
Abstract
Objective
We performed a systematic review on the comorbidities of familial/sporadic hemiplegic migraine (F/SHM) with seizure/epilepsy in patients with CACNA1A, ATP1A2 or SCN1A mutations, to identify the genotypes associated and investigate for the presence of mutational hot spots.
Methods
We performed a search in MEDLINE and in the Human Gene Mutation and Leiden Open Variation Databases for mutations in the CACNA1A, ATP1A2 and SCN1A genes. After having examined the clinical characteristics of the patients, we selected those having HM and seizures, febrile seizures or epilepsy. For each gene, we determined both the frequency and the positions at protein levels of these mutations, as well as the penetrance of epilepsy within families.
Results
Concerning F/SHM-Epilepsy1 (F/SHME1) and F/SHME2 endophenotypes, we observed a prevalent involvement of the transmembrane domains, and a strong correlation in F/SHME1 when the positively charged amino acids were involved. The penetrance of epilepsy within the families was highest for patients carrying mutation in the CACNA1A gene (60%), and lower in those having SCN1A (33.3%) and ATP1A2 (30.9%) mutations.
Conclusion
Among the HM cases with seizure/epilepsy, we observed mutational hot spots in the transmembrane domains of CACNA1A and ATP1A2 proteins. These findings could lead to a better understanding of the pathological mechanisms underlying migraine and epilepsy, therein guaranteeing the most appropriate therapeutic approach.
Introduction
More than a century of investigation has found that seizures and migraine can co-occur in affected individuals and families, and there is much evidence that these diseases also share genetic susceptibility (1). In both epilepsy and migraine with aura (MwA), susceptible brain regions are hyperexcitable and attacks are believed to begin with hypersynchronous neuronal firing. The involvement of this mechanism in migraine without aura (MwoA) is less clear (1). Moreover, the mechanisms responsible for neuronal hypersynchronous activity are also not well understood. However, genetically determined dysfunction of ion transporters seems to indicate a common underlying mechanism for both paroxysmal disorders. In fact, over the last two decades, the mutations in the ion transportation genes CACNA1A, ATP1A2 and SCN1A have been identified in familial hemiplegic migraine (FHM) (2–4). The prevalence of epilepsy in FHM has been estimated to be around 7% (5), while among patients with sporadic HM (SHM), in which recently an increasing number of CACNA1A and ATP1A2 mutations have been reported, its value is unknown. Though the underlying pathophysiological mechanisms of these associations are not well understood, it is evident that in these patients DNA variants are able to confer susceptibility to both HM and seizure/epilepsy (6). Different questions are still unanswered regarding the presence of epilepsy in HM patients, including the possible presence of a specific genotype related to this endophenotype, its penetrance within families, and the clinical characteristics of these patients. Since these items have not yet been investigated, we have here performed a systematic review on these comorbidities. The results drawn from our analysis add insight that can improve our capacity to predict, to diagnose, and manage patients with HM and epilepsy.
Materials and methods
Search strategy and study selection
We followed PRISMA 2009 guidelines for systematic review and meta-analysis (7). We sought to identify all published studies on the association between HM and seizure/epilepsy in patients or families carrying mutations in one of the HM genes. A search on MEDLINE (Ovid, New York, NY) from September 1993 to January 2016 was performed covering the time from the identification of the first FHM gene (4). No language restrictions were applied. The MEDLINE search strategy included both subject headings (MeSH terms) and text words for the target condition, including: FHM AND epilepsy; FHM AND seizure; HM AND epilepsy; HM and seizures; CACNA1A AND seizure/epilepsy; ATP1A2 AND seizure/epilepsy; and SCN1A AND seizure/epilepsy. We also searched reference lists and relevant journals not indexed in MEDLINE or EMBASE. Additionally, we searched in the Human Gene Mutation Database (HGMD, http://www.hgmd.cf.ac.uk/ac/index.php) and Leiden Open Variation Database (LOVD, http://www.lovd.nl/3.0/home) for mutations in the CACNA1A, ATP1A2 and SCN1A genes and their related phenotypes. We considered DNA variants as “mutations” when 1) functionally characterized and/or 2) segregated with the disease and/or 3) de novo variants. We also reviewed three publicly accessible variant resources to exclude polymorphisms (considering a Minor Allele Frequency <0.002): db SNP at http://www.ncbi.nlm.nih.gov/SNP/; ExAC Browser at http://exac.broadinstitute.org/ and Exome Variant Server at http://evs.gs.washington.edu/EVS/.
