
Abstract
It is indisputable that the global scientific advances in headache research, be it bench or bedside, have benefited enormously from the operational diagnostic criteria published in 1988. Today, this classification system is indispensable. The reason for this success is a low inter-rater variability. In general, orofacial pain conditions are less well characterised – with the noticeable exemption of temporomandibular disorder pain. Tremendous work has been put into changing this, and significant progress has been achieved – in particular, in terms of the clinical implications and overriding conceptual models for oro-facial pain. Scientific classifications have only one goal: To provide a scientific agreement about the main features of an object of research and a scientific consensus regarding the name. The main significance is not the fact that a good classification offers a detailed and accurate image of the reality. If we want to overcome the obstacles of different competing classification systems, we need to overcome specialisation borders. The key to success is to understand that such a definition does not mirror all possible clinical facets of a given pain condition but is simply a convention – that is, a consensus on a word used for a pain condition. Simply speaking, a classification creates a common language to be used by more than one profession. It will be crucial to define any given pain condition as precisely and rigid as possible, in order to ensure a homogenous population. Only this ensures a low inter-rater variability, which consequently allows combining and comparing research on a population across different professional settings. This is not easy for chronic facial pain without verifiable morphological cause or structural lesions, as these syndromes are often rather featureless. The new IASP classification of chronic pain is a big step forward to a better characterisation of such conditions, and will trigger future work on a new and operationalised classification of oro-facial pain.
It has been the general belief that facial pain and headache are first of all a symptom and not a disease in its own right. It was later realised that no morphological cause or structural abnormalities can be found in the majority of sufferers, and hence their pain condition has to be regarded as primary, that is, the pain syndrome in these patients is the disease itself, in contrast to secondary forms where the pain is a symptom of a disease such as a tumour or a trauma. Whereas in headache an unrivalled classification has been established (1), the classification of facial pain (2) has been less rigorous and not undisputed (3). A prominent exemption is the so-called Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) (4), now replaced by the Diagnostic Criteria for TMD (DC/TMD) (5). TMD was the former umbrella term used to describe a range of disorders in the jaw muscles, temporomandibular joint and associated tissues, with the cardinal signs and symptoms being pain, TMJ noises and perturbed jaw movements. However, until the milestone publication by Dworkin and LeResche in 1992 (4), there was no general agreement on criteria for the different sub-diagnosis. The RDC/TMD proposed and provided evidence in terms of reliability for operationalised TMD diagnosis. The newly updated DC/TMD, based on significant efforts, provides additional information about the validity of the TMD diagnosis. Therefore the DC/TMD is unique, and has set the standards for establishing diagnostic criteria for other types of oro-facial pain conditions than TMD. The difficulty in oro-facial pain classification may be that the majority of acute facial pain is related to oral/dental diseases, and is therefore a symptom rather than a syndrome. If pain persists and no dental cause can be established, differential diagnosis and treatment is challenging, and dentists should use multimodal and multidisciplinary approaches.
The last decade has seen tremendous efforts to better characterise and classify facial pain patients (4) with the goal of creating a modern and generally accepted classification integrating WHO, IHS and ICD-11 systematics.
Currently, the IASP Task Force is working on a simple and pragmatic classification model (7) for chronic pain with seven proposed main categories: 1. Primary pain, 2. Cancer pain, 3. Postsurgical and post-traumatic pain, 4. Neuropathic pain, 5. Headache and orofacial pain, 6. Visceral pain and 7. Musculoskeletal pain. The significance of this new pain classification is that, for example, TMD pain, as one of the most common types of orofacial pain, can be viewed as both a musculoskeletal pain condition and a primary pain condition because of the location, involved tissue and idiopathic background.
It should be noted that chronic pain in the new definition indicates a duration of more than three months replacing the former IASP definition of > 6 month duration. The subgroup of headaches and orofacial pain will be defined according to the ICHD-3 and the DC/TMD classifications, thereby placing more emphasis on the remaining types of chronic orofacial pain. A final note is that this new IASP classification system is a compromise between a mechanistic classification (e.g. neuropathic pain), a topographical classification (e.g. headache and orofacial pain) and tissue classification (e.g. viscera and musculoskeletal). Nevertheless, it is sufficiently pragmatic and clinically applicable and, importantly, will be adopted by the International Classification of Diseases. Given that this endeavour is inherently multidisciplinary, debates are welcome and compromises required (7). The question is, why do we need a more rigorous classification, have we not characterised facial pain sufficiently?
