
Abstract
Introduction
A relationship between headache and excessive daytime sleepiness (EDS) has been suggested. This study investigated this association in relation to people with chronic migraine or chronic tension-type headaches.
Methods
A total of 30,000 persons aged 30–44 from the general population were screened for chronic headache. Those eligible were interviewed by a headache specialist. EDS was defined as Epworth sleepiness scale score >10. Logistic regression models were used.
Results
Among the 323 eligible participants, 21.1% had EDS. In multivariable logistic regression analysis, the odds ratios (OR) of EDS were not significantly different in people with CM and CTTH. However, high headache frequency was associated with EDS (OR 2.03 (95% CI 1.11–3.73, p = 0.022)) for those with ≥ 80 compared to < 80 headache days/3 months, after adjustment for type of headache, age, and gender.
Conclusions
Increased EDS was associated with higher headache frequency, but not with specific headache diagnoses.
Introduction
Excessive daytime sleepiness (EDS) is associated with pain, but only a few studies have investigated EDS in migraine and headache. The results are not uniform, possibly due to different methods and patient populations (1–6).
The aim of this study was to investigate the prevalence of and factors associated with EDS in participants from the general population with chronic migraine (CM) or chronic tension-type headache CTTH), since this has not previously been done.
Methods
Study design, population and variables
In a cross-sectional survey of 30,000 people aged 30–44 drawn from the general population of eastern Akershus County, Norway, we used a postal questionnaire to screen for possible chronic headache (≥15days/last month and/or ≥180 days/last year). Screening-positive people were invited to a clinical interview at Akershus University Hospital.
Of the eligible participants, 71% (20,598/28,871) responded to the questionnaire. Of the 935 people with self-reported chronic headache, 633 were interviewed by two physicians experienced in headache diagnostics (490 face to face, 143 by telephone). After the interview, the participants filled in a self-administered questionnaire including the Epworth Sleepiness Scale (ESS). A more detailed description can be found elsewhere (7).
The participants also provided information on socio-demographics, height, weight, smoking status, medication overuse, headache frequency and headache disability via the Migraine Disability Assessment (MIDAS), and emotional distress via the Hopkins Symptom Checklist-25 (HSCL-25).
Headache classification
ICHD-II was applied in the interview. The diagnoses were reclassified according to ICHD-3 beta (8). We included people with CM or CTTH in the analyses, and excluded five people with other primary headaches, due to the low number of such diagnoses.
Excessive daytime sleepiness
The ESS questionnaire describes eight daily situations in which the respondents estimate their likelihood of dozing off on a 0–3 scale, i.e. 0 = no chance, 1 = slight chance, 2 = moderate chance, 3 = high chance (9). The ESS total scores (0–24) were dichotomized into scores ≤ 10 and > 10; the latter is considered as clinically significant EDS.
Statistical analysis
For descriptive data, proportions, means and SDs or 95% confidence intervals (CI) are given. Groups were compared using the t-test (continuous data) or the χ2 test (categorical data).
Logistic regression models were used to evaluate EDS (yes or no, as the dependent variable) in persons with CM or CTTH, using multivariable models. We estimated base models with (a) CM or CTTH, age, gender, and medication overuse as independent variables, and (b) extended models with the addition of headache frequency above the 75th percentile (≥80 days /3 months), emotional distress by HSCL-25 score (≥1.67 for men and ≥1.75 for women) vs. no distress (<1.67 for men and <1.75 for women), and severe headache disability by MIDAS score > 20 vs. no to moderate disability ≤20 as independent variables. In the base models, we assessed multiplicative interactions between headache diagnosis or medication overuse with age and gender. Finally, the impact of co-occurring migraine (yes or no) in those with CTTH was estimated using the same model specifications. The results are presented as odds ratios (ORs) with 95% CIs.
Significance levels were set at p < 0.05, using a two-sided test. We used Stata version 14.2 (StataCorp, College Station, TX) for all statistical analyses.
Ethical issues
The Regional Committee for Medical Research Ethics and the Norwegian Social Science Data Services approved the study. All participants gave informed consent.
Results
Descriptive statistics for respondents with classified chronic headaches. Number (%) unless stated otherwise.