Inclusion and exclusion criteria
Published studies and cases from the HGMD/LOVD were included if they reported an association between HM and seizure/epilepsy and their mutations were identified. We excluded review articles, editorials, commentaries, hypothesis papers, letters with no new data, as well as abstracts.
Data extraction
Two review authors independently extracted data; disagreements were resolved by discussion or referring to a third author. We collected data on genotype (DNA mutation), protein modification and patient information related to HM, headache, seizure, epilepsy and other neurological phenotypes, such as intellectual disability (ID), ataxia, and coma.
Data synthesis
For each gene, we selected the mutations associated with HM and seizure/epilepsy, so as to determine the relative frequencies of these mutations among all known mutations for that specific gene. Moreover, we calculated the penetrance (within a family, the percentage of individuals having a gene mutation and exhibiting epilepsy) of HM, seizure/epilepsy and other neurological phenotypes (ID, ataxia, coma). We also plotted the mutations in each protein structure regarding their locations in the transmembrane, extracellular or cytoplasmic domains (Figure 1). We performed a Chi-square test to investigate for associations between mutation location and phenotype.
The figure illustrates the distribution of all the mutations leading to HM in the three protein channels (CACNA1A, ATP1A2, SCN1A). The numbers inside the circles correspond to mutations, which are listed in a rising numerical order in the legend. Mutations associated with HM and epilepsy are shown as black circles, while those associated with HM are shown in white. The reference transcripts used for the CACNA1A gene is NM_001127221.1, for ATP1A2 is NM_000702.3, and for SCN1A is NM_001165963.1.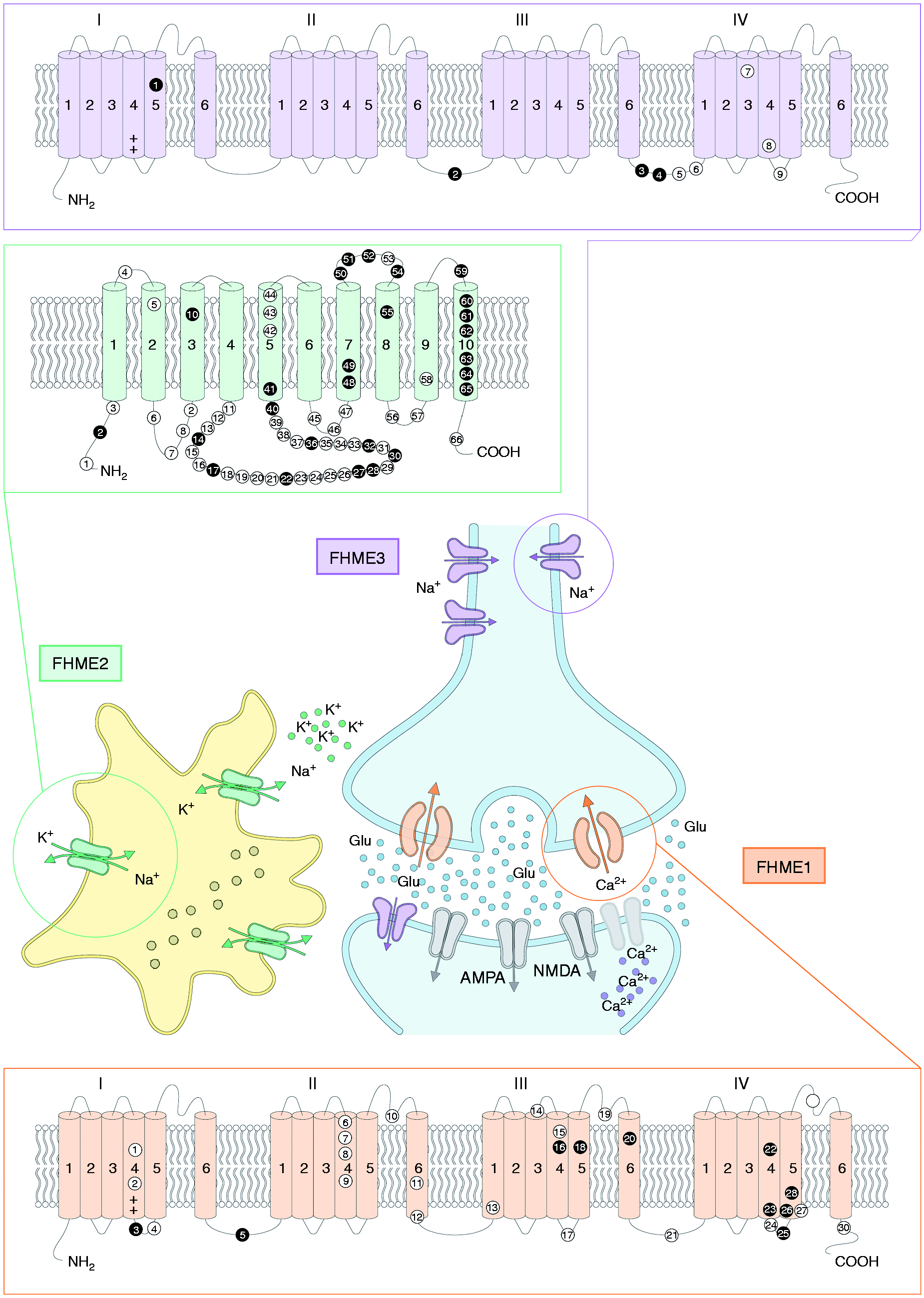
