
Abstract
Objectives
To estimate remission rates of chronic headache (CH), focusing on potential predictors of headache remission and medication.
Methods
We used data from the longitudinal population-based German Headache Consortium (GHC) Study (n = 9,944, 18–65 years). Validated questionnaires were used at baseline (t0, 2003–2007, response rate: 55.2%), first follow-up after 1.87 ± 0.39 years (t1, 37.2%) and second follow-up after 3.26 ± 0.60 years (t2, 38.8%) to assess headache type and frequency, use of analgesics and anti-migraine drugs, medication overuse, education, BMI, smoking and alcohol consumption. CH was defined as ≥ 15 headache days/month at t0 over three months. Outcomes were: CH remission (<15 headache days/month at both follow-ups), CH persistence (≥ 15 headache days/month at both follow-ups); all others were considered as partially remitted. To estimate predictors of remission, univariate and multiple logistic regression were calculated.
Results
At baseline, 255 (2.6%) participants were identified with CH. Of these, 158 (62.0%) participants responded at both follow-ups. Remission was observed in 58.2% of participants, partial remission in 17.7% and persistence in 24.1%. Remission was associated with female sex (adjusted odds ratio: 3.10, 95% confidence interval: 1.06–9.08) and no medication overuse (4.16, 1.45–11.94) compared to participants with persistent CH; participants with higher headache frequency at t0 were less likely to remit (0.90, 0.84–0.97). Medication, age, education, BMI, smoking and drinking showed no effects on remission. Similar results were observed for partial remission.
Conclusion
The majority of CH participants remitted from CH. Female sex, no overuse of pain medication and lower headache frequency were associated with remission.
Keywords
Introduction
The majority of patients with chronic headache (CH) suffer from chronic migraine with or without concomitant tension type headache (TTH) (1). CH is defined as headache that occurs on 15 or more days per month over three months (2). The prevalence of CH is approximately 1% to 4% in the general population (3–8). The kind of medication intake influences the development of CH (9). CH leads to psychological strain, a decrease in health-related quality of life (10) and socioeconomic consequences due to high direct and indirect costs (11). In order to find associated factors and optimize treatment paradigms, it is important to explore the risk factors of headache frequency in CH. Only a few studies report on remission of CH (12–19). Predictive factors for the remission of chronic migraine have been described as lower baseline headache frequency (17,19), absence of allodynia (19), younger age of onset (17), good compliance with preventive medication, withdrawal from continuous use of analgesics for headache relief, and regular physical exercise (18). Predictors for the persistence of CH included older age, daily headache, CH onset after the age of 32 years, CH duration of six or more years (13) and medication overuse (13–15). Individuals with a low level of education, Caucasians, and previously married (divorced, widowed, separated) people had a reduced likelihood of remission (12). Poor outcome in chronic TTH was associated with coexisting migraine, single status, and sleeping problems (17). The aim of our longitudinal, population-based German Headache Consortium (GHC) Study was to describe remission rates of CH and to identify potential predictors of remission such as age, sex, smoking status, alcoholic beverage consumption, body weight, educational level, and the role of medication intake.
Methods
Study design and study population
A detailed description of the GHC Study was published previously (8). Briefly, the GHC Study is a longitudinal population-based cohort study supported by the German Federal Ministry of Education and Research. The study was approved by the ethics committee of the University of Duisburg-Essen, Germany. Informed written consent was obtained from all participants. About 18,000 men and women were randomly selected from statutory lists of residence in three German cities: Essen, a large town (585,481 residents); Muenster, a medium-sized town (272,890 residents); Sigmaringen, a small town and rural area (16,501 residents). Men and women between 18 and 65 years with German citizenship, to ensure proper knowledge of the German language, were included. The baseline examination (t0) was conducted between 2003 and 2007, first follow-up (t1) after 1.87 years (SD: ± 0.39 years) and second follow-up (t2) after 3.26 years (SD: ± 0.60 years) in relation to baseline. A questionnaire was sent by postal mail to all participants and a reminder was sent two weeks later to reduce nonresponse. Subjects who did not respond were called and received a telephone interview by trained medical students based on the same questionnaire. Subjects were considered nonresponders after eight unsuccessful phone calls, or if they refused participation. For data analysis, we included all participants with CH at t0 and known headache frequency at t1 and t2. Figure 1 shows the flowchart of the study population.