1n = 252, 2n = 30, 3n = 288
The overall prevalence of EDS was 21.1% (95% CI 17.0–25.8) among those with CM and CTTH; 20.6% (95% CI 16.1–26.1) among women and 22.5% (95% CI 14.4–33.5) among men. The prevalence of EDS in CM was 20.0% (95% CI 8.9–39.1) for women, 30.0% (95% CI 10.8–60.3) for men, and overall 22.9% (95% CI 12.1–39.0). Furthermore, the prevalence of EDS in CTTH was 20.7% (95% CI 15.9–26.4) for women, 21.3% (95% CI 12.9–33.1) for men, and overall 20.8% (95% CI 16.5–25.9). Headache diagnosis, age, gender or medication overuse was not associated with EDS (Figure 1). There was no multiplicative interaction between headache diagnosis and age or gender, or between medication overuse and age or gender in this model.
Odds ratios for having excessive daytime sleepiness (EDS) among people with chronic migraine (CM) or chronic tension-type headache (CTTH). Multivariable logistic regression analysis. Base model (n = 323).
MIDAS or HSCL-25 scores were not associated with EDS, while high headache frequency, dichotomized into ≥80 and <80 headache days/3 months was associated with EDS (OR 2.03, 95% CI 1.11–3.73, p = 0.022), after adjustment for headache diagnosis, age, and gender (Figure 2).
Co-occurrence of migraine in people with CTTH was not associated with EDS (OR 0.89, 95% CI 0.48–1.64, p = 0.70). The prevalence of EDS in CTTH without vs. with co-occurrence of migraine were 22.2% (95% CI 16.5–29.2) and 18.9% (95% CI 13.0–26.6, p = 0.50).
EDS was associated with high headache frequency, dichotomized into ≥ 80 and < 80 headache days/3 months (OR 2.02, 95% CI 1.07–3.82, p = 0.022).
Odds ratios for having excessive daytime sleepiness (EDS) among people with chronic migraine (CM) or chronic tension-type headache (CTTH). Multivariable logistic regression analysis. Base model + headache frequency, MIDAS and HSCL-25 scores (n = 288).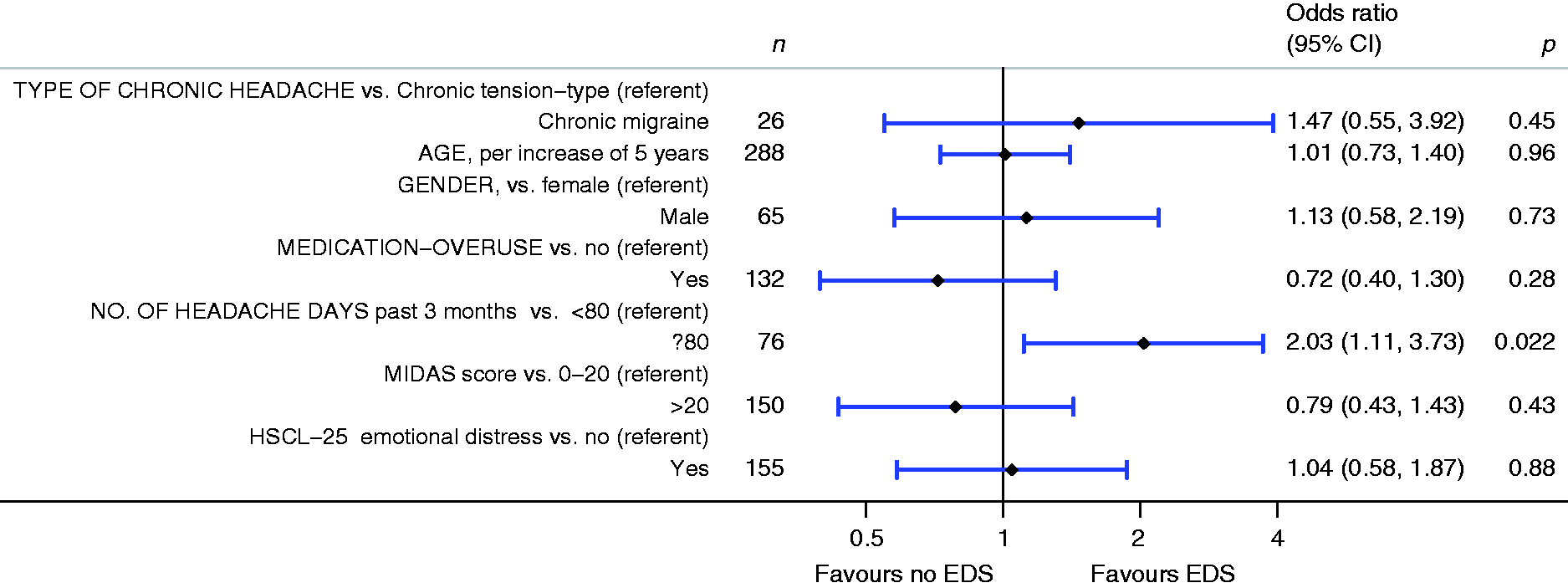
Discussion
The main findings were that EDS did not differ among those with CM or CTTH. However, EDS was associated with high headache frequency, i.e. headache frequency above vs. below the 75th percentile (≥80 days/3 month period). Furthermore, medication overuse, headache disability, and psychological distress were not associated with EDS in this population. Co-occurring migraine in people with CTTH was not associated with EDS.
