
Abstract
Background
Dopaminergic symptoms may be extremely pronounced in some migraine patients during the attack, representing a major source of disability.
Objectives
We aimed to carefully characterize the clinical picture of migraine patients with dopaminergic symptoms in a large patients’ population as a putative migraine endophenotype, allowing more precise disease management, treatment and outcome prediction.
Methods
We screened 1148 consecutive tertiary care episodic and chronic migraine patients with face-to-face interviews collecting thorough data on lifestyle, socio-demographic factors, and clinical migraine features.
Results
We identified 374 patients with migraine with dopaminergic symptoms (32.6%). The most frequent dopaminergic symptom was yawning followed by somnolence, nausea, vomiting, fatigue, mood changes and diuresis. Migraine patients with dopaminergic symptoms had longer attack duration (OR: 1.82; 95% CI: 1.41–2.36, p < 0.0001), more frequent osmophobia (OR: 2.01; 95% CI: 1.50–2.69, p < 0.0001), allodynia (OR: 1.43; 95% CI: 1.10–1.85, p = 0.0071) and unilateral cranial autonomic symptoms (OR: 1.31; 95% CI: 1.01–1.68, p = 0.045), but used less preventative treatments (OR: 0.74; 95% CI: 0.57–0.98, p = 0.033) than patients without dopaminergic symptoms.
Conclusions
Migraine patients with dopaminergic symptoms are characterized by a full-blown, more disabling migraine. Dopaminergic system modulation should be carefully considered in individuals with migraine with dopaminergic symptoms for both acute and preventative treatments in future ad hoc designed studies.
Introduction
Migraine is a sequential multiphasic process characterized by the appearance of dopaminergic symptoms (DAs) during the different attack stages (1). Yawning and somnolence, symptoms pertaining to dopamine pre-synaptic receptor activation, may occur during prodromes whereas nausea and vomiting, related to dopamine post-synaptic receptor stimulation, characterize the headache stage. Other dopamine-related symptoms, namely fatigue, diuresis and mood swings, may also appear during the different attack phases (2–5).
Dopamine is a well-recognized migraine player (6–8). Dopamine receptor hypersensitivity due to a chronic impairment of dopaminergic neurotransmission is indeed a migraine hallmark, as suggested by clinical, pharmacological, biochemical, genetic or neuroimaging studies (9–15).
In some migraine patients, dopaminergic symptoms accompanying the attack progression may be very pronounced and disabling, requiring specific adjunctive treatments. We postulate that these patients with migraine might represent a peculiar migraine endophenotype. To address this hypothesis, we assessed the frequency and characteristics of DAs in a large, well clinically characterized migraine outpatient population, detailing lifestyle, behavioral and socio-demographic factors and clinical phenotype.
Methods
Patients affected by episodic (with or without aura) or chronic migraine (with or without medication overuse) (16) were consecutively enrolled at the Headache and Pain Unit of the IRCCS San Raffaele Pisana Hospital in Rome from 1 December 2017 to 31 December 2018. After signing an informed consent, all patients underwent a careful physical and neurological examination performed in our outpatient clinic by three ad hoc specifically trained neurologists (PB, CA, GE, LF) and were screened with face-to-face interviews using a semi-structured questionnaire that was formulated to collect thorough data on lifestyle, behavioral and socio-demographic factors (age, sex, civil status, occupation, body mass index, arterial blood pressure, sport activity, use of coffee, alcohol, smoking, sleep disturbances, menopause, contraceptive use), comorbidities, concomitant medications and clinical features of migraine (disease duration, family history of migraine, presence, frequency, duration of attacks, location, accompanying symptoms, unilateral cranial autonomic symptoms, triggers and alleviating factors, prodromes, postdromes, allodynia, presence and duration of medication overuse, current acute or preventive medications, patient’s satisfaction with triptans) (17). The interview determined whether patients experienced DAs by asking the following question: “During prodromes, headache stage or postdromes do you also have at least one of the following symptoms: yawning, somnolence, nausea, vomiting, mood changes, fatigue or diuresis?”. Patients reporting at least one of the above symptoms during the prodromes, headache stage or postdromes were considered migraine patients with DAs. The institutional review board of IRCCS San Raffaele Pisana approved the protocol developed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. All participants signed informed consent prior to their inclusion in the study.