Flow chart of the study population, n (%).
Questionnaire
The questionnaire was based on the ICHD-2 classification criteria of The International Headache Society (IHS) (2). A validation and detailed description had been published previously (20,21). The questionnaire included questions about personal data, the medical history regarding migraine and TTH, number of headache days, intake of acute pain or headache medication, lifestyle (smoking, drinking, BMI) and socioeconomic status basing on education to avoid direct questions about income.
Diagnostic criteria
Firstly, we used modified IHS criteria (2) to define characteristics of headache: CH was defined according to the IHS criteria as headache present on ≥ 15 days/month over three months. Episodic headache was defined as headache present on < 15 days/month (2). Overuse of pain medication was defined as intake of analgesics or anti-migraine drugs on 10 or more days per month. Definitive migraine was defined as (a) headache attacks lasting untreated or unsuccessfully treated for 4–72 hours; (b) headache characteristics must be accompanied by at least two of the following symptoms: Unilateral location, pulsating quality, moderate or severe pain intensity, aggravation by or causing avoidance of routine physical activity (e.g., walking or climbing stairs); (c) during headache episodes at least one of the following conditions must be reported: Nausea and/or vomiting, photophobia and phonophobia; (d) attacks do not fulfill criteria for TTH (see below). Probable migraine was defined as attacks fulfilling all but one of criteria (a), (b) and (c) for definitive migraine and not fulfilling the criteria for TTH. Definitive TTH was defined as (e) headache lasting from 30 minutes to 7 days; (f) headache characteristics must be accompanied by at least two of the following symptoms: bilateral location, pressing/tightening (non-pulsating) quality, mild or moderate intensity, not aggravated by routine physical activity such as walking or climbing stairs; (g) both of the following: No nausea or vomiting (anorexia may occur), no more than one of photophobia or phonophobia; (h) episodes do not fulfill the criteria for migraine. Probable TTH was defined as episodes fulfilling all but one of criteria (e), (f) and (g) for TTH and not fulfilling the criteria for migraine.
Secondly, we combined the above-defined headache characteristics to classify seven headache subtypes at t0:
Chronic migraine with medication overuse: Participants who met modified ICHD2 criteria for definitive or probable migraine and who reported CH with medication overuse. Chronic migraine without medication overuse: Participants who met modified ICHD2 criteria for definitive or probable migraine and who reported CH without medication overuse. Chronic TTH with medication overuse: Participants who met modified ICHD-2 criteria for definitive or probable TTH and reported CH with medication overuse. Chronic TTH without medication overuse: Participants who met modified ICHD-2 criteria for definitive or probable TTH and reported CH without medication overuse. Chronic migraine with concomitant TTH with medication overuse: Participants who met modified ICHD-2 criteria for definitive or probable migraine and fulfilled the criteria for TTH and who reported CH with medication overuse. Chronic migraine with concomitant TTH without medication overuse: Participants who met modified ICHD-2 criteria for definitive or probable migraine and fulfilled the criteria for TTH and who reported CH without medication overuse. Unclassified chronic headache: The remaining participants with CH who did not meet criteria for chronic migraine, chronic TTH or chronic migraine with concomitant TTH.
Definition of outcome variables
The outcome variable was remission or persistence of CH as defined by headache frequency at t0, t1 and t2:
Persistent CH: Participants who met CH criteria at t0, t1 and t2. Remitted CH: Participants who met CH criteria at t0 and episodic headache criteria at t1 and t2. Partially remitted CH: Participants who met CH criteria at t0 and episodic headache criteria at t1 or t2.