Results
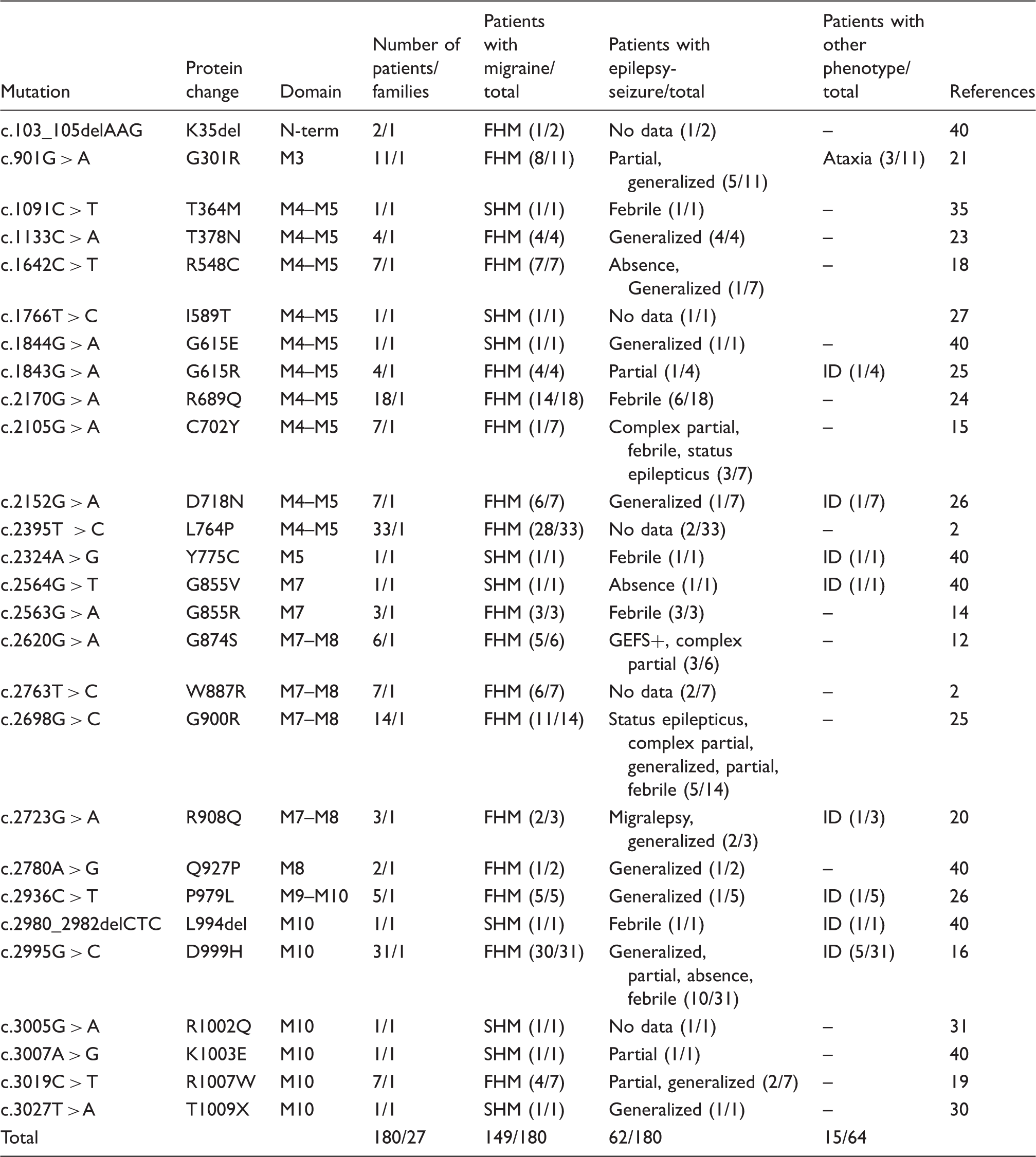
List of the CACNA1A gene (NM_001127221.1) mutations associated with HM/epilepsy, and clinical characteristics of patients.

Abbreviations: FHM, familial hemiplegic migraine; SHM, sporadic hemiplegic migraine; GEFS+, Generalized epilepsy with febrile seizures plus; ID, intellectual disability. “No data” refers to the absence of a detailed clinical description, but the patient had epilepsy.
List of the ATP1A2 gene (NM_000702.3) mutations associated with HM/epilepsy, and clinical characteristics of patients.
Abbreviations: FHM, familial hemiplegic migraine; SHM, sporadic hemiplegic migraine; GEFS+, Generalized epilepsy with febrile seizures plus; ID, intellectual disability. “No data” refers to the absence of a detailed clinical description, but the patient had epilepsy.
List of the SCN1A gene (NM_001165963.1) mutations associated with HM/epilepsy, and clinical characteristics of patients.

Abbreviations: FHM, familial hemiplegic migraine; SHM, sporadic hemiplegic migraine; GEFS+, generalized epilepsy with febrile seizures plus; ID, intellectual disability.
F/SHM1 and CACNA1A
Families and patients
Our search found 33 patients belonging to 23 families. In particular, 15 patients belonged to five families and 18 were sporadic cases. Of the former 15 patients, only nine had epileptic comorbidity, so the total number of patients having HM and epilepsy (here defined as F/SHME1, Familial/Sporadic Hemiplegic Migraine and Epilepsy type 1) was 27, nine familial (9/27, 33.3%) and 18 sporadic (18/27, 66.6%) (Table 1).
Mutation type and its distribution