Statistical analysis
Data are presented as percentages, or mean ± SD (range). Differences between percentages were assessed by chi-square test. Student’s t test was used for normally distributed variables. Mann-Whitney test was employed for non-parametric variables. To quantify the relationship between dopaminergic symptoms and migraine clinical features, multivariate logistic regression analyses were performed by stepwise forwarding to control for multiple confounders. The covariates entered in the model always included attack duration, osmophobia, allodynia, prophylaxis, medication overuse, phonophobia, photophobia, aura, unilateral cranial autonomic symptoms, dopaminergic drugs, gender and physical activity. Only p values were used for testing statistical significance. Only values lower than 0.05 were regarded as statistically significant. Calculations were performed using computer software packages (Statistica 8.0, StatSoft Inc., OK and MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org).
Results
We investigated 1148 migraine patients (F/M: 902/246): 801 were affected by migraine without aura, 60 by migraine with aura, 43 by migraine without aura + migraine with aura and 244 by chronic migraine. Medication overuse was present in 171 patients with chronic migraine.
Migraine patients with and without DAs did not differ for lifestyle, behavioral, socio-demographic factors, concomitant medications and comorbidities, albeit a slightly higher prevalence of affective disorders (p = 0.03) was noticed in migraine patients with DAs (Table 1).
Characteristics of migraine patients with and without dopaminergic symptoms (DAs).

*Student’s t test for normally distributed variables.
§Chi-square test for affective disorders only; p = 0.0298.
A total of 374 patients (32.6%) reported the presence of ≥1 DAs during the attack: 143 patients with DAs (38.2%) described one symptom, 107 (28.6%) two symptoms and 124 (33.2%) ≥3 symptoms. Two-hundred and nine of 374 patients with DAs (55.9%) referred to the co-occurrence of ≥1 pre-synaptic plus ≥1 post-synaptic DAs. The most frequent DA was yawning followed by somnolence, nausea, vomiting, fatigue, mood changes and diuresis (Table 2). DAs occurred during the headache stage in 202 patients (54%), prodromes in 126 (33.7%) and postdromes in 101 (27%).
Type and number of dopaminergic symptoms (DAs) complained of by migraine patients.

No correlation was found between DAs and migraine subtypes. Univariate analysis revealed significant correlations between the presence of DAs and attack duration (p < 0.0001), unilateral cranial autonomic symptoms (p = 0.0002), osmophobia (p < 0.0001) and allodynia (p = 0.0002) (Table 3).
Migraine characteristics: Comparison between patients with or without dopaminergic symptoms (DAs).

**Mann-Whitney test for non-parametric variables.
MO: migraine without aura; MA: migraine with aura; CM: chronic migraine; UAs: unilateral cranial autonomic symptoms.
After adjusting for confounders, multivariate logistic regression analysis revealed that DAs were independently associated with attack duration (OR: 1.82; 95% CI: 1.41–2.36, p < 0.0001), osmophobia (OR: 2.01; 95% CI: 1.50–2.69, p < 0.0001), allodynia (OR: 1.43; 95% CI: 1.10–1.85, p = 0.0071), use of prophylaxis (OR: 0.74; 95% CI: 0.57–0.98, p = 0.033) and presence of unilateral cranial autonomic symptoms (OR: 1.31; 95% CI: 1.01–1.68, p = 0.045) (Table 4).
Multivariate logistic regression analysis of independent determinant of dopaminergic symptoms in 1148 migraineurs.

*Patients were coded as 1/0 if attacks’ duration lasted >24/≤24 hours.
**Prophylactic treatment was coded as 1/0 irrespective of the drugs used.
Covariates included in the model were: Attack duration, osmophobia, allodynia, prophylaxis, medication overuse, phonophobia, photophobia, aura, unilateral cranial autonomic symptoms, dopaminergic drugs, gender and physical activity.
Multivariate logistic regression analysis of independent determinant of pre-synaptic or pre-presynaptic + post-synaptic DAs showed that migraine patients with pre-synaptic DAs were independently associated with increased attack duration (OR: 1.71; 95% CI: 1.21–2.43, p = 0.0026), more frequent allodynia (OR: 1.77; 95% CI: 1.25–2.50, p = 0.0013), and reduced use of prophylaxis (OR: 0.56; 95% CI: 0.38–0.83, p = 0.0035), whereas migraine patients with both pre-synaptic and post-synaptic DAs had prolonged attack duration (OR: 2.01; 95% CI: 1.45–2.77, p < 0.0001), osmophobia (OR: 2.51; 95% CI: 1.78–3.53, p < 0.0001) and allodynia (OR: 1.43; 95% CI: 1.04–1.96, p = 0.027) (Table 5). The six patients showing only post-synaptic DAs showed a trend for medication overuse and a lower frequency of phonophobia (data not shown).