Definition of exposure variables
Intake of medication at t0 was categorized into the subgroups of no medication, single analgesics and combination analgesics. The single analgesics subgroup was defined as intake of one main active agent: NSAIDs (ibuprofen, acetylsalicylic acid and diclofenac), paracetamol/acetaminophen and metamizole. The combination analgesics subgroup was defined as intake of at least two combined active agents: Acetylsalicylic acid, paracetamol/acetaminophen and caffeine; paracetamol/acetaminophen and codeine; and acetylsalicylic acid and paracetamol/acetaminophen.
Only one participant with CH reported intake of triptans, one participant intake of a beta blocker for prophylactic medication (according to the guidelines of the German Neurological Society (22)) and none reported intake of ergots or barbiturates. For this reason, we were unable to investigate this kind of medication.
Further, we defined overuse of pain medication as intake of analgesics or anti-migraine drugs on 10 or more days per month. Drinking was defined as daily or almost daily consumption of alcoholic beverages and no drinking as no or casual consumption of alcoholic beverages. Smoking was defined as current smoking or having quit smoking within the last 12 months, and no smoking was defined as never having smoked or past smoking. Body mass index (BMI) was categorized as normal (BMI < 25 kg/m2), overweight (≥ 25 – < 30 kg/m2) and obese (≥30 kg/ m2). High education was defined as general qualification for university entrance or completion of university, and low education as any other response.
Statistical analysis