We found 10 different CACNA1A variants associated with HM and seizures/epilepsy (Table 1). The 10 variants were all missense, the most frequent being S218L, which lies in the 3rd cytoplasmic domain, and was encountered in 10/27 patients (37%). The other nine variants produced a random distribution at the genomic level whereas, at the protein level, two were localized in the 4th and 12th cytoplasmic domains, while the remaining seven variants were all localized in the transmembrane domains III and IV (7/10, 70%); in fact, none of the mutations in the I and II transmembrane domains led to either seizure or epilepsy (p < 0.01). Nine out of 10 patients having S4 segment involvement showed a substitution of either an Arginine (R) or Lysine (K) (positively charged amino acid) with another neutral amino acid (Q, Glutamine; W, Tryptophan).
Mutation frequency and penetrance of seizures/epilepsy
The overall frequency of mutations associated with HM and seizure/epilepsy was 10/154 (6.5%), where 154 was the total number of mutations reported in the HGMD/LOVD for the CACNA1A gene related to three different phenotypes: Episodic Ataxia type 2 (EA2), Spinocerebellar Ataxia type 6 (SCA6), and FHM1. Of these 154 mutations, 30 were associated with HM (sporadic or familial) (legend of Figure 1), resulting in a frequency of HM mutations associated with seizure/epilepsy equal to 33.3% (10/30). This frequency was unexpectedly high considering the low number of patients, as these mutations are generally associated with severe phenotypes (HM and ataxia or HM, ataxia, and ID) in SHM cases. Regarding the penetrance of epilepsy, we found it to be 60%, particularly high, even though it was calculated on the basis of few familial cases.