Scientific classifications have only one goal: To provide a scientific agreement on the main features of an object of research and a scientific consensus regarding the name. As long as the features of an object of research are not precisely defined and the name universally accepted, this object (i.e. disease) cannot be meaningfully examined and scientific progress is consequently frustrating. If a given facial pain syndrome is attributed with several names not used synonymously, the first and most obvious barrier is that medical doctors, dentists and scientists may investigate the same clinical problem without recognising this and consequently cannot share the data. Even worse is the case when such a syndrome is ill defined and, more to the point, superficially defined. This is best illustrated by an easy example (see Figure 1): Let us assume a scientist develops a substance that aborts migraine attacks in 100% of migraine patients. This substance is tested in 100 patients with half-sided headache, as there is no better definition for migraine in this example. Twenty of these patients actually suffer from migraine, the other patients suffer from other half-sided headaches such as cluster headache, SUNCT-syndrome, hemicrania continua, occipital neuralgia, tension-type headache and so forth. This study fails, as the scientist can only show a positive response in 20% of the patients. The reason is solely because the inclusion criteria, that is, the classification of the syndromes, were imprecise. If we replace the drug with the words neuroimaging, genetic study, epidemiology and so on, it becomes eminent that a good classification is the key to scientific success (8). A good classification does not necessarily provide the most detailed and accurate image of the reality, but provides a scientific agreement on the main and operationalised features of an object of research and a scientific consensus regarding the name (9).
Theoretical example of an idealised research question (assumed 100% accuracy of the used test in migraine) in a patient population which is poorly defined (left hand side) versus a population which is rigorously defined (right hand side).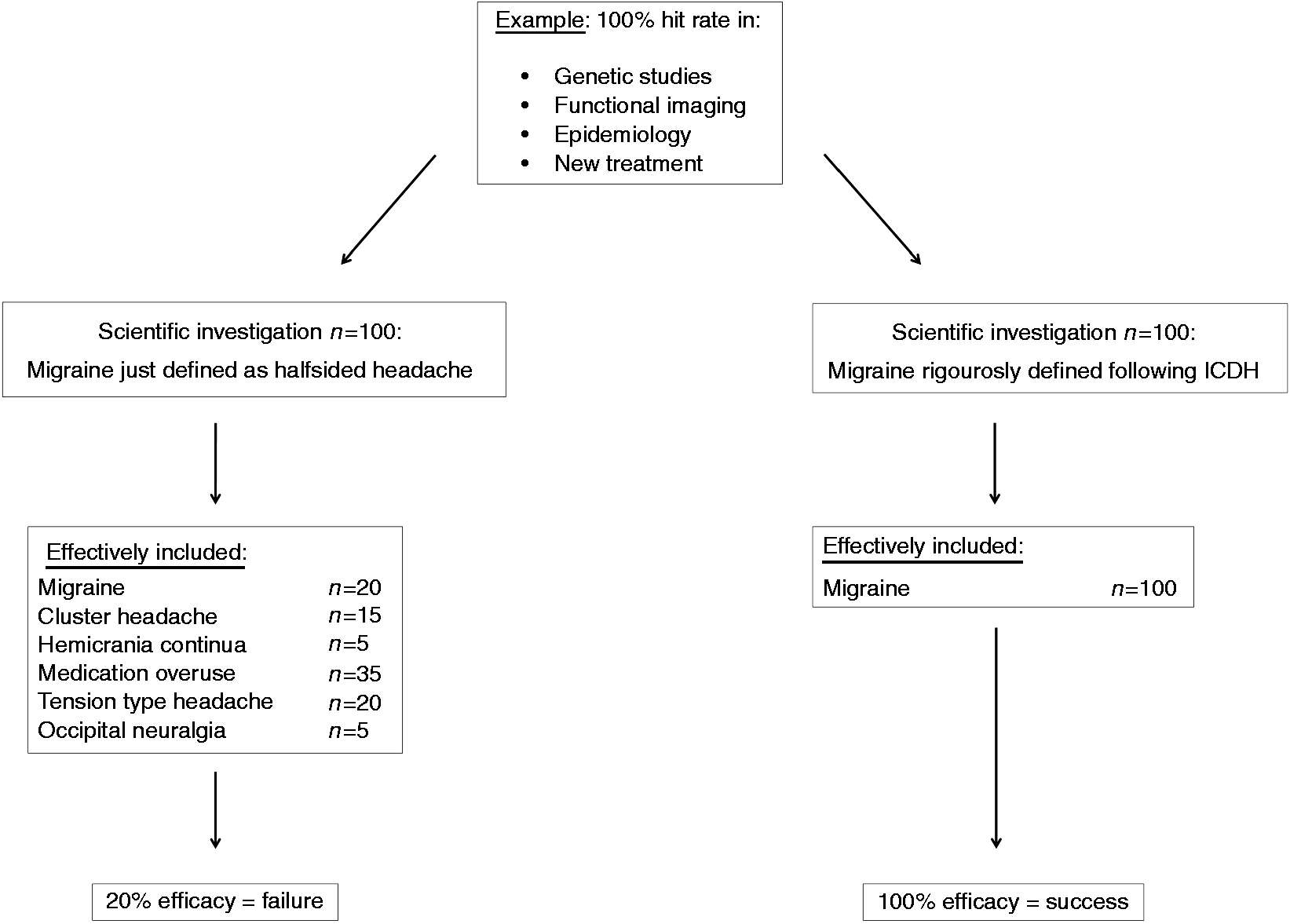
An example of an ill-defined headache syndrome is tension-type headache (1). Consequently, we know little about the pathogenesis and even less about how to treat this syndrome efficiently. The reason is, probably, that the term tension-type-headache combines a mixture of several not-yet better classified headache types and causes. There may also be a significant overlap with some of the painful TMDs (10). An example of a badly defined non-dental chronic facial condition is atypical facial pain, now called persistent idiopathic facial pain (PIFP). However, there may be a significant need to better define the intraoral version of PIFP, and attempts have been made to formulate criteria for a “persistent alveolar-dental pain” (PDAP) (10). Again, the most important criteria for success may not be the name in itself, but rather well-defined, operationalised and reproducible criteria.