Descriptive statistics were used to determine rates of CH remission. Univariate and multiple logistic regression analyses were computed to assess predictors of remission or partial remission by estimating the odds ratio (OR) and their corresponding 95% confidence interval (95% CI). Crude OR and 95% CI were separately estimated for age (years), sex, headache days per month at t0, medication overuse, kind of medication intake, education, smoking, drinking, and BMI. In model 1, adjusted ORs were estimated for sex, headache days/month and medication overuse. All analyses were carried out using SAS 9.4 (Statistical Analysis System Corp., Cary, NC, USA).
Results
Response
Of the 18,000 individuals surveyed, we obtained baseline information for 9,944 participants (response rate: 55.2%). Detailed information of the population characteristics have been reported previously (23). A total of 255 respondents (2.6%) reported CH at t0. Of these, we obtained follow-up information about headache frequency from 158 (62.0%) participants (Figure 1). Analyses of possible differences between responders (66.5% women, 45.8 ± 13.2 years, 21.4 ± 6.3 headache days/month at t0) and nonresponders (n = 97, 62.9% women, 45.3 ± 15.4 years, 22.4 ± 5.7 headache days/month at t0) reveal no differences in regard to proportion of women, age and amount of headache days/month at baseline.
Characteristics of the study population at baseline
Characteristics of the study population.
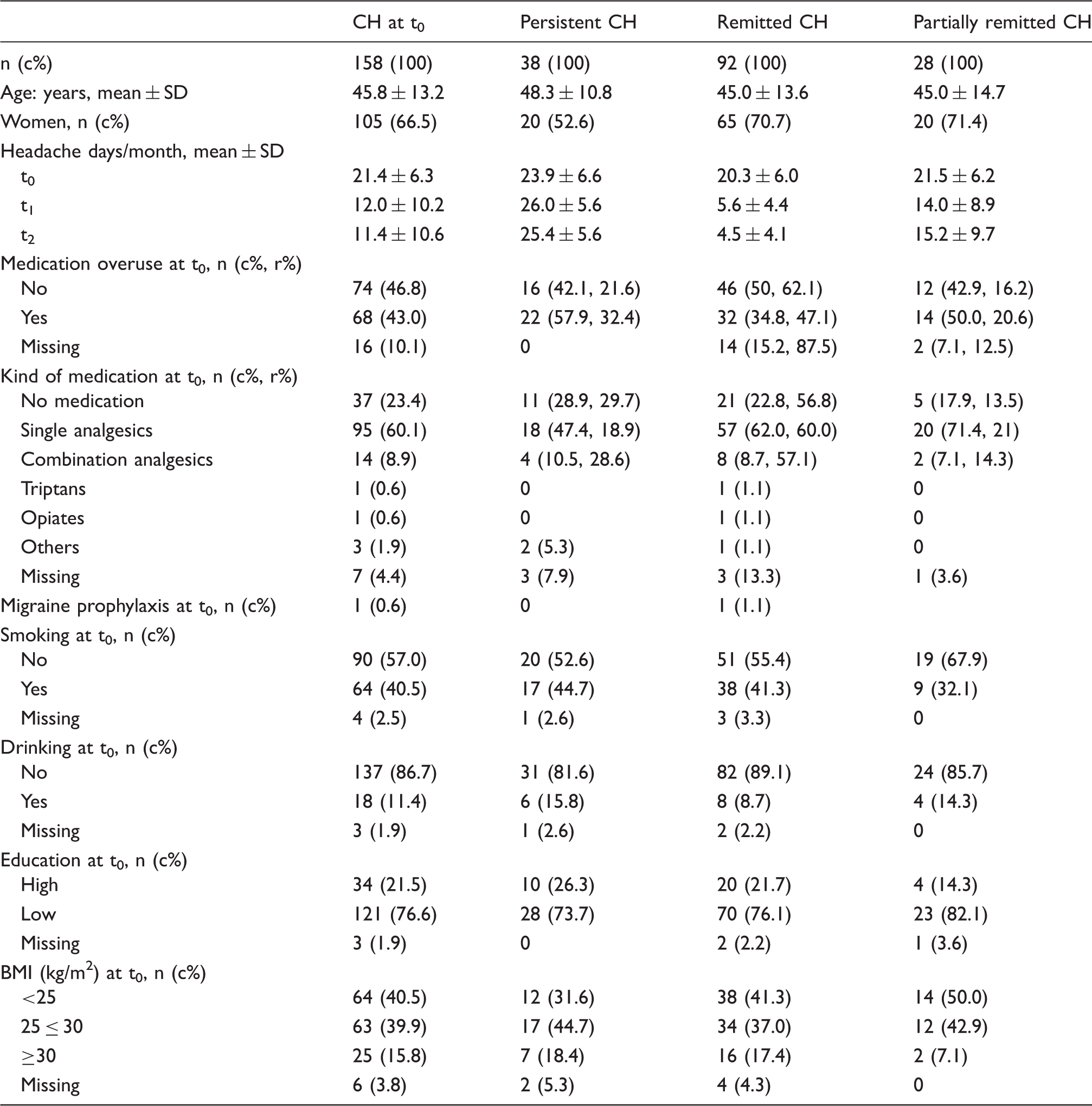
CH: Chronic headache; t0: Baseline; t1: First follow-up; t2: Second follow-up; c%: Column percent; r%: Row percent; BMI: Body Mass Index; TTH: Tension-type headache; MIG+TTH: Migraine with concomitant tension-type headache.
CH subtypes and medication overuse
Chronic headache (CH) subtypes and medication overuse (MO).