Multivariate logistic regression analysis of independent determinant of pre-synaptic or pre-synaptic + post-synaptic dopaminergic symptoms in migraineurs.

*Patients were coded as 1/0 if attacks’ duration lasted >24/≤24 hours.
Ninety-nine patients were under active treatment with dopaminergic drugs (flunarizine n = 70; neuroleptics n = 12; metoclopramide/domperidone n = 7; DA-agonists n = 10).
**Prophylactic treatment was coded as 1/0 irrespective of the drugs used.
Covariates included in the model were: Attack duration, osmophobia, allodynia, prophylaxis, medication overuse, phonophobia, photophobia, aura, unilateral cranial autonomic symptoms, dopaminergic drugs, gender and physical activity.
Discussion
Migraine is a clinically heterogeneous brain disorder despite its major subdivisions according to headache frequency and presence of aura (18). The search for migraine endophenotypes is still in its infancy but it may be useful not only to unravel pathophysiological mechanisms, but mostly to empower tailored therapy in the modern era of precision medicine (18–21).
In this study, the first specifically designed to evaluate dopaminergic symptoms in a large series of migraine patients attending a tertiary-referral center, we document that DAs are common (32.6%), frequently pre-synaptic (yawning and somnolence), and prevail during the headache stage, when both pre-synaptic and post-synaptic DAs may coexist. Of interest, longer attack duration (OR 1.82), more frequent allodynia (OR 1.43), unilateral autonomic symptoms (OR 1.31), osmophobia (OR 2.01) and a reduced use of migraine preventative drugs (OR 0.74) were all independently associated with DAs.
Dopamine significantly contributes to migraine pathophysiology (6–8). Experimental animal models showed that dopamine behaves as a brake on the rostral transmission of nociceptive inputs as descending fibers originating from the A11 dopaminergic nucleus are capable of reducing the neuronal firing in the trigemino-cervical complex by acting on inhibitory dopamine D2-like receptors (22,23). In humans, pharmacological studies have documented that migraine is characterized by an impairment of dopaminergic neurotransmission, which causes dopamine receptor up-regulation and hypersensitivity to dopamine agonists, a typical migraine hallmark (10,24,25).
DAs may be extremely pronounced in some patients with migraine during the attack, representing a major source of disability and sometimes requiring a specific symptomatic approach. Our study suggests that migraine patients with DAs have probably an even more conspicuous derangement of the dopaminergic neurotransmission compared to those without DAs. In fact, the relevance of DAs during the migraine attack in the former points to a lower activation threshold of both pre-synaptic and post-synaptic dopamine receptors. The sequential appearance of dopaminergic symptoms across the attack progression in migraine patients with DAs is consistent with the hypothesis that during the attack there is a relative increase in the dopaminergic activity in patients with a hypodopaminergic biological trait. Accordingly, during prodromes, a progressive rise in dopamine plasma levels would stimulate hypersensitive, up-regulated pre-synaptic dopamine receptors located in the hypothalamus, producing yawing and somnolence. Such attack-related relative increase in dopaminergic activity would not be sufficient to counteract the innate reduced inhibition exerted by the A11 dopaminergic cells on the trigemino-cervical complex in these patients – hence the activation of the trigemino-vascular system and head pain development – but would indeed stimulate hypersensitive, up-regulated post-synaptic dopamine receptors, originating nausea and vomiting. Other symptoms at least partly related to dopamine receptor stimulation (mood changes, fatigue and diuresis, which often appear in the second part of the migraine storm), could be referred to a scattered regression of dopaminergic activity to the previous interictal level (Figure 1). Our assumption is supported by some pharmacological, biochemical and clinical findings. Acute antagonism at dopamine receptors may stop the attack (26) whereas chronic dopamine receptor stimulation with (non-selective) dopamine agonists such as lysuride and alpha-dihydroergocryptine may prevent migraine (27–29). Further, chronic migraine, pathogenetically considered a never-ending migraine attack (30), is characterized by several-fold higher dopamine plasma levels compared to chronic tension type headache and healthy controls (31). Lastly, the finding in our study of a higher prevalence of affective disorders in migraine patients with DAs compared to those without fits well with the relevance of the dopamine system dysregulation in depressed individuals (32).
