not having chronic headache one year after withdrawal) were still free of chronic headache at nine years. We also observed an improvement over time, as the number of headache days per month for the whole cohort decreased significantly from 16.7 to 13.3 days per month. Although this is a significant improvement, the group still have very frequent headaches.
A considerable proportion (23%) of patients who had chronic headache at one year had returned to an episodic headache pattern at nine years. The proportion of patients who overused medication was higher at nine years (32%) than at one year (13%), but the difference was not significant. The social functioning domain of quality of life measured on the SF-36 also improved significantly from one to nine years. These encouraging results are in line with previous follow-up studies beyond one year after withdrawal. An Italian five-year follow-up study of headache in 58 chronic migraine patients reported 10.5 headache days per month one year after withdrawal and 11.3 headache days per month five years after withdrawal (9). A German telephone interview study of 75 patients subjected to withdrawal therapy found that, after four years, 45% of the patients had relapsed into medication-overuse headache (17).
Whether the improvement in headache and quality of life from one to nine years is caused by the withdrawal therapy or other factors is not known. We could not find any differences between SCH patients and those that converted to an episodic pattern. This could be due to the inclusion of very few patients or not asking the right questions. At nine years, many patients reported that they were better able to cope and live with the headache than before. Some expressed relief that their children were older and needed less support. Women ≥52 years of age had a non-significant tendency towards fewer headaches then the younger women. This is in line with previous studies that showed improvement in migraine after menopause (18). Several patients said that the most important improvement occurred when they reduced or stopped working and received disability benefits or pension. In the HUNT study from Norway, the prevalence of >8 weeks’ sick leave during the past year was more than three times higher among individuals with headache than those without headache, and those with chronic headache had the highest rate of sick leave (19).
Our study confirms a high rate of disability benefits in Norwegian headache patients. Overall, labor participation decreased from 47% to 36% and the number receiving disability benefits increased from 38% to 61%. We could not find any significant difference in labor participation and the number receiving disability benefits between SCH patients and those with an episodic pattern and a much lower headache burden. We do not have any explanation for why this difference exists; we thought that those with a higher burden would have lower labor participation, but that was not our finding. Maybe a difference would be evident if the study had included more participants. Nevertheless, we still speculate whether lower labor participation has a positive impact on headache. A permanent solution regarding labor ability and stable income may lead to a more predictable future and remove uncertainty that could otherwise act as a trigger for headache.
Patients with sustained chronic headache
Twenty-five percent of the cohort had SCH one and nine years after withdrawal therapy and had, on average, 25 headache days per month at nine years with a significantly lower vitality score than the rest of the cohort. These patients had fewer headache days after nine years and the difference was near significant (p = 0.036), but they still had a very high number of headache days per month.
Regression analysis revealed a significant association between headache days and medication overuse at nine years for the whole cohort. The majority of SCH patients (71%) overused medication. Why so many reverted to medication overuse, or whether some of them could have improved over time if they reduced their use of medication, is not clear. The use of preventive drugs was low in this group, and higher use could possibly have improved the situation.
Our experience is that it is difficult to convince a patient to attempt medication withdrawal again if they did not succeed with a previous withdrawal attempt, or experienced very little change in their headache pattern. We think that factors other than medication overuse may also contribute to headaches in this group, and that we should make a greater effort to identify them rather than insist on repeated medication withdrawal attempts. The patients with SCH used significantly more medications than the other patients, and there was a non-significant tendency towards greater use of codeine drugs. There was also a non-significant tendency towards reduced sleep quality. The SCH patients did not have more depression and anxiety than the others, but this does not rule out other contributing psychological factors. A study from Norway showed that behavioral problems, anxiety, and depression in adolescence are associated with recurrent headache (20). Other studies have shown that individuals who have experienced traumatic events in childhood are more prone to suffer from pain and headaches than those who did not (21–23).
Strengths and weaknesses
The strength of this study is that all patients had a long record with detailed information about their headache and symptoms. The same consultant met the patients at both follow-ups and the patients filled in their headache data carefully. We counted days with headache in our data, which is a precise way of evaluating headaches because it is easy to understand and record in the diary and less prone to subjective interpretation than other methods.
The weaknesses of the study are the small number of patients and not including all patients from the original study. We cannot exclude bias due to the selection of patients with a favorable outcome. Furthermore, we could have examined muscle tension and previous traumatic events more specifically to further characterize the patients with sustained chronic headache.
Footnotes
Clinical implications
Medication-overuse headache patients with a good early outcome after withdrawal therapy have a good long-term prognosis, and patients with a poor early outcome after withdrawal may improve with time.
The number of patients receiving disability benefits increases with time after withdrawal therapy.
Subgroups of medication-overuse headache patients have a poor early response to withdrawal therapy and a poor long-term prognosis. The patients often revert to medication overuse.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sørlandet hospital.
Acknowledgements
We thank the research unit at Sørlandet hospital for funding and support.