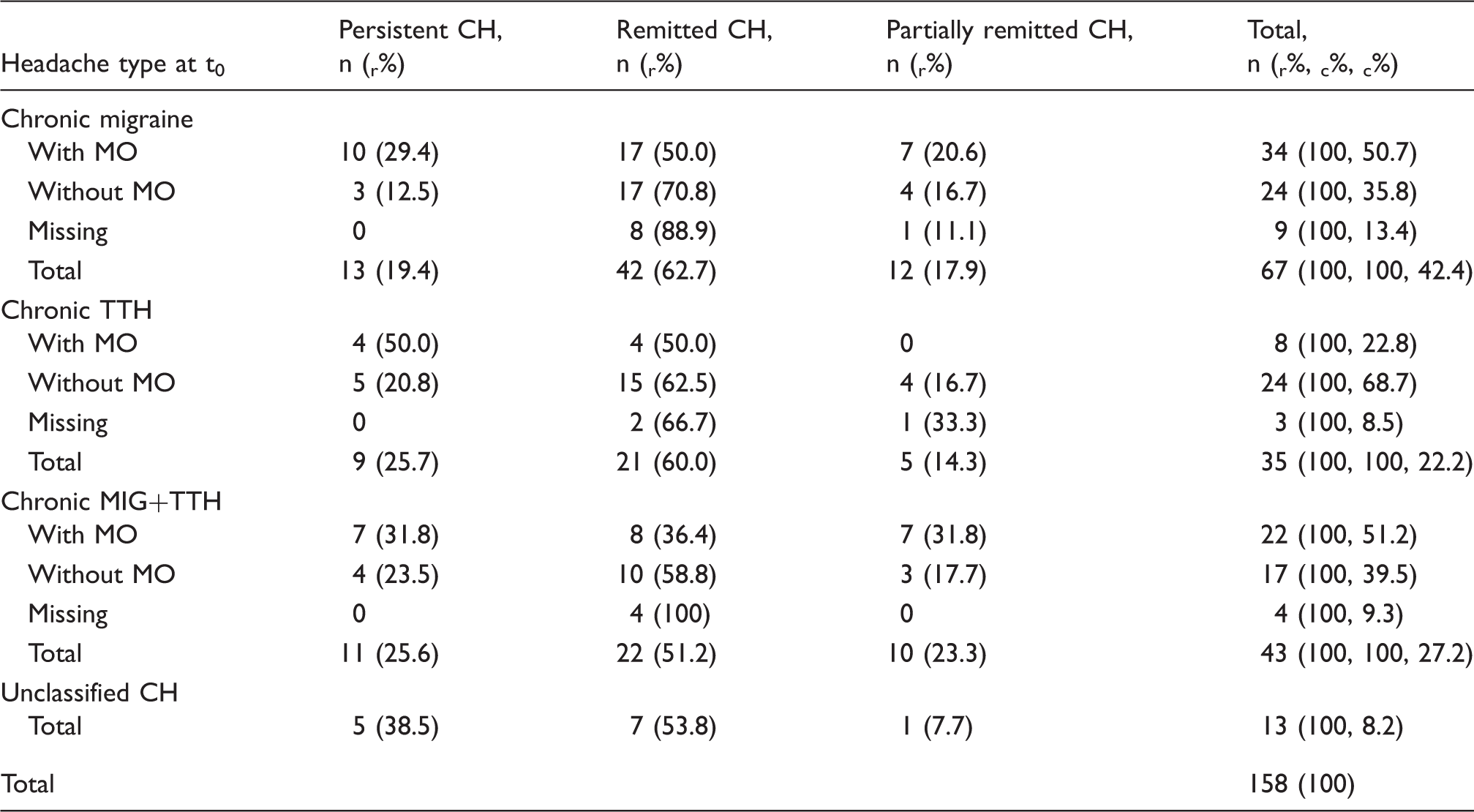
CH: Chronic headache; MO: Medication overuse; t0: Baseline; r%: Row percent; c%: Column percent; TTH: Tension-type headache; MIG+TTH: Migraine with concomitant TTH.
Remission rates and comparisons between remitted and persistent CH
Remission was reported by 92 participants (58.2%), while 38 (24.1%) suffered from persistent CH. Remitted CH in at least one of the follow-up surveys (partially remitted CH) was reported in 28 (17.7%) cases (Figure 2). Considering the different headache types, Table 2 shows the highest remission rates in participants with chronic migraine (62.7%) and chronic TTH (60.0%), whereas 51% of the participants with migraine and concomitant TTH showed remission. Considering medication intake, the remission rate was higher in participants without medication overuse regardless of headache subtype (migraine: 70.8%, TTH: 62.5%, migraine with concomitant TTH: 58.8%). Irrespective of headache type, remission from CH was more often reported in cases with no medication overuse at t0 compared to medication overuse (62.1% resp. 47.1%). Remission of CH was similar in participants taking no pain medication (56.8%), single analgesics (60.0%) and combination analgesics (57.1%).