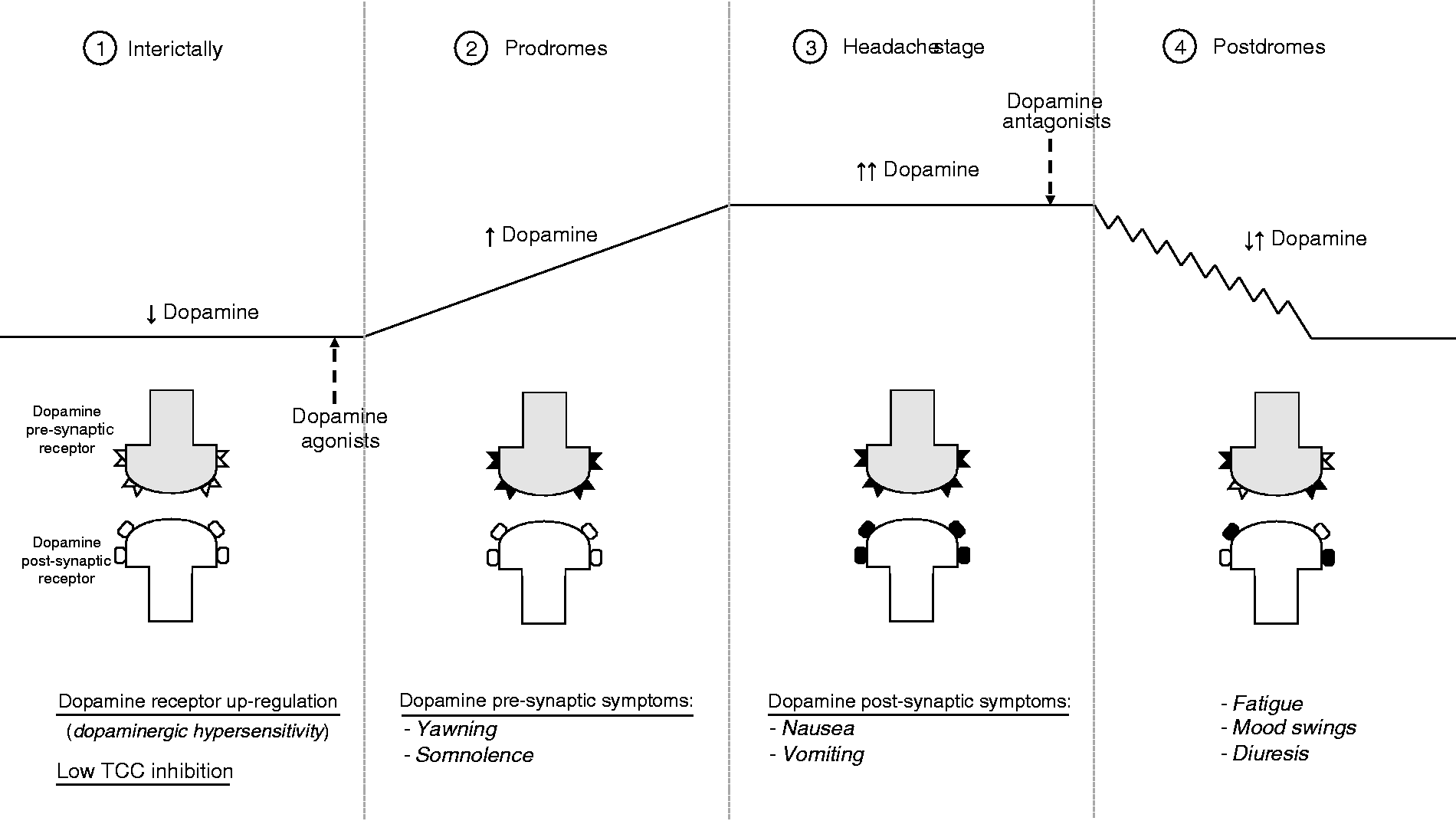
Interictally (1), a low dopaminergic tone would upregulate dopamine receptors and reduce the neuronal firing inhibition at the level of the trigeminal-cervical complex, rendering the patient prone to develop the migraine attack. In the prodromal phase (2), the increased dopaminergic activity would stimulate at very low plasma concentrations the hypersensitive dopamine pre-synaptic receptors, producing yawning and somnolence. During the headache phase (3), increasing dopamine levels would stimulate also dopamine post-synaptic receptors causing nausea and vomiting, while in the prodromal stage (4), dopamine levels would fluctuate, slowly reverting to baseline and sometimes triggering fatigue, mood swings and diuresis. Dopamine agonists would exert a migraine prophylactic effect by increasing the low interictal dopaminergic tone, whereas dopamine antagonists would abort the migraine attack by reducing the attack-related increased dopaminergic activity. TCC: trigemino-cervical complex.