If we want to overcome the obstacles of different classification systems, we also need to overcome specialisation borders. All faculties involved in facial pain diagnosis, treatment and scientific investigation need to find and agree on a general and universal definition of a given facial pain syndrome. The key to success is to understand that such a definition does not mirror all possible facets of a given syndrome, but simply depends on convention – that is, a consensus on a word to be used for a syndrome (11). Thus, it does not matter which combination of features we call PIFP or PDAP, as long as all of us agree on what combination of clinical symptoms is called PIFP and PDAP. In the definition of PIFP inherently lies the demarcation from all other facial pain syndromes – which is (next to standardised communication) the key element of scientific investigation of PIFP. The consensus on the basic features of PIFP is therefore achieved through simple definitions and not through systematic studies.
Clinicians might argue that a rigid classification system cannot accommodate all clinical pictures, and that not all patients may fit into the defined categories. It is extremely important to stress the fact that the headache classification in its current form was not written for clinicians but for scientists (see preface and introduction of the 1988 classification (12)). It is not the aim to categorise each single patient, but to define categories in which a patient either clearly fits or clearly does not fit. This is the key to ensuring that studies done on this specific category can be done anywhere in the world and results can be compared. The more rigid the classification becomes, the better is the comparability of the results. The same philosophy applied to the conception of the RDC/TMD. Of note, consensus on the key features of a disease or disorder is also helpful for the clinical community: It makes communication among health professionals easier, and it alerts us to suspecting other – possibly malignant – causes, in cases where the symptoms do not exactly match these diagnostic criteria. Clearly defined diagnostic criteria are thus of vast importance for diagnostic and eventually even therapeutic decisions (9).
Footnotes
Article highlights
It will be crucial to define any given pain condition as precisely and rigidly as possible, in order to ensure a very homogenous population. Only this ensures a low inter-rater variability, which consequently allows combining and comparing research about this population even in different professional settings. The main significance herein lies exactly not in the fact that a good classification offer a most detailed and accurate image of reality. If we want to overcome the obstacles of different classification systems, we need to overcome specialisation borders.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.