Clinical description
Summary of the results from this review. Abbreviations: GEFS+, generalized epilepsy febrile seizures plus; ID, intellectual disability; HM, hemiplegic migraine; FHME, familial hemiplegic migraine and epilepsy; SHME, sporadic hemiplegic migraine and epilepsy.

F/SHM2 and ATP1A2
Families and patients
We found 180 patients belonging to 27 families. In particular, 171 patients belonged to 18 families, while nine patients were sporadic cases. Of the 171 patients, 53 had epileptic comorbidity, so that the total number of patients having HM and epilepsy (here defined as F/SHME2, Familial/Sporadic Hemiplegic Migraine and Epilepsy type 2) was 62, 53 familial (53/62, 85.5%) and nine sporadic (9/62, 14.5%) (Table 2).
Mutation type and its distribution
We found 27 different ATP1A2 variants associated with HM and seizures/epilepsy (Table 2). Of these variants, two were small deletions, and the remaining 25 single nucleotide substitutions led to missense mutations. The mutations associated with seizure/epilepsy were located in the transmembrane (11/27, 41%), cytoplasmic (11/27, 41%) or extracellular domains (5/27, 18%). This finding was in contrast to the distribution of mutations observed in FHM2. In fact, of the 66 mutations responsible for FHM2 (legend of Figure 1), 43 were located in the cytoplasmic domains (43/66, 65.2%), while only 15/66 (22.7%) and 8/66 (12.1%), were situated in one of the 10 transmembrane domains or in the extracellular domains, respectively. Moreover, 11/15 (73,3%) mutations affecting the transmembrane domains were associated with epilepsy, compared with only 16/51 (31%) of those outside the transmembrane domains (p < 0.05) (Figure 1).
Mutation frequency and penetrance of seizures/epilepsy
The overall frequency of mutations associated with seizure/epilepsy was 27/73 (36.9%), where 73 was the total number of mutations reported in the HGMD/LOVD for the ATP1A2 gene related to migraine or HM phenotypes. Of these 73 mutations, 66 were associated with HM (sporadic or familial) (legend of Figure 1), resulting in a frequency of ATP1A2 mutations associated with HM and seizure/epilepsy equal to 40.9% (27/66), while the median penetrance of epilepsy was calculated to be 30.9% within the 18 families.
Clinical description
The epileptic phenotype appeared to be mostly of a generalized type, and in eight families it was reported to be triggered by fever. Ataxia was present in three patients belonging to the same family and was associated with the G301R mutation, whereas ID was observed in both the sporadic (three patients) and familial cases (four patients belonging to four families), with an overall frequency of 11.3% (7/62 patients) (Table 4).
FHM 3 and SCN1A
Families and patients
We found 45 patients belonging to seven families (100% of familial cases). A total of 15 patients had the epileptic comorbidity endophenotype here defined as FHME3 (Familial/Sporadic Hemiplegic Migraine and Epilepsy type 3) (Table 3).
Mutation type and its distribution
We found four different SCN1A mutations associated with HM and seizures/epilepsy (Table 3). All four DNA variants were single nucleotide substitutions leading to missense mutations. The L263V mutation was located in a transmembrane domain (IS5), whereas the T1174S, Q1489K and Q1489H mutations were located in the IIS6-IIIS1 and IIIS6-IVS1 cytoplasmic domains, respectively. However, the T1174S variant needs to be considered with caution, since there isn’t a definitive conclusion about its clinical significance.
Mutation frequency and penetrance of seizures/epilepsy
The overall frequency of SCN1A mutations associated with HM and epilepsy was 4/852 (0.47%), with 852 being the total number of mutations reported in the HGMD/LOVD for the SCN1A gene associated with different phenotypes (FHM3, Dravet syndrome, generalized epilepsy with febrile seizures plus (GEFS+), febrile seizures). To date, only nine SCN1A mutations associated with FHM3 have been described (Figure 1 and legend) (3, 8–10, 41–44); therefore the relative frequency of SCN1A mutations associated with HM and seizure/epilepsy was 44.4% (4/9), with a median penetrance of the epilepsy within these families of 33.3%.