We deem that the complex migraine picture characterizing patients with DAs in the present study (long-lasting attacks associated with allodynia, unilateral cranial autonomic symptoms and osmophobia) may be at least partly explained by a reduced dopaminergic inhibition on the neuronal firing in the trigemino-cervical complex, which allows a full-blown migraine phenotype. Allodynia and unilateral cranial autonomic symptoms, often coexisting in the same subjects (17), are the clinical expression of central and peripheral sensitization, neurophysiological processes resulting from the coupling of an abnormal neuronal excitability with a dysfunctional descending pain modulation (33). Thus, a reduced dopaminergic tone in migraine patients with DAs would facilitate an undisputed firing of trigeminal nociceptive inputs. Cutaneous allodynia is also linked to an imbalance in endogenous dopamine release, as demonstrated by a sudden decrease in the binding of [11C]raclopride (a dopamine D2/D3-selective radiotracer) in the insula in migraine patients following a sustained thermal pain threshold challenge on the trigeminal region (15). Osmophobia is an alteration of the sense of smell, a sensorial function involving primarily the dopaminergic system (34). Osmophobia is characterized by an unbearable perception of non-aversive odors and represents a specific migraine sensory hypersensitivity that affects more than 50% of patients with migraine (35). As osmophobia prevails in migraine patients with longer disease duration, allodynia, anxiety and depression, we suggest that its higher frequency in migraine patients with DAs could be related to the sensitization of the neurolimbic pain network in these patients.
We do not have any reliable explanation for the low use of migraine prophylaxis in individuals with migraine with DAs, an unexpected finding in patients with more disabling migraine attacks. Our tentative, purely speculative hypothesis is that the salience of non-headache symptoms (e.g. gastrointestinal dopaminergic symptoms) in this population might have led to misdiagnosis and to inappropriate treatments.
The main strength of our study is the large patient sample and their thorough demographic and clinical characterization using face-to-face interviews performed by specifically trained neurologists. Limitations include the fact that the study is not a population study – being referred to tertiary care patients – and the potential occurrence of recall bias.
In conclusion, this study helps broaden our knowledge on potential migraine endophenotypes, documenting that one third of migraine patients do present DAs, probably due to a more pronounced derangement of dopaminergic neurotransmission compared to the general migraine population. In migraine patients with DAs, attacks last longer and are particularly disabling not only due to the presence of DAs but also for the occurrence of symptoms related to peripheral and central trigeminal sensitization, namely unilateral cranial autonomic symptoms, allodynia and osmophobia. A lower dopaminergic control on the firing of the trigemino-cervical neuron could be the underlying pathophysiological substrate of this endophenotype. As to therapeutic implications, modulation of the dopaminergic system should be carefully considered in these patients for both acute and preventative treatments in future, ad hoc designed studies.
Clinical implications
Dopaminergic symptoms (DAs) are present in 32.6% of migraine patients during the attack. Migraine patients with DAs have longer attack duration and more frequent osmophobia, allodynia, unilateral cranial autonomic symptoms than those without, but use fewer preventative treatments. The clinical endophenotype of migraine with DAs suggests a reduced inhibition of the firing of trigemino-cervical neurons linked to a lower dopaminergic activity in these patients. Modulation of the dopaminergic system should be considered for both acute and preventive migraine treatment in patients with DAs.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PB received travel grants, honoraria for advisory boards, speaker panels or investigation studies from Alder, Allergan, Bayer, ElectroCore, Eli-Lilly, GSK, Lusofarmaco, MSD, Novartis, Stx-Med, Teva, Visufarma; CA received travel grants from Eli-Lilly, FB-Health, Lusofarmaco and Teva; GE received travel grants and honoraria from Eli-Lilly, Novartis, New Penta and Ecupharma; LF received travel grants and honoraria from Teva, Eli-Lilly and Novartis; FG and PF report no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Italian Ministry of Health (institutional funding ricerca corrente) and by the European Social Fund, PNR 2015-2020 ARS01_01163 PerMedNet under the Italian Ministry of Education, University and Research (CUP B66G18000220005).