Transition rates relative to chronic headache (CH) status at baseline.
We observed specific differences between participants with persistent and remitted resp. partially remitted CH (Table 1). Remitted and partially remitted CH participants were younger and more likely to be women compared to the persistent CH group (remitted: 70.7% women, 45.0 years; partially remitted: 71.4% women, 45.0 years; persistent: 52.6% women, 48.3 years). They had a lower headache frequency at t0 (remitted: 20.3 headache days/month, partially remitted: 21.5 days/month, persistent: 23.9 days/month). Participants with remitted CH reported medication overuse less often at t0 than participants with persistent CH (34.8% vs. 57.9%). A higher percentage of participants with remitted CH used single analgesics at t0 compared to those with persistent CH (62.0% vs. 47.4%). For partially remitted CH it was even higher, at 71.4%. There were no major differences in smoking, drinking, education or BMI.
Predictors of remission
Logistic regression models to identify potential promoting factors for chronic headache (CH) remission.
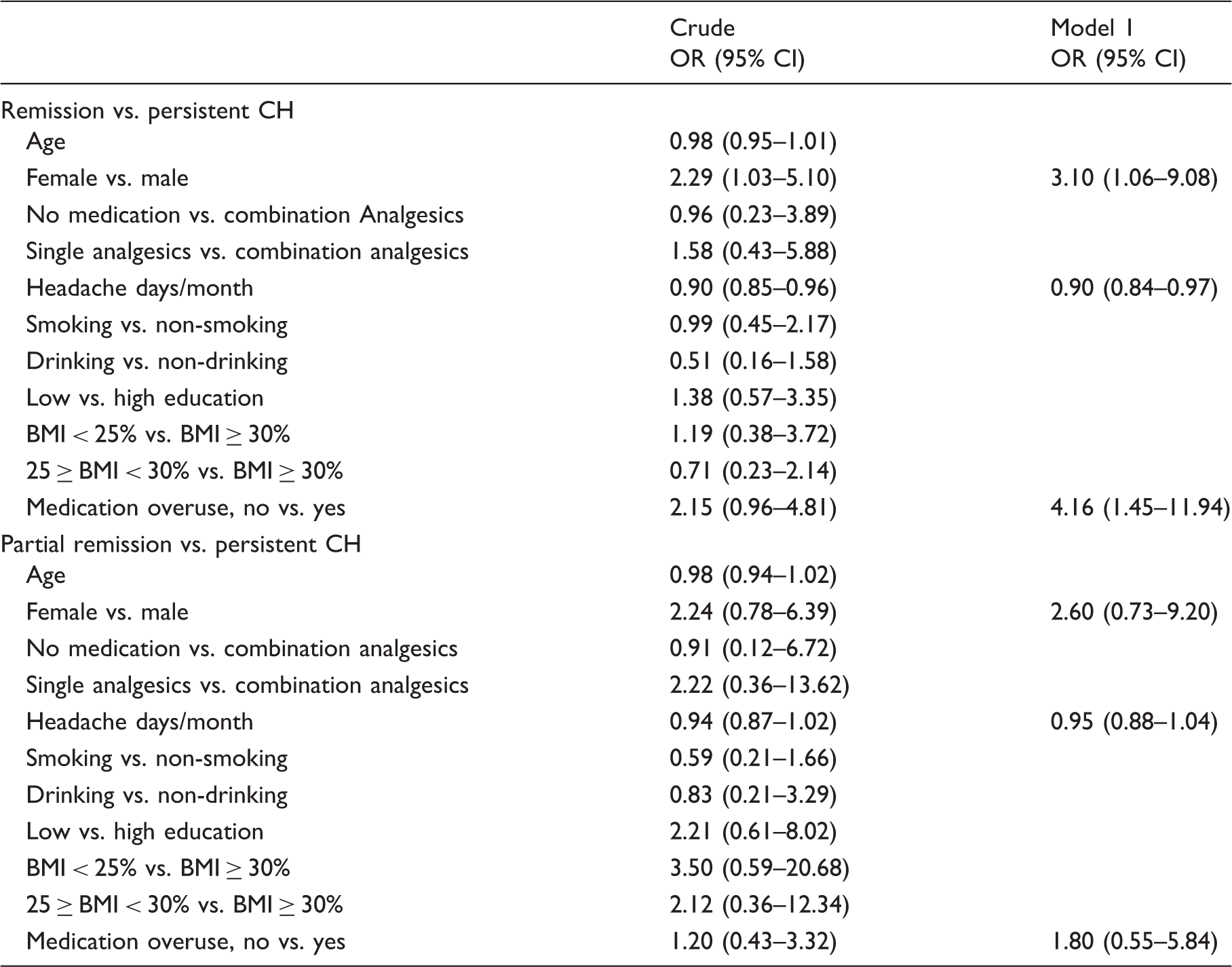
CH: Chronic headache; OR: Odds ratio; 95% CI: 95% confidence interval; BMI: Body Mass Index.