The prevalence of EDS in men and women with CM or CTTH corresponds well with that of the Norwegian general population (16.1% women, and 20.1% men), as well as that of Korean and Norwegian migraineurs from the general population (20%) (4–6,10). Furthermore, the prevalence is comparable to that in an Italian tertiary care study of CM (20%) (2). In contrast, the prevalence of EDS was higher in Austrian (33% and 35% for episodic migraine) and American (32% for episodic migraine and 40% for CM) migraineurs based on selected populations (1,3).
The differences in the prevalence of headache diagnoses and EDS may partly be explained by the differences in study designs, different cut-offs for EDS (ESS ≥ 10), and/or use of different headache classifications (1–4). Furthermore, different cultural ways of defining sleepiness has been suggested as explaining the large variation of EDS reported across the world (10). Face-to-face interviews by headache experts, as in the present study, provide more valid headache diagnoses than questionnaire-based studies (11). Although physicians may differ in their diagnosing, there were no differences in the proportions of the diagnoses or medication use between the two physicians who conducted the headache interviews.
No previous study has compared EDS for CM and CTTH in the general population. Thus, the finding that EDS did not differ between these diagnoses is new and can only indirectly be compared with previous studies. A Norwegian study of the general population found that EDS was significantly increased among migraineurs, but not among those with tension-type headache after adjustment for age, gender and sleep medication (4).
The Italian tertiary care study found that EDS was more common in people with CM than in healthy controls (20% vs. 6%; OR 3.9, 95% CI 1.5–10.2), but the association disappeared after adjusting for poor sleep quality and use of anxiolytics and antidepressant drugs (2). Two recent population surveys found a significant, but weaker association between migraine and EDS, which disappeared after adjusting for the confounders anxiety, depression, sleep quality and sleep duration (5,6).
The finding that those with headache frequency/3 months above the 75th percentile (> 80 days/3 months) had more EDS than those below this percentile supports the previous finding in a Norwegian questionnaire-based study, where EDS increased with increasing headache frequency among both migraineurs and non-migraineurs, and that those with chronic headache had the highest prevalence of EDS (6).
An association between EDS and different chronic pain conditions has been reported. Our findings that increased frequency, but not type of headache, increased EDS may contribute to the hypothesis that it is the burden of complex pain rather than the specific condition that is associated with EDS.
The population-based sample in the present study was large, and the high response rate should ensure that the sample was representative of the general population. The ESS is a widely used validated questionnaire for evaluating subjective daytime sleepiness, and the score is associated with clinically-important outcomes (12).
The 30–44 years age range in our study was chosen in order to ascertain a general population sample without much co-morbidity of non-headache disorders. Because EDS varies with age, our findings may not be generalizable to younger or older populations. The study lacked data on sleep quality and sleep duration that may be associated with sleepiness in headache (2,3,5,6). The overall sample size limited the number of variables that could be analyzed as potential confounders, and this also lead us to dichotomize many variables for use in the analyses. Finally, the cross-sectional design in the present study does not permit any conclusions about causality in the relationship between CM/CTTH and EDS.
In conclusion, CM and CTTH with or without medication overuse were not associated with EDS, while a high frequency of headache was associated with higher odds of EDS in this general population sample.
Clinical implications
Excessive daytime sleepiness does not differ among subjects with chronic migraine and chronic tension-type headache. High frequency of headache is associated with increased risk of excessive daytime sleepiness. When treating people with primary chronic headache, physicians should examine sleep problems and treat them both accordingly.
Footnotes
Authors’ contributions
MBR had the original idea for the study and planned the overall design together with CL. All authors were involved in the planning and interpretation of the data analysis. ESK and KS conducted the data analysis. ESK prepared the initial draft. All authors have commented on, revised and approved the final manuscript.
Acknowledgments
Kjersti Aaseth and Ragnhild Berling Grande conducted the clinical interviews.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the South East Norway Regional Health Authority and Institute of Clinical Medicine, Campus Akershus University Hospital, University of Oslo.