Clinical description
L263V was more often associated with generalized epilepsy, while patients with T1174S or Q1489K mutations had focal seizures plus febrile seizures. Finally, the two patients with Q1489H mutation had partial epilepsy with occasional secondary generalization (childhood benign epilepsy), complicated by elicited repetitive daily blindness. There were no reported cases of ataxia or ataxia/ID in these families (Table 4).
Discussion
After having reviewed the cases of patients with HM and seizures/epilepsy carrying mutations in the CACNA1A or ATP1A2 or SCN1A genes, we present here a detailed picture of the frequency and location of each mutation, as well as of the penetrance of epilepsy within the families (Table 4).
Patients with F/SHME1 were mostly sporadic cases (66.6%), while the penetrance of epilepsy in the few familial cases was very high (60%), thus suggesting a strong correlation between specific mutations and the onset of epileptic discharge. Specifically, with the exceptions of S218L, F363S and W1684R, the other seven CACNA1A variants were associated with seizure/epilepsy (7/10, 70%) and were localized in the transmembrane domains (S1–S6). Moreover, patients with F/SHM1 were more likely to develop epilepsy when the mutation modified positively charged amino acids in the III or the IV S4/S5 domains, whereas no missense mutation affecting the first two S4 segments of the Cav2.1 channel (encoded by the CACNA1A gene) resulted in being associated with seizures/epilepsy. Accordingly, Beyl et al. (45) reported that neutralization of gating charges in the I and II S4 transmembrane domains of the Cav1.2 calcium channel (encoded by the CACNA1C gene) only slightly affect the equilibrium constant of voltage sensor transition. Therefore, F/SHM1 patients harbouring a missense mutation lying in the III or the IV S4/S5 domains appear to be more susceptible to developing epilepsy and therein need to be closely followed up and managed for this higher risk. The mechanisms underlying this genetic susceptibility can be hypothesized on the basis of the functional and animal studies conducted to date. To this regard, studies in heterologous expression systems have reported that the mutations associated with FHM1 lead to an enhanced single channel Ca2+ influx also for mild depolarizations, indicating an increased channel open probability due to a shift to lower voltages of channel activation (6). Notably, compared with the other FHM1 mutations, S218L (the most frequent mutation among FHME1 patients) produces the largest shift of activation and the largest gain-of-function of human Cav2.1 channels, especially in the case of small depolarization (1,6,46). Furthermore, S218L knockin mice have shown a unique increased susceptibility to repetitive successive cortical spreading depression (CSD) events, following a single CSD-inducing stimulus (6,47,48). This particularly low CSD threshold and the strong tendency to respond with multiple CSD events may in fact cause the severe neurological phenotype, and could also be involved in an increased susceptibility to seizures (49). In support of this hypothesis, recent research suggests that repeated CSD activity is able to lower the seizure threshold or induce increased excitability, therein promoting a change into epileptic status in isolated normal or injured (traumatic or perinfarctual) brains (49,50). This also might explain the underlying mechanisms of the other mutations associated with FHME1.
The association of CACNA1A mutations with ataxia is explained by the relevant role of Cav2.1 channels in the cerebellum for the maintenance of the highly regular, intrinsic, pacemaking of Purkinjie cells (PCs). The disruption of the pacemaking of PCs can be the result of either gain or loss-of-function mutations (51). Episodic Ataxia type 2 (EA2) is a disease that starts in childhood or early adolescence (age range 2–32 years) and is characterized by paroxysmal attacks of ataxia, vertigo, and nausea, typically lasting hours to days. EA2 patients usually have truncating CACNA1A mutations, but some of these can have missense mutations such as G1483R, F1491S, V1494I, R1662H, and R1665Q. Interestingly, these missense variants lie mostly in the III and IV S4, S5 or S6 transmembrane domains (51), where the FHME1 mutations are also mainly localized. The functional consequences of EA2 missense mutations have been investigated by expressing the channels in either mammalian cells or oocytes, and a clear dominant negative effect of these mutants was revealed (51). Therefore, it is not possible to exclude a dominant negative effect also for the missense mutations leading to FHME1. Overall, it appears that FHME1 mutations generate an intermediate phenotype through a gain-of-function and/or dominant negative effect, in a continuum clinical spectrum between HM and EA2 where the clinical connecting point is the ataxia. In fact, ataxia is consistent in EA2, present in 51.7% of FHME1 patients, while rare or completely absent in FHM1. Mutations associated with F/SHME1 had a worse prognostic value, as the percentage of severe cases (HM, epilepsy, ataxia, ID) was high (37%) (Table 4). Clinically, the epilepsy was refereed as generalized, focal or post-traumatic (in patients with the S218L mutation) and only in one case was a GEFS+ phenotype reported.