Model 1: Adjusted for sex, headache days/month and medication overuse.
Discussion
In our population-based GHC Study we found a prevalence of CH of 2.6%, and a high remission rate from CH of 58%. Only 43% of participants with CH reported an intake of analgesics or anti-migraine drugs on 10 or more days/month (medication overuse) despite a mean headache frequency of 21.4 days/month. Only 32% of participants with medication overuse and 21% without medication overuse had persistent CH over three years. Participants without pain medication overuse were more likely to remit from CH. Most participants used single analgesics (60%). Using preventive medication and triptans was rather uncommon. Remission was not related to the type of medication used (none vs. single vs. combination analgesics). Remission rates were higher for women and for participants with lower baseline headache frequency.
The prevalence of our study cohort is fully comparable to previous studies from the USA and Europe, with prevalence ranging between 1% and 4% (3–7, 16). Studies investigating elderly people (≥65 years) (14,24) and adolescents (12–14 years) (25,26) also revealed similar prevalence rates. These results suggest that the prevalence of CH may be consistent in different populations as well as population subgroups.
Of 158 participants with CH at t0 and known headache frequency at both follow-ups, more than half (58%) remitted from CH and only one quarter (24%) had persistent CH; the remaining 18% of participants were at least partially remitted from CH. Our findings show that most CH participants remit to an episodic pattern. Other studies with different definitions for remission and study size report remission rates ranging as low as 26% and as high as 65% (12–14,19). For example, the large longitudinal American study including 1,134 participants with CH, reported a one-year remission rate of 57%, which compares favorably with our results (12).
Participants reporting no medication overuse were more likely to remit from CH compared to participants with medication overuse regardless of headache subtype. This was also reported previously (13-15). In regard to the kind of medication used (none vs. single vs. combination analgesics) we could not find a clear result. This is in line with our previous results where we could not find differences in prognosis regarding headache frequency comparing intake of combinations of aspirin with caffeine vs. aspirin alone or no analgesics (28). Since only one participant with CH reported the use of triptans and only one was on prophylactic medication, we were unable to evaluate the impact of this kind of medication on remission rates.
The surprisingly low intake of triptans or prophylactic medication in our study indicates a potentially insufficient delivery of medical treatment to CH patients in Germany. It has already been shown that the lack of a proper migraine treatment could lead to significant medication overuse of simple and combination analgesics (29–31). Patients suffering from CH improved after being detoxified and receiving prophylactic treatment (18,32), and good compliance with preventive medication was shown to have positive effects on remission (18). Awareness of this problem and better access to headache management are both highly relevant.
On the other hand, our studies show that only 30% of participants with medication overuse presented persistent CH over three years, whereas most participants at least changed to episodic headaches. There seems to be a high “natural” remission rate from CH with medication overuse, at least in the general population. Also, persistence of CH without medication overuse was very low (21.6%). A recent review about the therapy of medication overuse headache (MOH) showed that early discontinuation of medication overuse alone does not lead to the best possible outcome, but introducing preventive medication into the therapy of MOH improved the outcome (33). Overall, concepts to improve identification and treatment of patients with CH are necessary.
We also examined different factors predicting remission. Sex seems to be a predictor, as in our study women more often remitted from CH. This gender effect was also reported in an American study where the likelihood of remission increased with age for women but not for men (12). Two studies that investigated adolescents reported a higher remission in boys (15,34). Perhaps sex may have a different impact on remission in different age groups, potentially related to hormonal influences.
In our study, we found an association between lower baseline headache frequency and remission from CH, reconfirming previous reports (17,19).
In the literature, it was also reported that younger age, higher education (12), higher socioeconomic status (27,35) and no obesity (6,12,27) might have positive effects on remission of CH. In our study, age, education, BMI, smoking and alcoholic beverage consumption did not seem to influence remission.
Participants with chronic migraine and chronic TTH had a similar remission rate (62.7% vs. 60.0%), whereas the remission rate of chronic migraine with concomitant TTH was a little lower (51.2%). In the literature, the remission rate from chronic migraine ranged between 26% (19) and 70% (18). For chronic TTH, a remission rate of 45% was reported previously (17). A reason for the different remission rates could be the different definition of persistence and remission in the studies and the different ways of classification in headache subtypes. In our study, the subclassification was not very exact, as the participants were only asked once about their headache characteristics, at t0. The remission rate of chronic migraine and chronic TTH depends on the definition of remission and the accuracy of the diagnosis of the headache type, but we did not find relevant differences.
An important methodological issue needs to be addressed. In comparative interview/prospective diary studies it was reported previously that CH is over-reported and episodic headache is underreported (36). This could also be the case in the present study.
Strengths of our study are: The representative, large sample size of patients with CH, which provided enough power to test a number of predefined covariates; the large-scale population-based longitudinal design with participants from three different regions of Germany; and the use of a validated questionnaire.
Our study certainly has several limitations. All acquired information depends on self-reported data rather than clinical assessment, so that diagnostic uncertainty cannot be excluded completely. Our questionnaire was based on ICHD-2 classification, in the meantime there is now an actualized version (ICHD-3 beta) (37). Although our response rate of 55.2% at t0 and 37.2% resp. 38.8% at t1 and t2 is comparable to other large-scale population-based studies in Western Europe and the USA, selection bias cannot be excluded. Even though our study focused on baseline variables as predictors of later outcome, assessing the influence of changing patterns of treatment would be of great interest for future analysis. Unfortunately, our study population was too small for this kind of investigation. None of these limitations are unique to our study.
Conclusion
Our study shows a prevalence of 2.6% of CH, and it demonstrates that the vast majority of CH participants remitted from CH, so prognosis was generally good regardless of medication overuse. However, participants without overuse of pain medication were more likely to remit from CH. Prognosis for remission was better for women and participants with lower headache frequency. We could not find an effect of the type of medication (none vs. single vs combination analgesics), age, weight, education, smoking nor drinking alcoholic beverages. As most of the participants with CH did not receive any specific headache treatment or prophylactic medication, better identification and treatment of patients with CH in clinical care seems to be necessary. There remains a highly relevant question of which exact medication and which additional factors might support the remission of CH.
Clinical implications
Prognosis of chronic headache is generally good regardless of overuse of pain medication. Prognosis of chronic headache in patients without overuse of pain medication is better than with overuse. Better identification and treatment of patients with chronic headache is necessary.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Zaza Katsarava received honoraria from Allergan, Amgen, Böhringer-Ingelheim. Mark Obermann received scientific support and/or honoraria from Biogen Idec, Novartis, Sanofi-Aventis, Genzyme, Pfizer, Teva and Heel. He received research grants from Allergan, Electrocore, Heel, and the German Ministry for Education and Research (BMBF).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the German Federal Ministry of Education and Research.