Patients with F/SHME2 were mostly familial cases (85.5%), where the penetrance of epilepsy was quite high (30.9%), suggesting a rather strong effect of some specific mutations in the generation of epileptic discharge. Moreover, regarding the genotype-phenotype correlation, our review evidenced that 73.3% of mutations affecting the transmembrane domains were associated with epilepsy, thus patients carrying such mutations could be much more susceptible to developing epilepsy compared to those having mutations outside the transmembrane domains, for whom this risk appears to be lower (31%). Missense mutations affecting the transmembrane domains can lead to both the perturbation of catalytic site functions and the modification of pump kinetic characteristics (1,2,15,19). Specifically, malfunctioning of the Na+, K+-ATPase pump may lead to neuronal hyperexcitability, which facilitates paroxysmal depolarizing shift (PDS) or CSD, causing seizures or migraine, respectively (1,2,19). This malfunctioning can occur due to three synergistic events: An elevation of extracellular K+ levels, an accumulation of glutamate in the synaptic cleft, or an increase in intracellular Ca2+ concentrations (15). Clinically speaking, epilepsy has been described mainly as generalized and in some cases triggered by fever. The severe cases, which were very rare among FHM2 patients, were instead more frequent (11.3%) among patients with F/SHME2 (Table 4).
Finally, regarding 852 SCN1A variants, these have been described in association with different phenotypes (GEFS+, Dravet syndrome, FHM3, febrile seizures), which can affect the entire protein structures in the intracellular, extracellular and transmembrane domains. Patients with FHME3 were all familial cases, and the penetrance of epilepsy was 33.3%, a value that is lower than expected for a gene whose mutations are strongly associated with epilepsy. The genotype-phenotype correlation in these cases seemed to be highly dependent on the functional effect of the mutation, rather than their positions in the canal proteins. In fact, mutations leading to loss of function were more commonly associated with severe phenotype (Dravet syndrome), whereas gain-of-function mutations were usually associated with either GEFS+ or FHM3, as they were milder phenotypes (3,5,9). In the case of FHM3 experimental evidence, it suggested that a single mutation can have double functional effects. In fact, Cestele et al. (10), applying a genetic and functional approach, studied a family having the T1174S (c.3521 C > G) SCN1A mutation associated with seizure and/or HM, reporting that this variant induced divergent functional effects, loss of function or gain of function, a finding consistent with both epilepsy and HM phenotypes, respectively. However, to date, the T1174S variant should not be considered a proven mutation causing disease. In fact, its clinical effect is still uncertain: Its frequency in polymorphism databases is 0.27% (European population), and it was not predicted to be damaging by the majority of prediction tools. On the other hand, the T1174S variant appears to be enriched in patients with epilepsy and/or FHM, compared to its frequency in the general population, and therefore might have a reduced penetrance, as one recent study suggested (52). Clinically, epilepsy was described as generalized, focal, partial with secondary generalization, and in some families febrile seizures were reported. Compared with FHME1 and FHME2 individually, the prognosis for FHME3 was not worse, as there were no severe cases or patients with other relevant complications among this subgroup.
Therapeutic implications
The efficacies of antiepileptic drugs (AEDs) in migraine and epilepsy have been reported to be mediated by interactions involved at multiple sites. In fact, these AED targets have more molecular sites in the brain, which are able to alter either voltage-operated ion channels or ligand-gated channels (53–55). Among the drugs widely used for epilepsy, topiramate is the most effective for migraine when compared with valproate and gabapentin, whereas lamotrigine has been reported to be effective for MwA in open studies, but has not been demonstrated to be effective for MwoA (56). The effectiveness of some antiepileptic drugs (topiramate, valproate and lamotrigine) and other migraine prophylactic drugs for CSD threshold have been evaluated only in different animal studies (57,58), so the therapeutic effect of these drugs in migraine patients is not clear. Other relevant targets for migraine pathophysiology could also be effective in migraine but, even in this case, evidence has derived only from animal models, and therein these findings cannot be extrapolated to humans (59–61).
Sodium valproate has been reported to reduce HM attacks, epileptic seizures and severe FHM attacks in patients suffering from both conditions (18), while evidence regarding the efficacy of topiramate is limited in HM (62) whereas lamotrigine has been reported to improve MwA in open-label studies, but not for MwoA in controlled trials vs a placebo or vs an active drug (63). This drug has a proven suppressive effect on CSD, which could explain its selective action on MwA (58). To date, the choice of preventive therapeutic strategies for HM has been based upon recommendations for common migraine, employing empirical strategies formulated on a limited number of FHM case reports. Conversely, AEDs including phenytoin, oxcarbazepine and vigabatrin block voltage-gated sodium channels and GABAergic transmissions, thereby reducing hyperexcitability mechanisms, but they are inefficacious in migraine (64). Despite these limitations with AEDs, the use of some anticonvulsivants, considered efficacious for both migraine and epilepsy, could be reasonable choices for treatment for HM and complex phenotypes, particularly HM and epilepsy. The evidence regarding the use of AEDs in literature is scarce. Therefore, clinicians should consider prescribing AEDs to HM patients having mutations associated with a marked susceptibility to developing epilepsy, instead of other anti-migraine drugs.
Conclusion
This review found that, in HM, mutations associated with seizure/epilepsy are not only frequent in S/FHM3 (44.4%) and S/FHM2 (40.9%) but also in S/FHM1 (33.3%), where in the latter the penetrance of epilepsy had the highest value (60%). Moreover, regarding the genotype-phenotype correlation, F/SHME1 and F/SHME2 had mutational hot spots at the protein levels. In fact, we observed prevalent and statistically significant involvement of the transmembrane domains for S/FHME1 (70%) and S/FHME2 (41%). In the former condition, the strongest genotype-phenotype correlation was observed when positively charged amino acids were involved in the S4 segments, while in the latter condition about 73% of mutations affecting the transmembrane domains were associated with seizure/epilepsy. These findings provide a better understanding of the pathological mechanisms underlying migraine and epilepsy and, if confirmed, these results would necessitate the recognition of an F/SHME subgroup.
Footnotes
Clinical implications
In hemiplegic migraine, the relative number of mutations associated with seizure/epilepsy was elevated not only for ATP1A2 and SCN1A genes, but also for the CACNA1A gene, where the penetrance of epilepsy for the latter had the highest value (60%).
Concerning F/SHM-Epilepsy1 (F/SHME1) and F/SHME2 endophenotypes, we observed a prevalent involvement of the transmembrane domains, and a strong genotype-phenotype correlation in F/SHME1 when the positively charged amino acids were involved.
The few SCN1A mutations associated with HM and epilepsy (FHME3) all belonged to familial cases. These genotype-phenotype correlations seem to depend on the functional effects of the mutations rather than their positions in the canal proteins.
Our results suggest the presence of mutational hot spots at the protein levels rather than a genotype-phenotype correlation at least for FHME1 and FHME2.
Author contributions
Conception/design: PP, CC, CP, SP. Collection and/or assembly of data: CS, PP, BC. Data analysis and interpretation: PP, CS, CC, SP. Manuscript writing: PP, CC, CML, CP, SP; Figures and tables: CC, CS, PP, CP. Revisions of manuscript: PP, CC, BC, CML, CP, CS, and SP. All authors provided important intellectual content and critically revised the final version of the manuscript.
Acknowledgement
We thank Dr Saviz Yaghmai for his precious support in preparing the illustration.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PC receives/received research support from Biogen, Lundbeck, Merck-Serono, Sanofi-Aventis and UCB Pharma. He also receives/received support from Ricerca Corrente and Ricerca Finalizzata IRCCS Fondazione Santa Lucia. All other authors report no disclosures. This study is not industry-sponsored.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.